Health literacy is not “just education”
In inflammatory arthritis, lower ability to find, understand &use health information is linked to worse physical, mental, treatment &work outcomes
This matters in IBD too
Evidence-based online education can empower patients and support better shared decision-making
https://t.co/ohNKKzJDmi
@TheLancet@LancetGastroHep
🩺 Cirrhosis is no longer just a “liver disease.”
This review summarizes how inpatient cirrhosis management has fundamentally evolved from static “end stage liver disease care” into dynamic risk stratification and organ support.
One of the most important modern concepts highlighted:
⚠️ “Cirrhosis” is increasingly being replaced by the concept of compensated advanced chronic liver disease (cACLD).
A particularly important ICU and ward management point:
🩸 Variceal bleeding management has changed.
Modern evidence supports:
• restrictive transfusion strategy
• early vasoactive therapy
• early antibiotics
• rapid endoscopy
• selective early TIPS in high risk patients
One major physiological misconception continues to harm patients:
❌ Elevated INR in cirrhosis does NOT equal auto anticoagulation.
Cirrhosis creates a “rebalanced” coagulation state where patients can simultaneously:
• bleed
AND
• thrombosis
This explains why routine FFP correction before paracentesis is no longer recommended and why portal vein thrombosis remains common.
Another critical update:
💧 Ascites management is not simply “give diuretics.”
The review reinforces that:
• sodium restriction is foundational
• albumin remains physiologically crucial
• aggressive fluid shifts can precipitate renal collapse
• diagnostic paracentesis should be routine in hospitalized patients with ascites, even without symptoms
Perhaps one of the most important modern concepts:
🧠 Hepatic encephalopathy is not merely “high ammonia.”
The article emphasizes:
• systemic inflammation
• infection triggers
• electrolyte disturbances
• medications
• renal dysfunction
• gut microbiome interactions
as central drivers of encephalopathy.
And importantly:
🍖 Protein restriction is now contraindicated.
This is a major paradigm shift from older teaching.
Patients with cirrhosis require:
• aggressive nutritional support
• high protein intake
• sarcopenia prevention
• late night protein supplementation
One of the strongest messages of the paper:
⚠️ Every hospitalization for decompensated cirrhosis should trigger transplant thinking.
Not “end stage management.”
Not passive stabilization.
But active reassessment of:
• prognosis
• reversibility
• candidacy
• goals of care
• frailty
• transplant referral timing
For intensivists and hospitalists, cirrhosis management is increasingly becoming a discipline of: • hemodynamic physiology
• renal protection
• inflammation control
• nutritional optimization
• procedural timing
• multidisciplinary coordination
rather than isolated hepatology alone.
📖 Rogal S. Inpatient Management of Patients With Cirrhosis. Annals of Internal Medicine. 2026. doi:10.7326/ANNALS-26-00513
PEI is common, frequently unrecognised – and not a 'pancreas-only problem.' New 'Mistakes in…' article unpacks the key clinical pitfalls: from overinterpreting faecal elastase results to insufficient nutritional assessment.
Full article on Gutflix 🔗 https://t.co/j3uvPrRWko
📊 JAMA Clinical Guidelines Synopsis: #CrohnDisease guidelines recommend fecal calprotectin for screening and monitoring, routine colonoscopy for colorectal cancer, and oral budesonide for induction in mild to moderate ileocecal disease.
https://t.co/s9czp8Szkn
Join us for a live, patient-centered recap of #CCC2026! Hear insights from patient reporters Ian Goldstein & Victoria Tyler, and IBD experts @KrugCleveland & @AdamFayeMD.
Presented in partnership with @CrohnsColitisFn.
📅 Feb. 26, 2026
⏰ 8–9 p.m. ET
🔗 https://t.co/Th07B6TWtG
This review highlights the expanding role of JAK inhibitors in managing extra‑intestinal manifestations of IBD, including joint and skin involvement, while noting the need for more targeted evidence. #JAKinhibitors#IBDEIMs#GIResearch#Clinicalresearch https://t.co/YafeVRenBB
🧵 Can past response to steroids predict future response in patients with UC?
We tried to answer a question clinicians face every day—but that has surprisingly little data behind it
New research - Efficacy and safety of subcutaneous guselkumab induction therapy in participants with moderately to severely active ulcerative colitis (ASTRO): a double-blind, treat-through, randomised, placebo-controlled, phase 3 trial
https://t.co/WhBmg8MWfW
#GITwitter
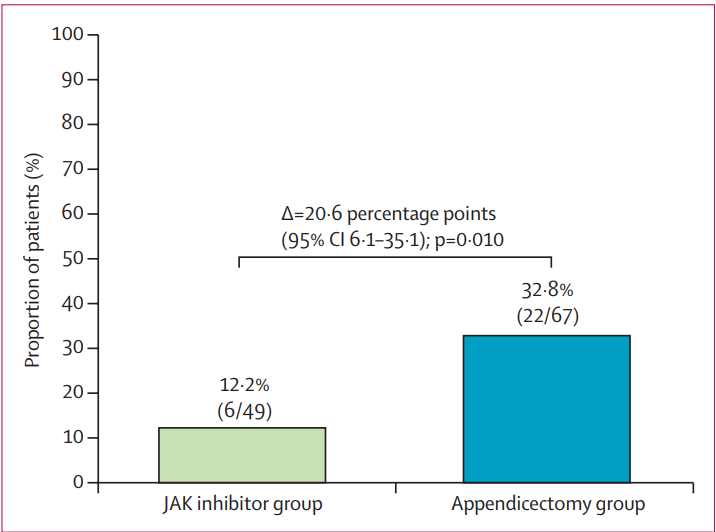
❗️Appendectomy was found to be superior to switching to a JAK inhibitor among patients with active ulcerative colitis exposed to advanced therapies. Higher clinical response, clinical remission, steroid-free remission, and endoscopic response.
https://t.co/xVGOAyV3Nj
One more thing.
We have received another FDA IND clearance and have initiated Phase 1 for ENV-6946, bringing our total to three first-in-class, novel, nature-inspired molecules in the clinic.
ENV-6946 is an oral small molecule engineered for the potential to treat inflammatory bowel disease, designed as a “multi-biologic in a pill.” It simultaneously targets TNFα, IL-23, and TL1A signaling in the gut without requiring separate injectable therapies.
Millions of people live with IBD, with far too few efficacious, safe, durable, and convenient options available. ENV-6946 represents a new path forward – one designed for efficacy, safety, and simplicity.
With ENV-294, ENV-308, and now ENV-6946 in clinical development, we continue to demonstrate:
• The ingenuity of nature
• The power of our platform
• The pace and commitment of our team
Onward.
Read more: https://t.co/GH04ifkwyb
This week is Crohn’s & Colitis Awareness Week.
🟣 Nearly 3M Americans live with IBD conditions, often invisible but certainly life-changing.
🟣Join Duke GI in raising awareness & supporting all affected.
💜 #IBDAwareness#IBDLooksLike#CrohnsAndColitisAwarenessWeek#IBDVisible