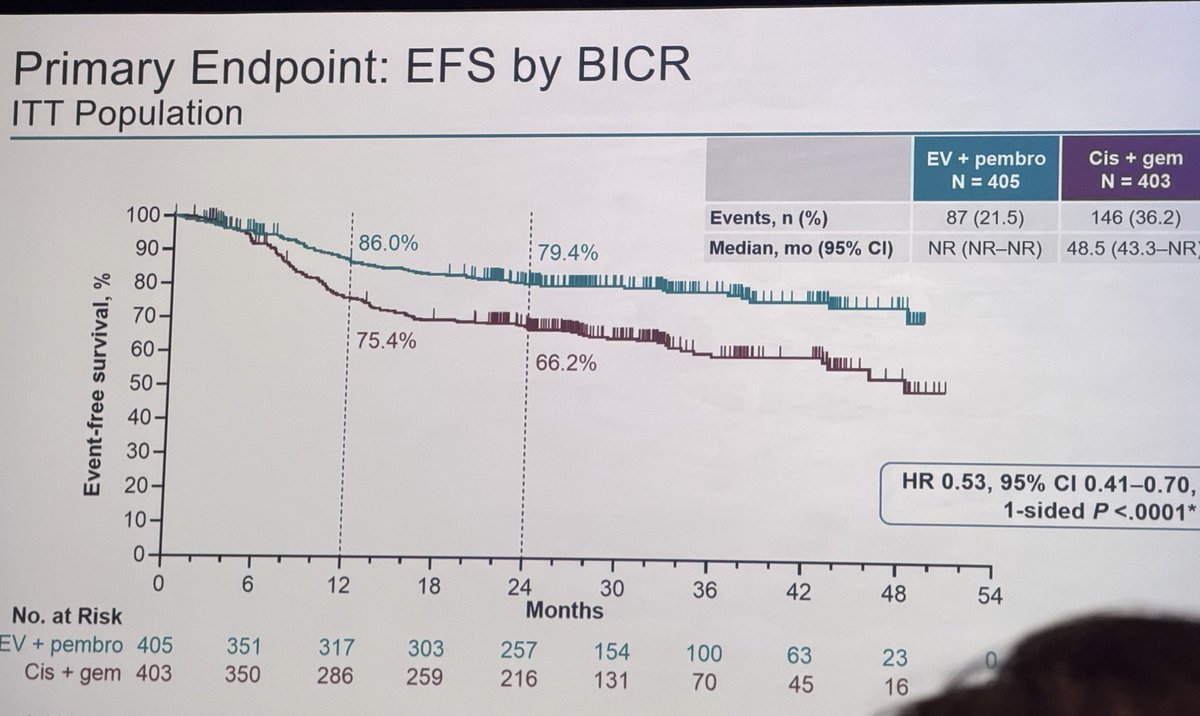
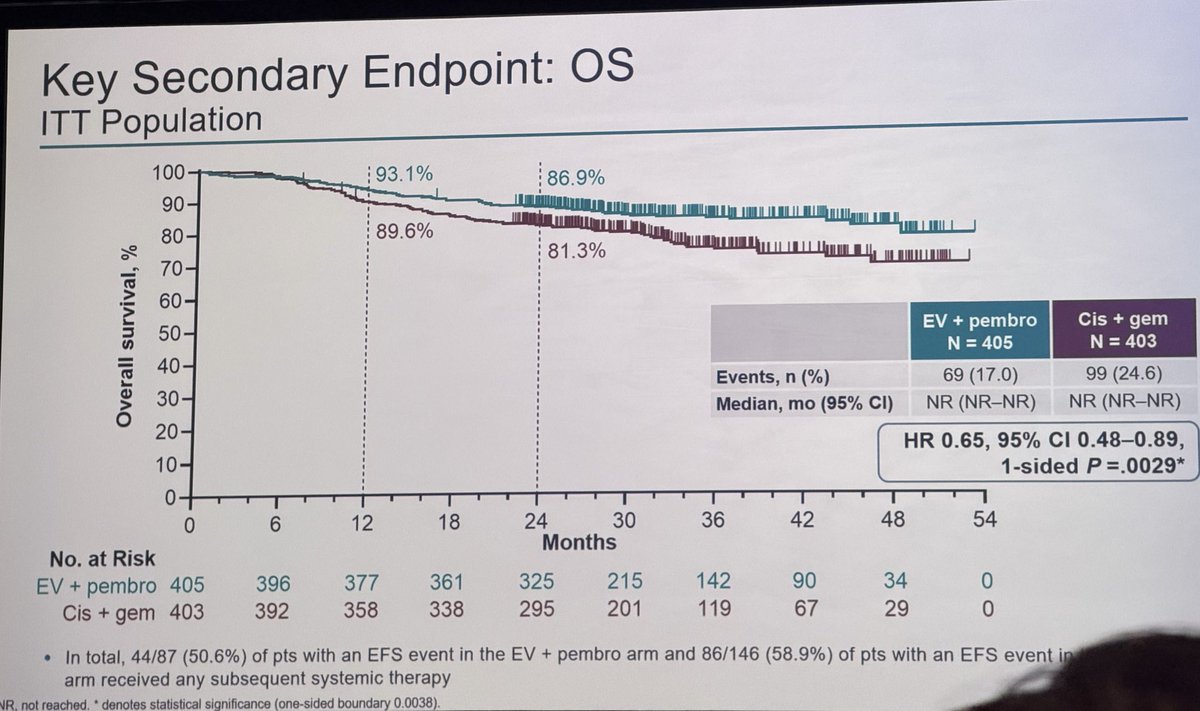
PRACTICE CHANGING: #KEYNOTEB15/EV304- in #MIBC, periop EV/P led to sig EFS (NR v 48.5m, 24m EFS 79.4 v 66.2%, HR0.53; 0.41-0.7), OS (NR v NR, 24m estimated OS 86.9 v 81.3%, HR 0.65; 0.48-0.89), pCR (55.8 v 32.5%) benefit v. neoadj gem/cis, supporting EV/P as SOC in this setting
A decade of work comes to fruition. Better care for our patients with high risk prostate cancer. Both primary endpoints positive. Congrats to the entire team and recognition to all our patients who participated @MGHUrology@MassGenBrigham@MGBUrology@DanaFarber_GU
Presented at #ASCO26:
In high-risk localized prostate cancer, ADT plus apalutamide led to a pathological complete response or minimal residual disease and 5-year metastasis-free survival in a greater percentage of patients than ADT plus placebo. Full phase 3 PROTEUS trial results: https://t.co/UxXUkYwd8Z
Editorial: A Watershed Moment in the Perioperative Treatment of Prostate Cancer https://t.co/XgeWL3lqy6
@ASCO
@DrYukselUrun not just radical cystectomy hopefully all “bladder sparing (?) radical therapies” which clearly effect bladder dynamics & quality of life issues
Kongremiz 17–21 Kasım 2027 tarihleri arasında Regnum Carya Otel, Antalya’da gerçekleştirilecektir.
Mesleki gelişim, bilgi paylaşımı ve bilimsel etkileşimin ön planda olacağı bu kongrede sizleri aramızda görmekten onur duyacağız.
#Üroonkoloji#ÜroonkolojiKongresi#Bilim
🔥 POISE-3 Urology published in European Urology 🚨
In the largest randomized placebo-controlled #urology analysis of #TranexamicAcid (TXA), #TXA reduced major #bleeding risk by 37% (from 9.5% to 6.1%) with no clear increase in #thrombosis
More at https://t.co/Yypy7vb9Jz
#EBM
Neoadjuvant Chemotherapy for High-risk Localized Upper Tract Urothelial Carcinoma: Final Long-term Outcomes from a Phase 2 Clinical Trial and an Expanded Cohort - European Urology https://t.co/UlOKYibQGC
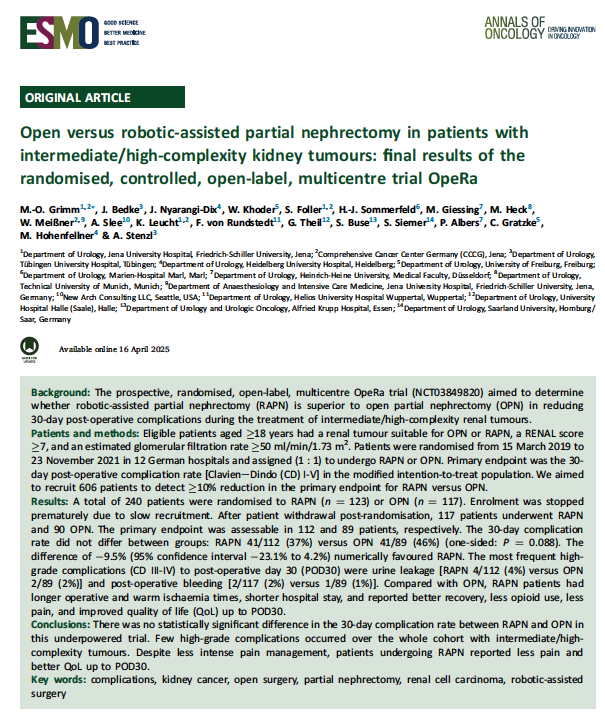
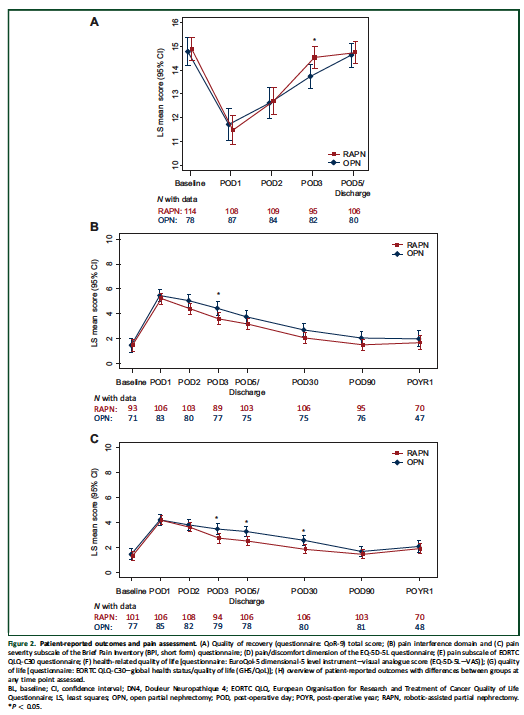
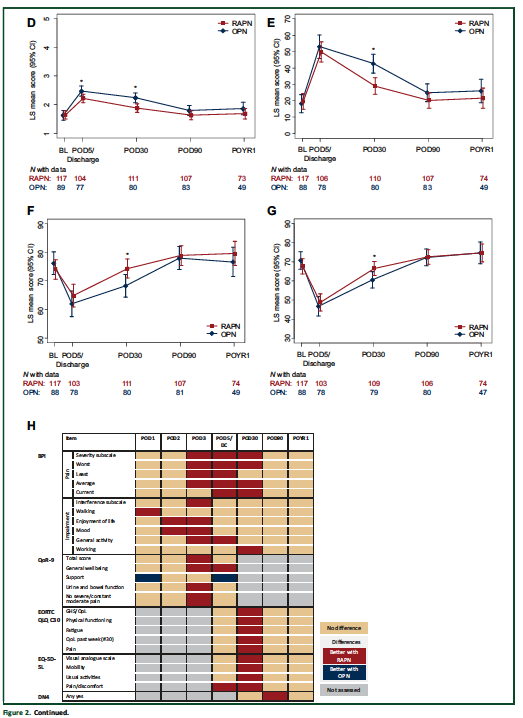
🤖🆚🗡️ Robotic vs open partial nephrectomy for complex kidney tumors
👏Tested in an RCT (OpeRa trial)
@Annals_Oncology
🔑🔑 Takeaways:
⚖️ 30-day complications: no significant difference (RAPN 37% vs OPN 46%)
⏱️ RAPN = longer OR + warm ischemia time
🏥 RAPN = shorter hospital stay
💊 Less opioids, less pain
😊 Better QoL through POD30
⭐️ RAPN not clearly safer, but easier on patients in the short term — even for intermediate/high-complexity tumors
🔗https://t.co/bVnRZKb8yt
@urotoday@renalandurology@UrologyTimes
⚡️ @EurUrolOncol: Regional node–positive bladder cancer (cN+) is heterogeneous and still lacks phase III evidence.
Retrospective series support multimodal management: cisplatin-based induction chemotherapy plus consolidative RC, with best outcomes when ypN0 is achieved.
#BladderCancer @OncoAlert
https://t.co/HePnUf53a1
⚡️ Bladder preservation after neoadjuvant therapy in MIBC: we’re not yet ready to replace radical cystectomy.
No phase 3 noninferiority data, heterogeneous protocols.
For now, a strategy for carefully selected pts in expert centres.
#BladderCancer
https://t.co/w3wLBgesyn
I really think we should embrace this concept! The combination of a good surgery (ERBT) and a good adjuvant treatment (E.g. BCG) is crucial to cure patients with NMIBC, even for those with high-risk diseases! We are getting there!!
Remains one of the cheapest/easiest ways to minimize unnecessary testing, biopsy, diagnosis, or treatment: repeat a newly elevated PSA (without empiric abx)
https://t.co/7kF7p2vOio
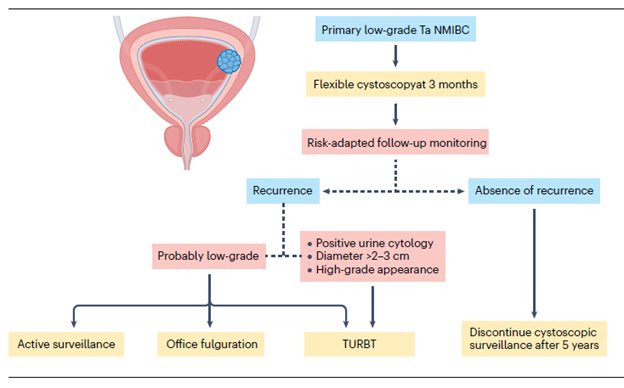
“Low-grade Non–Muscle-Invasive Bladder Cancer: Molecular Landscape, Treatment Strategies, and Emerging Therapies” - just published in Nature Reviews Urology @NatRevUrol. This State-of-the-Art review by Drs. Roger Li @UrogerliMD, Lexi Wen, and colleagues @philippespiess@spsutkaMD@LDyrskjot@DrShariat@UroDocAsh offer an outstanding overview of advances in molecular biology, diagnosis, targeted therapies, and clinical management for #bladdercancer. A great honor to be part of this effort.
Summary:
The management of low-grade non–muscle-invasive bladder cancer (NMIBC) is undergoing rapid evolution, driven by a growing recognition of the need for nuanced, risk-adapted strategies that minimize overtreatment. Yet widespread adoption of de-escalated approaches remains limited by the lack of well-defined, evidence-based guidelines tailored to this favorable-prognosis disease subset. Clear recommendations - particularly regarding surveillance frequency, duration, and criteria for de-intensified care - will likely require international consensus efforts supported by robust prospective data.
A major priority for future research is refining risk stratification. Distinguishing patients at truly increased risk of progression from those with indolent disease will enable more personalized management, including appropriate use of active surveillance and reduced surveillance intensity. Advances in molecular profiling, urine-based biomarkers, and AI-assisted pathology show promise for identifying meaningful biomarkers and histologic patterns to support such stratification, but rigorous prospective validation remains essential before broad clinical adoption.
AI integration into clinical workflows offers additional opportunities to enhance diagnostic accuracy, predict recurrence or progression, and support individualized decision-making. Multimodal models capable of real-time risk assessment may eventually guide therapy selection, but challenges - including the need for diverse training datasets, transparent algorithms, and clear ethical and regulatory frameworks - must be addressed before routine clinical use.
Despite favorable overall outcomes, managing low-grade NMIBC remains challenging owing to high recurrence rates and continued reliance on invasive cystoscopy and imperfect biomarkers. Until emerging diagnostic tools are validated, established clinicopathological systems such as the IBCG risk stratification model will continue to guide treatment decisions. Patients with multiple risk factors generally warrant intravesical therapy, while those without risk factors may be reasonable candidates for active surveillance. The ongoing BCG shortage further underscores the need to balance clinical benefit with treatment burden and to evaluate new intravesical therapies against their potential financial and clinical toxicity.
Meaningful progress in low-grade NMIBC will depend on prospective validation of emerging technologies and therapies, paired with thoughtful integration into evidence-based guidelines. By aligning molecular insights, technological innovation, and risk-adapted clinical practice, the field can improve outcomes while reducing unnecessary interventions and surveillance for this common, yet often overtreated, disease.
The article is available at the following link:
https://t.co/Hkzge1HLDo
New data show radiotherapy can induce amphiregulin, reprogram myeloid cells, and support distant tumour growth. Understanding this may help us design better treatment paths for patients. @Nature@OncoAlert
https://t.co/yhM0nUzrPK
For men with prostate cancer treated with radiation therapy, what is the ideal duration of hormone therapy?
Intermediate risk: <6 months
High risk: ~12 months
(For most)
The longer the hormones, the less death from prostate cancer, but more death from heart attack, stroke, etc.
⚡️ Bladder preservation after neoadjuvant therapy in MIBC: this review cautions we’re not ready to replace radical cystectomy.
No phase 3 noninferiority data and heterogeneous protocols.
An evolving option for carefully selected pts in expert centers.
#BladderCancer@emanuele_crupi@AndreaNecchi
https://t.co/zjEWff7HHs