This policy does not merely try to sideline programs like DACA through bureaucratic maneuvering. It goes much further. For those affected inside the United States, it effectively collapses the INA itself, nullifying nearly every meaningful legal pathway.
It reaches across almost the entire immigration system, including:
★ H-1B petitions, including extensions and changes of employer or status
★ O-1 visas for individuals of extraordinary ability
★ J-1 physician-related pathways, including follow-on employment and related dependent benefits
★ EB-1A extraordinary ability petitions
★ EB-1B petitions for outstanding professors and researchers
★ EB-1C petitions for multinational managers and executives
★ EB-2 National Interest Waiver petitions
★ EB-2 Physician National Interest Waiver petitions
★ Family-based cases, including petitions involving spouses, parents, and immediate relatives of U.S. citizens where the beneficiary is from a covered country
★ Adjustment of Status (I-485) applications filed inside the United States, regardless of the underlying category
★ Work permits tied to pending Adjustment of Status, including (c)(9) EADs
★ Advance Parole and travel documents tied to pending adjustment cases
★ Deferred action-related work permits
★ J-2 spouse EADs
★ H-4 spouse EADs
★ TPS-based EADs
★ F-1 related extensions and changes of status
★ OPT-related benefits connected to F-1 status
★ Asylum-related benefits that were swept in under the earlier December memorandum,
Under PM-602-0192 and PM-602-0194, USCIS does not merely blur the line between legal and illegal. It erases it. The policy operates regardless of lawful presence, immigration category, years of compliance with the law, or length of legal stay.
Because it is triggered by nationality, citizenship, or country-of-birth criteria, it cuts across the entire system and harms even U.S. citizens in practical terms by blocking petitions for their spouses, parents, and immediate relatives.
In effect, it turns lawful process into a trap: follow the rules, file through the proper channels, wait your turn, pay the fees and still end up stranded in limbo, lose employment, pushed into a gray zone, and exposed to detention or removal. Punished solely for where you were born.
It was implemented abruptly, without notice and without any meaningful opportunity for affected individuals to adjust their affairs or revise plans made in reasonable reliance on the prior legal framework. Worse still, it was applied retroactively to applications that had been properly filed years earlier.
It takes people from entirely different legal categories and treats birthplace as if it were a disqualifying offense. Physician, professor, spouse of a U.S. citizen, student, highly skilled worker, or undocumented person, all are funneled toward the same end: attrition, de-legalization, and exclusion.
At its core, this is the logic of exclusion by identity or origin, more reminiscent of Idi Amin or the Alhambra Decree than of any modern legal system. More regressive than the Code of Hammurabi (c. 1754 BC). How is this even legal?
#LiftTheHold #LiftThePause #PM6020192
#PM6020194 #UscisPause
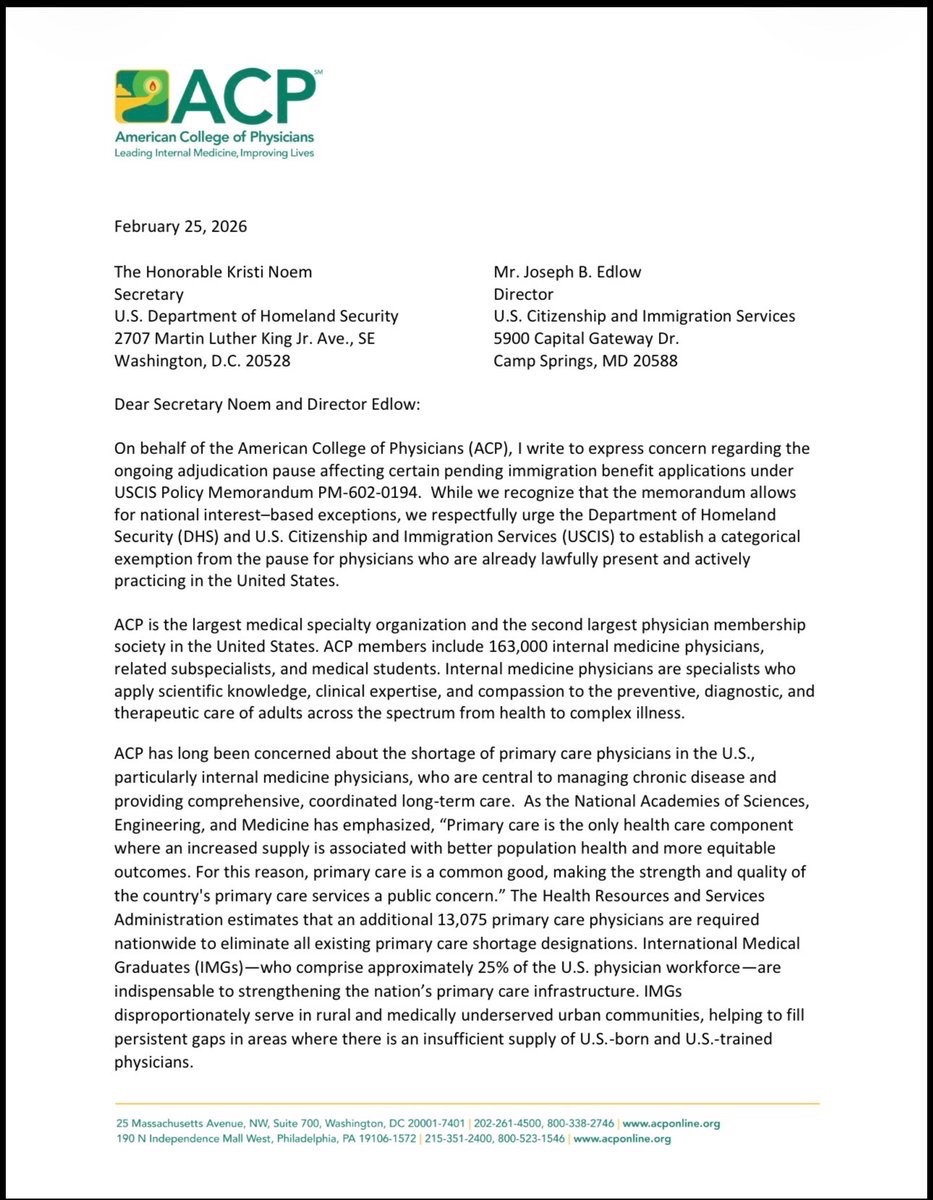
We thank @ACPIMPhysicians for standing up and advocating for the thousands of physicians affected by the USCIS pause.
Since December, US-trained doctors born in 39 designated countries have effectively been blocked from every legal pathway to remain lawfully in the US and continue caring for patients: no visa extensions, no work permits, no green cards, and no path to citizenship, despite doing everything right and giving years of service to the US healthcare system.
These are not new applicants trying to enter the system. They are doctors already here who completed residency and fellowship in the US, are board-certified in their primary specialty, and are already caring for American patients. Many serve in rural and underserved communities, where losing even one physician can be devastating.
After years of training and service, their careers are being brought to a halt for one reason alone: their country of birth. Yet almost no one knows this is happening. Media coverage has been minimal, and organizational advocacy has been scarce.
ACP was among the first to recognize the gravity of this issue. This is not just an immigration matter. It is a patient care crisis unfolding in plain sight.
@ACPIMPhysicians@AmerMedicalAssn@Cardiology@Cardiology@AANmember@AAMCtoday@ProjectImg@ReichlinMelnick
https://t.co/pv3axFpeSy
Now that everyone is an expert on curing pancreatic cancer in mice, not rats - I want to add some context that goes beyond the headline.
You will want to read this.
Cancer is cured in mice all the time.
Thousands of times. ~90% of those “cures” fail in humans.
Why?
Because mice are:
Genetically simpler.
Treated earlier.
Short-lived.
Not humans.
Mice are a filter - not a finish line.
Yes, this study matters. It comes from the Spanish National Cancer Research Centre.
Yes, it’s pancreatic cancer - one of the deadliest there is. Yes, full tumor regression is impressive.
But here’s what it actually means:
“This approach is now good enough to risk years, trials, and millions of euros on.”
Not:
“Cancer is solved.”
What happens next?
More animal work.
Toxicology.
Phase I (safety).
Phase II (maybe works).
Phase III (beats standard care?).
Maybe 8-10 years if everything goes right.
The real damage isn’t failed drugs.
It’s failed expectations.
Every “cured cancer in mice” headline trains the public to believe:
Cures are being hidden.
Progress should be fast.
Scientists are lying when reality hits.
That’s how trust erodes.
Bottom line:
This is how real cancer progress looks.
Messy. Slow. Risky. Incremental.
Not miracles.
Not conspiracies.
Just science - doing the hard work.
🚨 Why Thousands of Doctors in the U.S. Will Soon Stop Seeing Patients
This is not getting media attention. Since December 2025, there has been a little-known internal freeze and indefinite hold affecting immigrant and non-immigrant applications for people born in, or citizens of, 39 countries. This applies even if someone has lived in the U.S. for decades, trained here, paid taxes, and is legally working right now.
What does this mean in real life?
About 25% of U.S. doctors are foreign-born. Many come to the U.S. and complete 3 to 8 years of rigorous residency and fellowship training to become fully licensed to practice independently. These training positions are based in teaching hospitals and supported by public funding streams, including Medicare.
Under this freeze, many doctors born in countries such as Iran, Nigeria, Syria, Sudan, Cuba, Venezuela, and others may be unable to renew or change work visas, obtain work permits, or move forward with green cards or citizenship.
This is not an entry ban. It affects people already inside the United States, including many who have been here for more than a decade.
There is no reliable workaround.
If a doctor’s current work authorization expires, they must stop working immediately. They cannot see patients, finish residency or fellowship, or start jobs they already signed contracts for.
This is not theoretical. It is already happening.
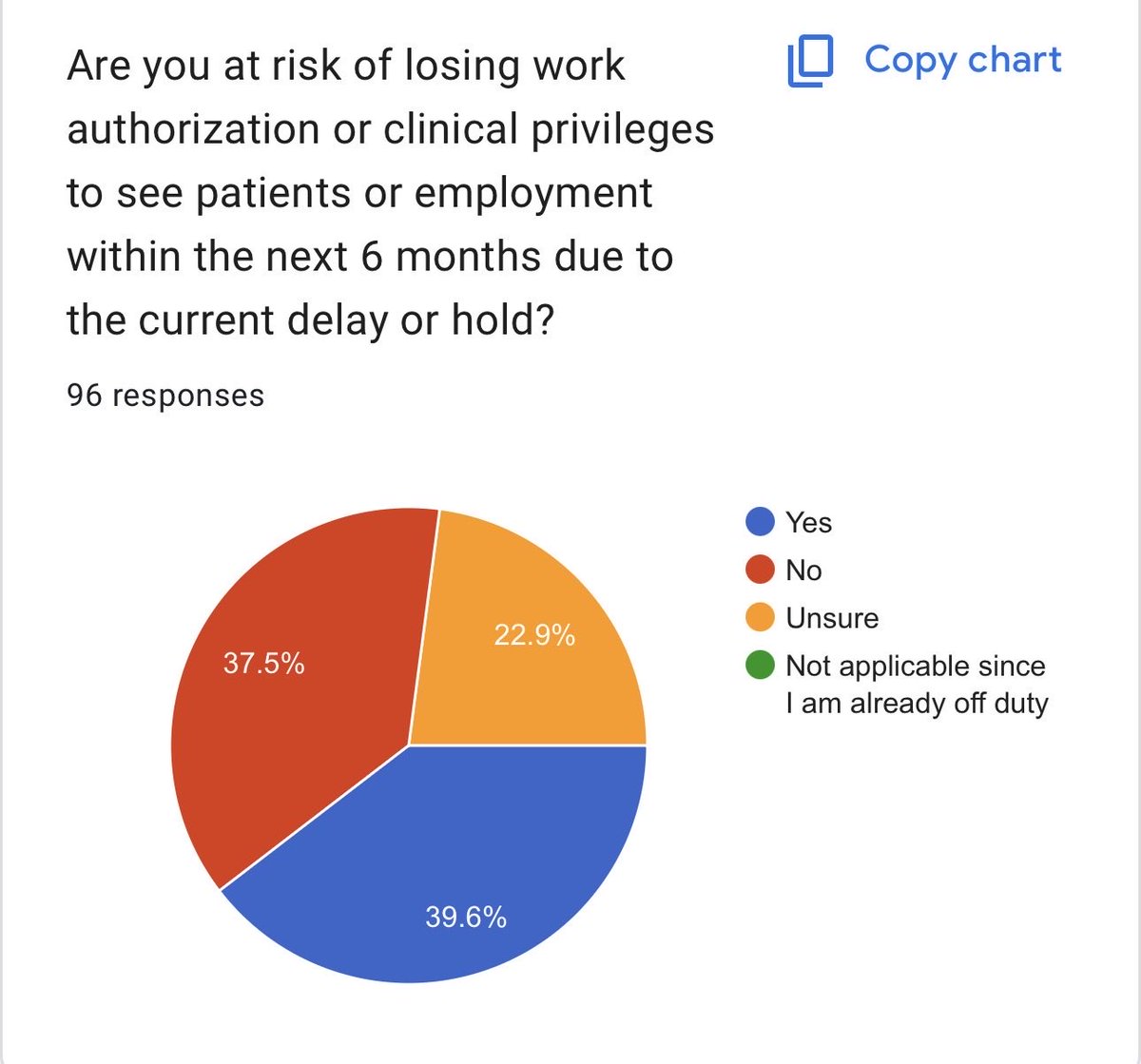
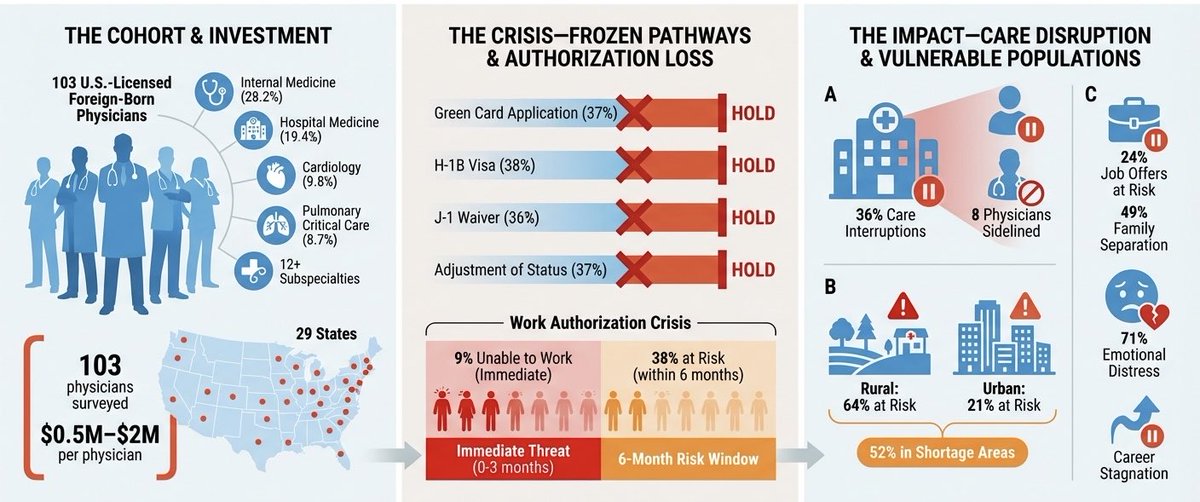
We surveyed 103 U.S.-trained physicians directly affected by this freeze:
•9% have already lost their residency positions or jobs and have stopped seeing patients.
•39% expect to be forced to stop seeing patients within the next 6 months, or expect to be unable to start jobs they already signed for after graduating from residency or fellowship.
•The average physician in our survey has been working in the U.S. for 4 to 7 years.
Many of these physicians are board-certified or board-eligible, working in hospitals, clinics, and training programs across the country.
When a doctor is suddenly removed, patients lose continuity of care, clinics scramble to cover shifts, and residency programs lose trainees mid-year.
This disproportionately affects rural and underserved communities, where many of these physicians work and where replacements are hardest to find. In our respondents, 53% of attendings work in rural settings. Many reported they are the only vascular surgeon or interventional cardiologist covering multiple counties.
What makes this more concerning is that many hospitals, professional societies, and policymakers may not realize this freeze exists, because it is not a public ban or a court order. It is happening quietly. Over the last two months, we are not aware of any physician who has been granted an exception, even when patient care is clearly impacted.
This is not about politics. It is about patient care and workforce stability. These are physicians already here, already licensed, and already caring for American patients. They have been vetted by state licensing boards, hospitals, and credentialing systems. 10% of our respondents work in VA hospitals caring for veterans. These include oncologists, cardiologists, surgeons, and ICU physicians nationwide.
Removing these physicians after years of U.S.-based training and integration is not a smart allocation of taxpayer investment and directly undermines workforce stability and patient access to care.
Patient care is already being disrupted. Without urgent action or a clear exception pathway, the loss of physicians will accelerate.
Summary of the survey results is below.
Pneumopexy After Open Right Upper Lobe Lobectomy
This incredible video from @elkamel__ demonstrates the surgical technique of pneumopexy to prevent lung torsion after open right upper lobectomy in a patient with adenocarcinoma.
🔗https://t.co/tS0NkdvBEa
#thoracic#lung
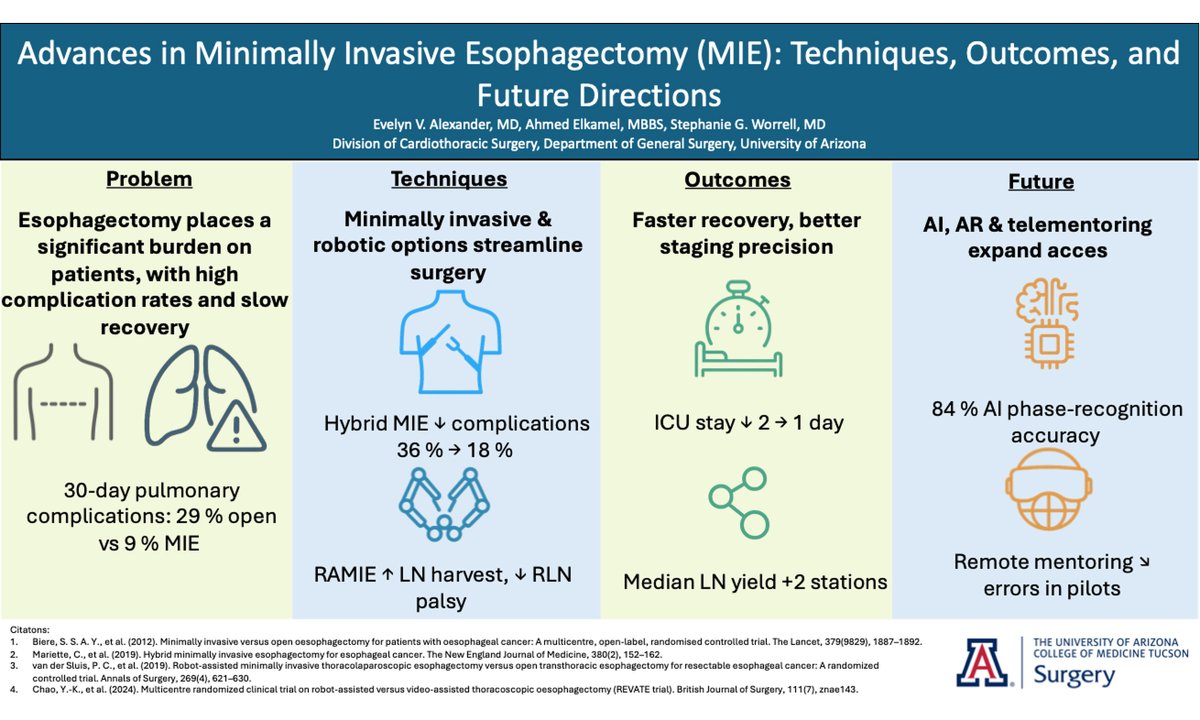
🚨 New in Mini-invasive Surgery!
🔬 Advances in Minimally Invasive Esophagectomy (MIE)
By Evelyn V. Alexander, Ahmed Elkamel & Stephanie G. Worrell
✅ Robotic precision
✅ REVATE & ROBOT-2 trials
✅ AI & telementoring shaping the future
🔗 https://t.co/RsDen46C9X
Does surgical residency really need to be 5 years? 🤔
In our recent study of senior residents, skills improved with PGY—except in Nissen fundoplication, which requires advanced suturing.
Time ≠ mastery. Should we rethink how we train?
📄 https://t.co/U28JhnG0Xc
#MedEd
🌟 113 Future Physicians Matched! 🌟
Despite the ongoing war in Sudan, 113 newly matched residents have shown incredible resilience and determination. Over 95% benefited from SAPA’s support—observerships, interview prep, mentorship, and more.
Congratulations to all who matched—you inspire us! 🎉
Stay tuned as we highlight their stories.
🔹 Join SAPA Academic on Facebook and let’s build success together! https://t.co/M6vSVQA5SL
#Match2025 #MatchDay
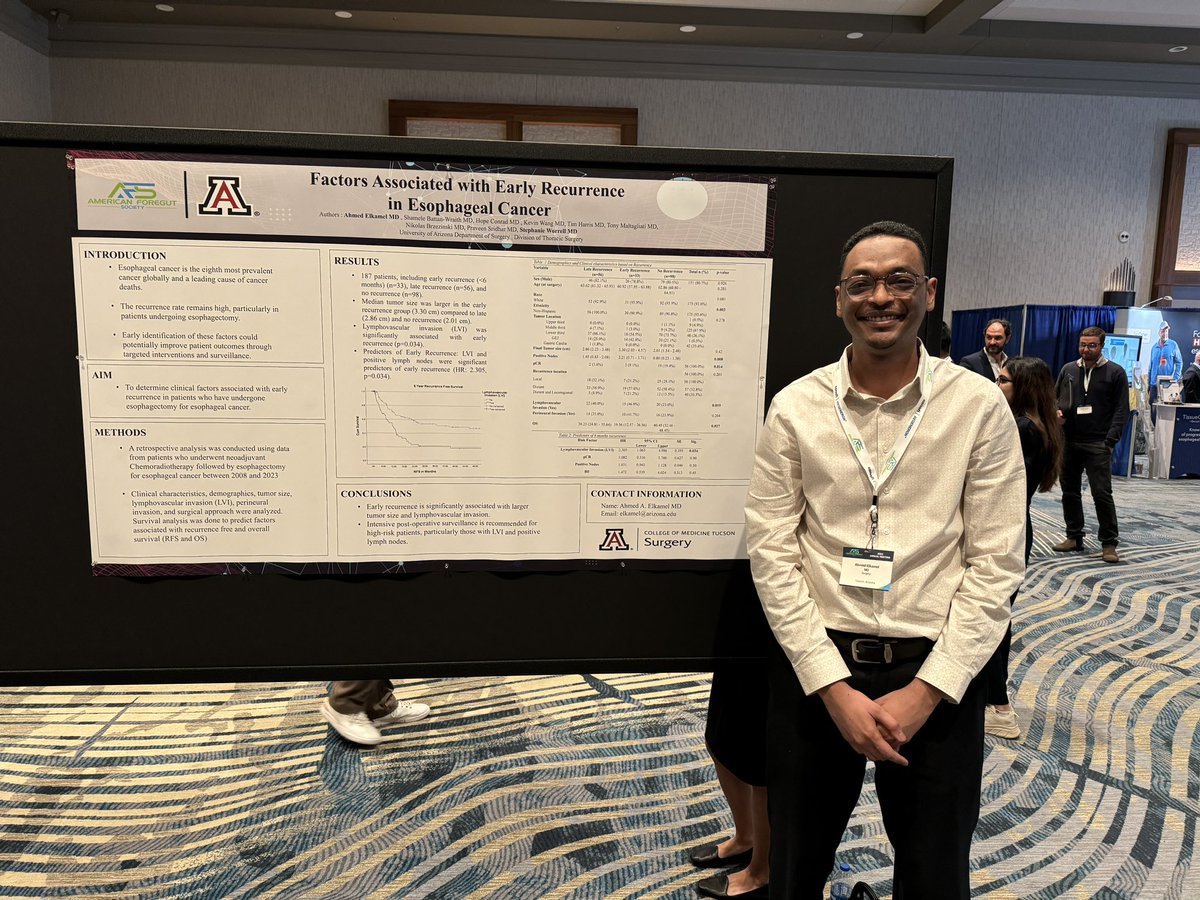
Great representation from @UofAZSurgery at #ASC2025 this year! Proud to be part of such an incredible team pushing the boundaries of surgical research! @AcademicSurgery
We couldn’t be more proud of our incredible General Surgery residents and fellow who represented #UofAZSurgery at the 20th Annual Academic Surgical Congress last week! Take a look at their presentations from #ASC2025 ⬇️
The emerging reports that RSF soldiers poisoned hundreds of Sudanese in the village of Alhilaliya shock the conscience. To poison food in a country already suffering from famine is an especially heinous act. If confirmed, General Hemedti & all of the RSF leadership need to answer for this. Emergency supplies & aid need to get to Alhilaliya right away.
Grateful to be at the STSA cardiothoracic meeting with my mentor @sgworrell and two amazing 4th-year residents @KevinWangMD@TimRHarrisMD1 from the University of Arizona. Honored to learn and grow together in the field of thoracic surgery!
#STSA2024