People who don't follow cancer research often ask me why we haven't cured cancer. That perception masks a wonderful reality: We make amazing, stepwise progress every year, and the result is that many people live much longer today than they would have previously.
Right now we're in the thick of the annual meeting of the American Society of Clinical Oncology, the biggest research meeting on new cancer medicines, and this morning a bunch of really important studies dropped. I'm going to review them here.
This first image is the result for daraxonrasib, a treatment for pancreatic cancer that is generating consdirable excitement. The green line is the probability of living for patients who got the new drug; the gray one is the chemo control group.
If you follow cancer drugs, a chart like this will make your breath hitch a little. I'm going to review these and some other data here.
A warm #ASCO26 welcome to daraxonrasib and RASolute-302 study in 2nd line metPDAC from $RVMD
My story in the post below.
Here are the OS curves you haven't seen yet.
Strong session for #gynonc at #ASCO26.
#RUBY 4-year dMMR data: PFS 57.9% vs 15.7%, HR 0.30 (0.17–0.52). Four new events in 2.5additional years. Cure modeling: 54% curative potential. PFS at 1 year → 91.7%probability still PFS at 3 years. Alive at 1 year → 88.0% probability surviving to 3 years. The plateauis real and it holds.
#NRGGY018 dMMR OS HR 0.56, RUBY 0.66. Not a drug difference -LIKELY poststudy ICI use. 93.2% of GY018 control patients received poststudy ICI vs 70.7% in RUBY. Morerescue in the control arm. Both trials say the same thing: first-line is the only clean window indMMR.I am waiting for KEYNOTE-C93 results to answer: does dMMR EC need the chemotherapy at all?And haven't started addressing POLE!Duration equally unresolved.
The plateau establishes by month 12. Whether 36 months addsanything over 24 in complete remission is untested.
What I do: dostarlimab + CP for dMMR EC.For UCS — dMMR or pMMR — dostarlimab + CP (10% in the RUBY).
@NRGonc@ASCO
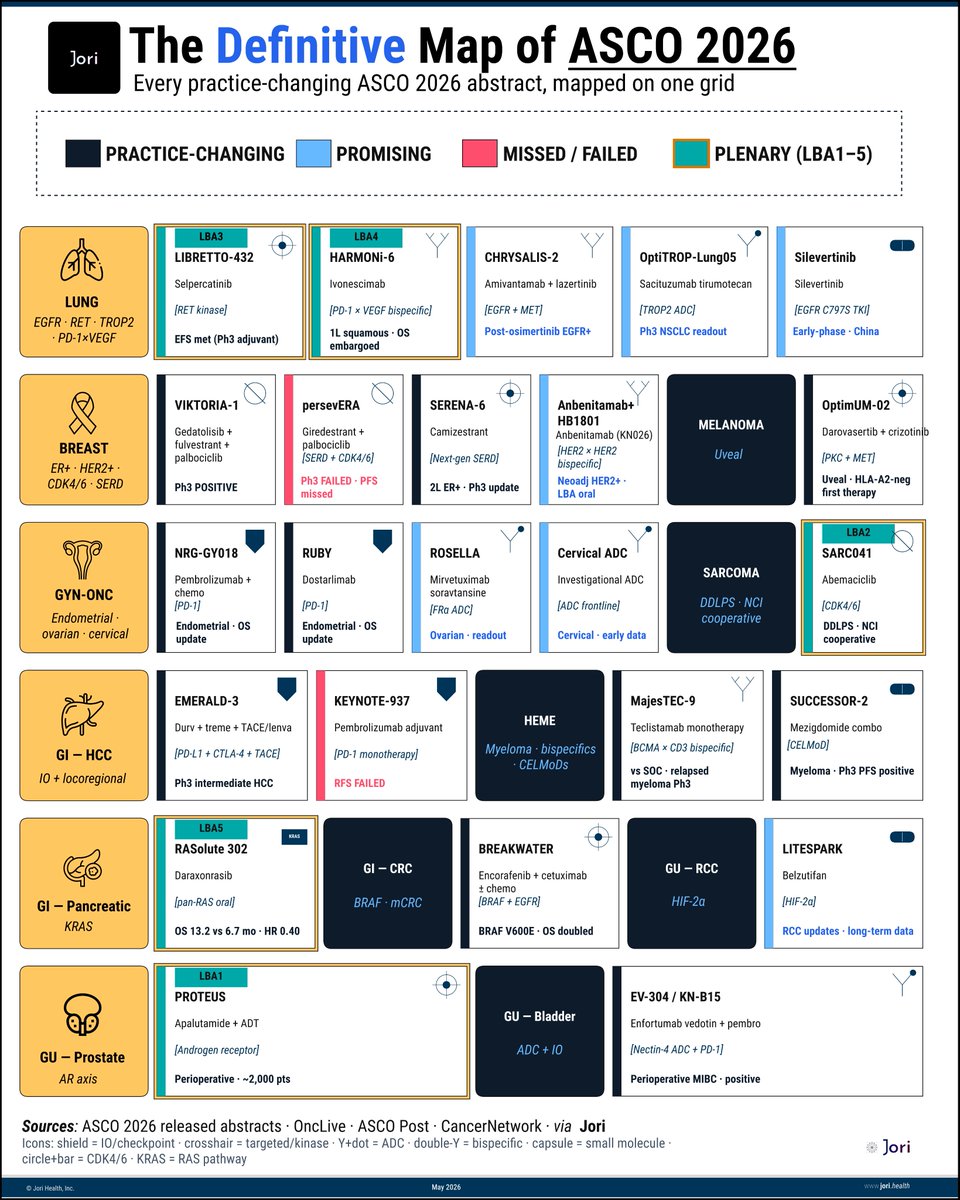
ASCO this year has 5,000+ abstracts.
But maybe 24 will actually change practice. This is that map.
(ERRATA: this plot fixes an error on VICTORIA which reflected incorrect data, thnx @Dr_RShatsky)
Map spans 12 disease areas, 24 critical readouts, 5 plenaries & 2 confirmed misses already on the board.
Few things jump out immediately:
▫️Pancreatic cancer gets the headline.
Daraxonrasib: 13.2 vs 6.7 months.
▫️Sarcoma gets a plenary because public science funded what pharma would not.
▫️Lung cancer remains the most crowded battlefield in oncology:
RET adjuvant, bispecific OS, post-osimertinib, next-gen EGFR.
By next week, some of these cells will become new standards of care.
This is your cheat sheet to keep score in real time.
- - - - -
Sources: @asco@OncLive@CancerNetwrk via @Jori_health
- - - - -
Algorithm for Systemic Therapy in Early HR+/HER2- Breast Cancer
(Recommendations in gray areas reflect my own clinical judgment— eg. olaparib and CDK4/6 sequence)
• In Febrile Neutropenia, the enemy isn’t the most common bug.
• It’s the one that kills first.
• Why we prioritise Gm-neg & anti-pseudomonal cover
• Why Gm pos- isn’t routine
• Why the first 60 minutes matter
👇
#FebrileNeutropenia#Antibiotics#EmergencyMedicine#MVOnco
Sarcomas comprise a heterogeneous group of malignant neoplasms that include genomically simple and genomically complex subtypes. This consensus provides guidelines for efficient, rational use of next-generation sequencing in their clinical management. https://t.co/Z3ojzwWmnT
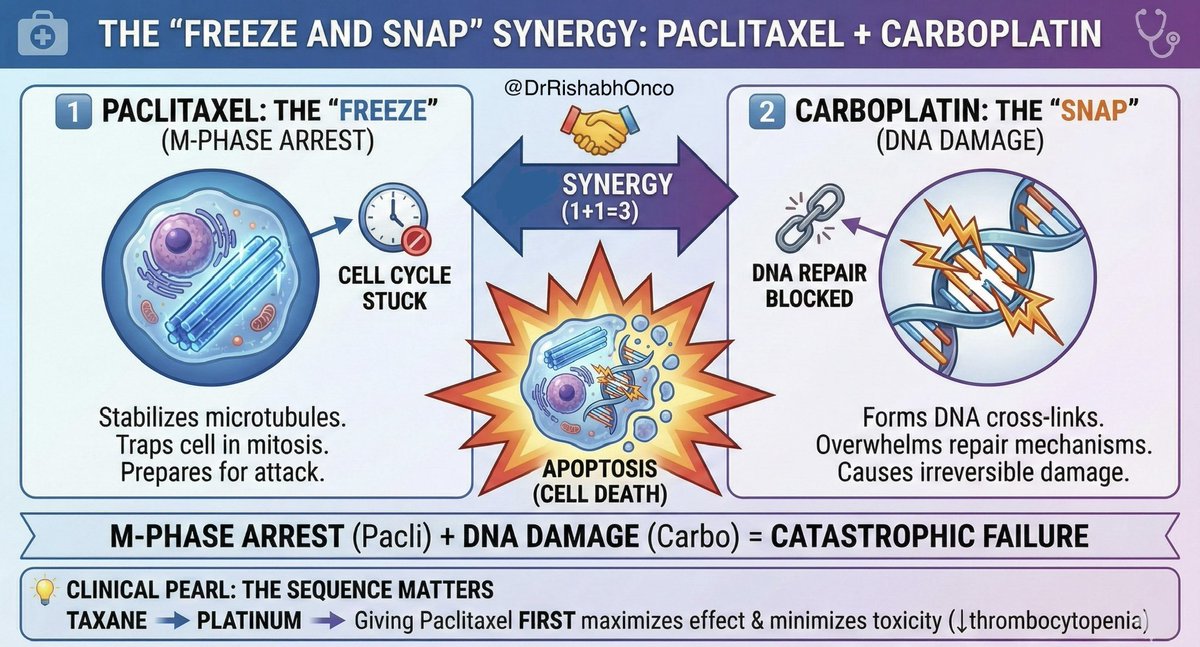
The Paclitaxel + Carboplatin "CarboTaxol" doublet is the bread and butter of oncology for a reason. 🍞🧈
But why does this specific combo work so well?
It’s all about the "Freeze and Snap" synergy. ❄️💥
1️⃣ The Freezer (Paclitaxel):
Paclitaxel stabilizes microtubules, preventing depolymerization.
It freezes the cell’s skeleton in the M-phase (Mitosis). The cell tries to divide but gets stuck. 🛑
2️⃣ The Snap (Carboplatin):
While the cell is arrested and stressed, Carboplatin slides in.
It acts as an alkylating agent, forming reactive platinum complexes that bind to DNA (cross-linking). 🧬🔗
🤝 The Synergy (Why 1+1 = 3):
The magic lies in the timing.
Paclitaxel arrests cells in the G2/M phase.
Cells in this phase are less efficient at repairing the DNA damage caused by Carboplatin.
The "Freeze" prevents the "Repair," leading to accumulation of DNA damage ➡️ Apoptosis (Cell Death). ☠️
💡 Clinical Pearl (The Sequence Matters):
This is why we often administer Taxane before Platinum.
Giving Paclitaxel first avoids the antagonistic effect where Carboplatin might inhibit the uptake or cytotoxicity of the taxane.
It also reduces thrombocytopenia! 📉🩸
#Oncology #MedTwitter #OncTwitter
@OncoAlert@myesmo@esmo_open@asco
🫁 Sequential therapy for advanced/metastatic #EGFRm#NSCLC 🫁
🫁 I’ve compiled it into a table. (PFS & OS only)
🌟 As of October 2025
🌟 I will update after #ESMO25#lungcancer#nsclc#egfr#LCSM
No better news to start the week. In TROPION-Breast02, 1L datopotamab deruxtecan improved PFS & OS over chemo for IO-ineligible pts with metastatic TNBC. ADCs keep delivering & are rapidly climbing to earlier lines. Hope to see the full results at #ESMO25. https://t.co/Hh0vJ8lhF4
This was on expected lines . Tdx1 is better and more effective ADC as compared to TdM1. It is more toxic also. It will be intresting to see rates of Grade 4-5 ILD and magnitude of benifit. Also if benifit is more in those with significant residual disease vs only small residual disease . Looking forward to full data at @myESMO #esmo2025
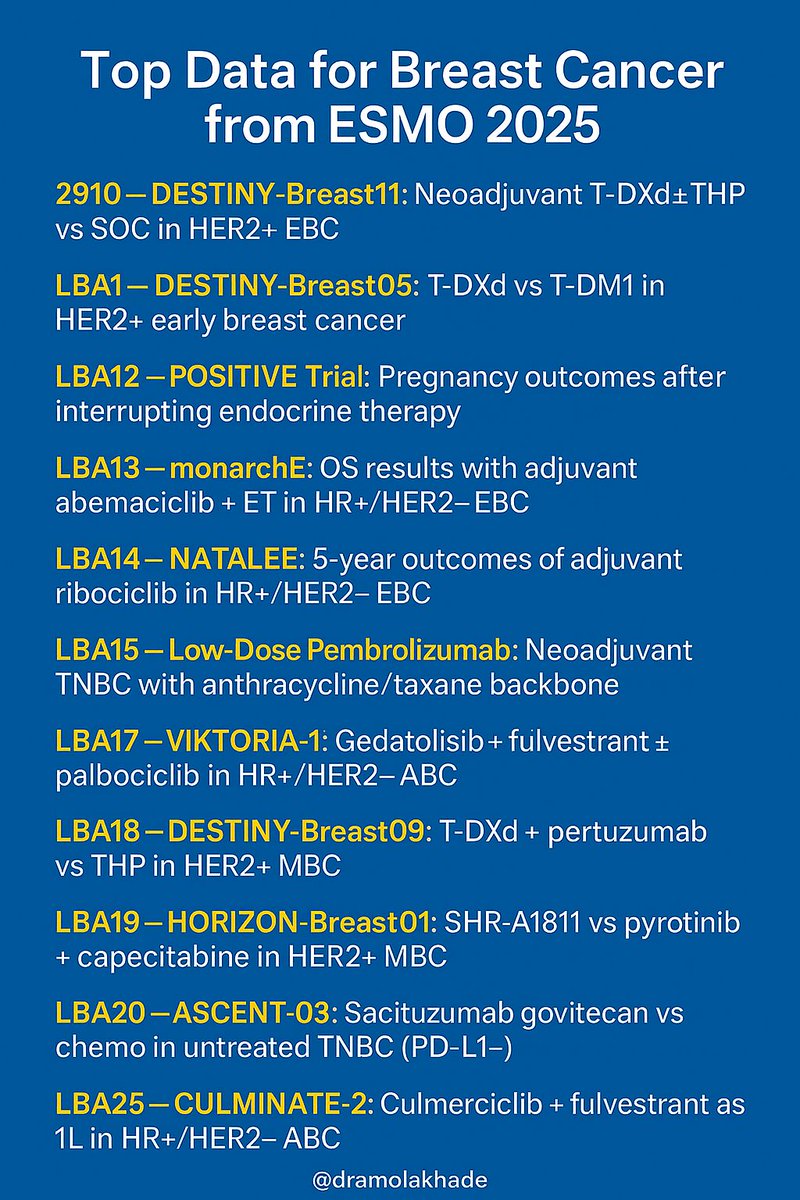
🚨 Top Breast Cancer Data – #ESMO25 🚨
From early to metastatic settings, 13 key trials shaping practice:
✅ DESTINY-Breast11, Breast05, Breast09
✅ monarchE, NATALEE, POSITIVE
✅ ASCENT-03, VIKTORIA-1, OptiTROP-Breast02, CULMINATE-2 & more @myESMO
#esmo2025 @On@OncoAlert@OncBrothers
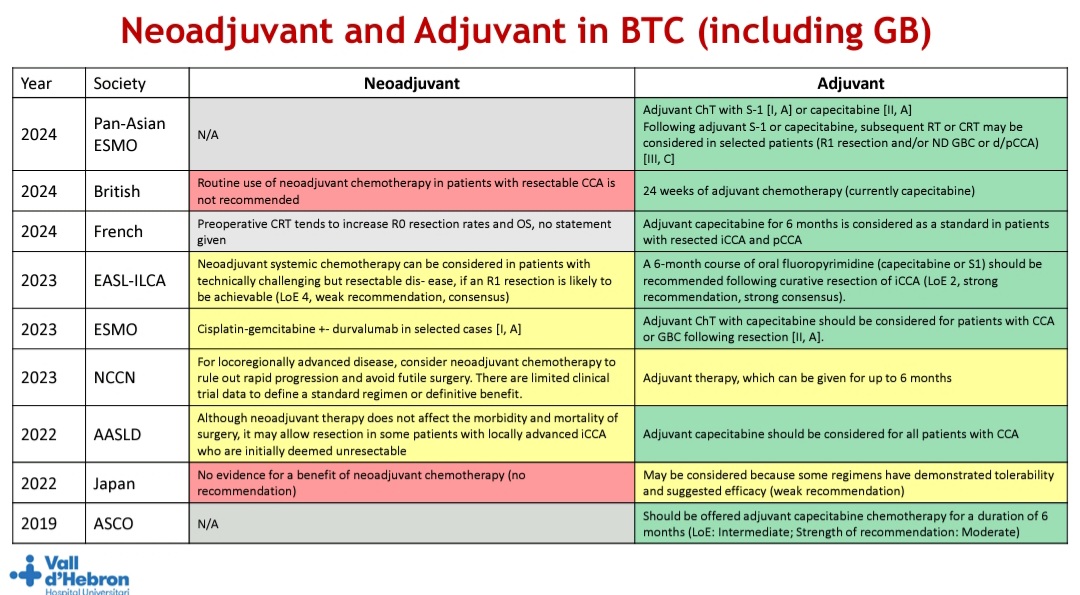
Nice slide to show evolution of various gudilelines over the years for Neoadjuvant and Adjuvant therapy in BTC ( including GB )
From educational session by Dr Gonzalo @myESMO#ESMOGI2025