@VickersBiostats@DrSpratticus@DrYukselUrun@ChapinMD It didn’t seem that the evidence was convincing enough https://t.co/vGB085CIjW see @gu_onc episode about a year ago ! Surgical RCTs are not easy to perform, but sometimes it may be even harder to convince surgeons to change practice.
A decade of work comes to fruition. Better care for our patients with high risk prostate cancer. Both primary endpoints positive. Congrats to the entire team and recognition to all our patients who participated @MGHUrology@MassGenBrigham@MGBUrology@DanaFarber_GU
Presented at #ASCO26:
In high-risk localized prostate cancer, ADT plus apalutamide led to a pathological complete response or minimal residual disease and 5-year metastasis-free survival in a greater percentage of patients than ADT plus placebo. Full phase 3 PROTEUS trial results: https://t.co/UxXUkYwd8Z
Editorial: A Watershed Moment in the Perioperative Treatment of Prostate Cancer https://t.co/XgeWL3lqy6
@ASCO
2/ ctDNA testing in @NHS-Galleri screening study did yield more diagnoses of stage 1 or 2 cancers, especially colorectal cancer (important to note that US has far more colon cancer screening than does UK, which may be contibutor here).
Which trial are you watching most closely? #ASCO26
For me: RCC biomarkers, perioperative EV+pembro in MIBC, and whether PROTEUS changes the treatment paradigm in high-risk localised prostate cancer.
My Top 10 GU cancer trials to watch at #ASCO26 — RCC first, then urothelial/bladder, then prostate.
Key themes: adjuvant intensification, ctDNA/MRD, perioperative IO/ADC, and biomarker-selected therapy.
Abstract links below 🧵
#GUOncology#UroSoMe
Where is urologic oncology heading next?
Excited about the upcoming #UROFAIR26 Oncology Programme, as we bring together colleagues across Asia and beyond!
Outstanding regional & international faculty joining us this July in Singapore! 🇸🇬
#Urology#UroOnc
@jimhumd@DrSpratticus Great overview — perhaps PROTEUS could also be considered here, given its potential implications for perioperative management of high-risk localized prostate cancer. https://t.co/VqofjbR2Rw
Where is urologic oncology heading next?
Robotics 🤖
Precision imaging 🧠
Systemic therapy integration 💊
Organ preservation 🫶
Advanced disease surgery ⚔️
Excited for the #UROFAIR26 Oncology Plenary in Singapore 🇸🇬
Outstanding regional & international faculty joining!
Optimizing Ureteral Stent Changes: A Hybrid Approach ✅
Publishing our experience with a risk-stratified model for ureteral stent changes: Outpatient (Local Anesthesia) and Operating Room (GA/MAC).
High success rates with good classification.
https://t.co/dL6ScC08KN
https://t.co/Yy5h3BKLpt
10.1007/s00345-026-06360-x
@steffiyuen@endouro@DocGauhar@jleow@TheodorosTokas@Shkohsg@wjurol@asiaendouro@PEARLSendouro
No doubt @RoyalFreeNHS Specialist Centre for Kidney Cancer runs one of THE BEST robotic urology fellowship programs in the UK!! 🇬🇧 @FHMUMTAZ@2frcsurol Axel Bex
🤖High volume
✂️Complex robotic, lap & open upper urinary tract surgeries
🧬 Malignant & benign conditions !!
so incredibly proud of these superstars!
a group of supremely talented surgeons that we have had the pleasure of training at the specialist centre for kidney cancer @RoyalFreeNHS
so much joy at our alumni dinner at #EAU26
UK/ Ireland/ Saudi/ Singapore/ Aus
in the house 💪🏽
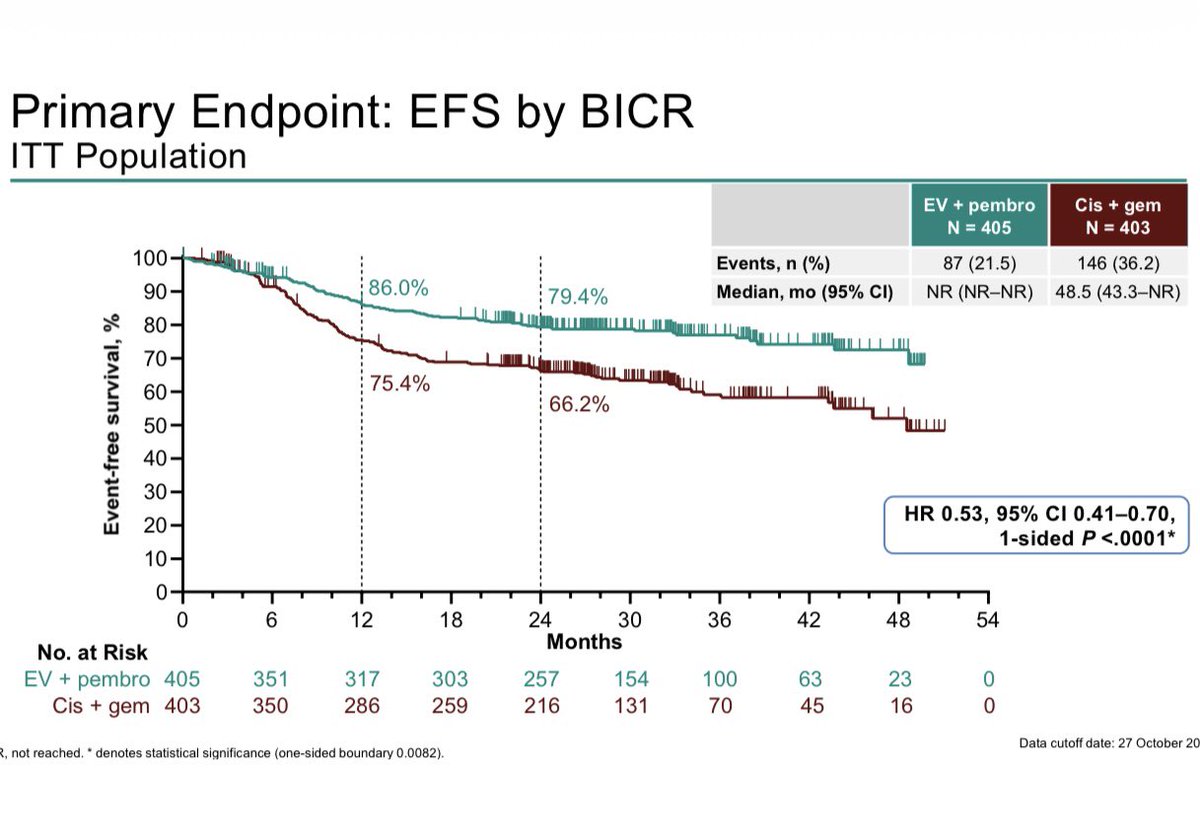
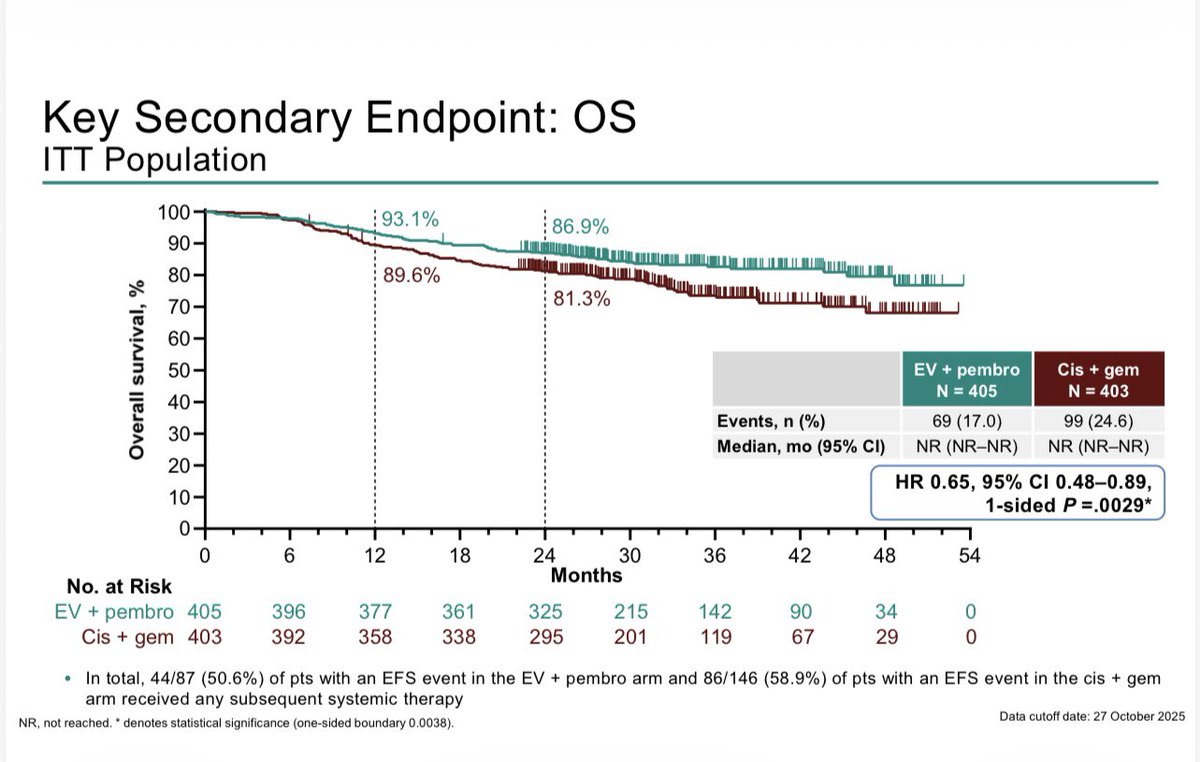
KN-B15/EV303: R3 Perioperative EVP vs Gem/cis in MIBC shows EFS HR 0.53 (0.41–0.70), OS HR 0.65 (0.48-0.89), pCR 56% vs 33%, G3+ tox 76% vs 67% #GU26. About half the patients completed 9 cycles of EVP. These are great results. Gem/cid is harder to beat when not all patients are at risk of relapse. Bladder sparing approaches for cCR (~60%) will be where this ends. ‘EVP 1st, ask questions later’. These studies are needed soon.
Ready for ASCO GU.
Every trial is a promise. Behind names like LITESPARK, PEACE or NIAGARA, there is a person waiting for a normal Tuesday. We turn data into time. Science is the bridge, but hope is the destination.
@ASCO@OncoAlert@ONCOassist@OncLive#Cancer