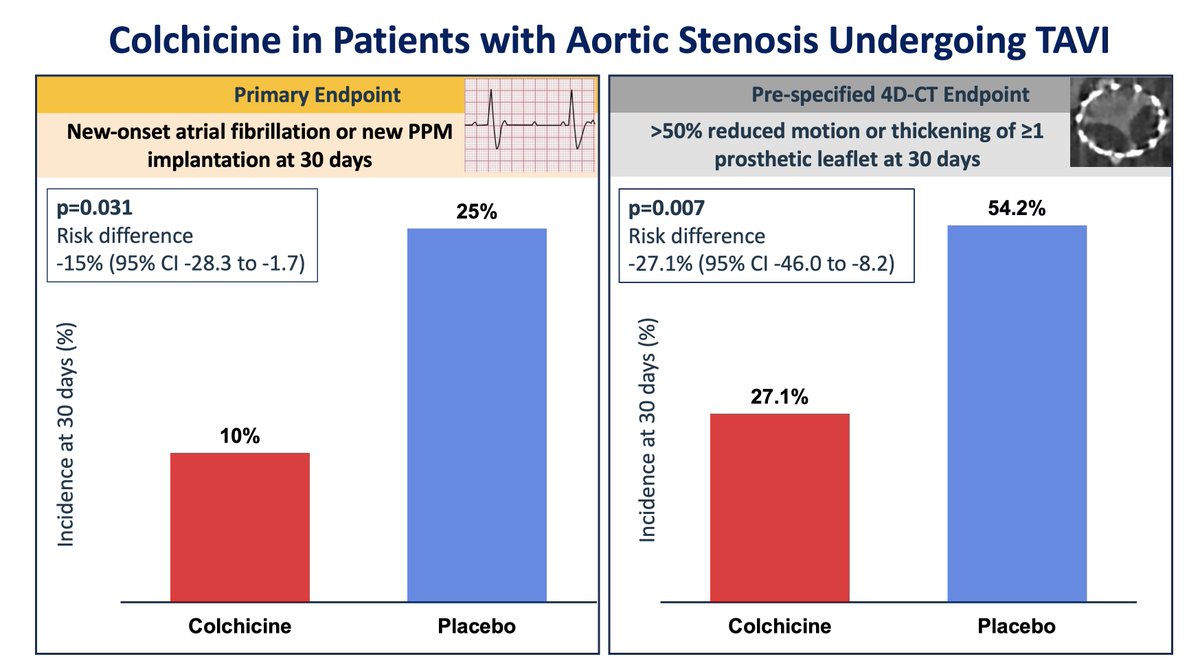
In this RCT in TAVI patients, treatment with colchicine was associated with a lower risk of new-onset rhythm disturbances and subclinical leaflet thrombosis compared with placebo. The inflammatory response to TAVI may represent a novel therapeutic target. https://t.co/rCqbpCTgfN
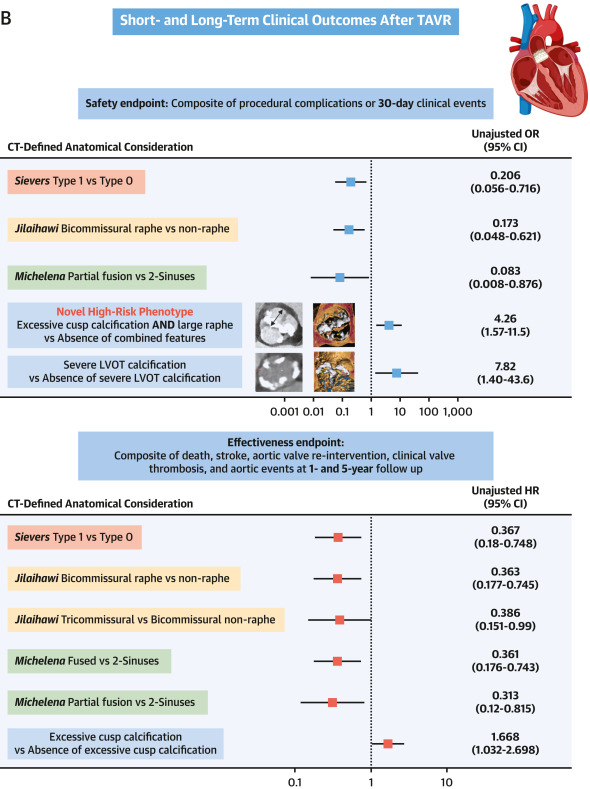
Bicuspid anatomy can pose a significant challenge for TAVI: the combination of a substantial AVC calcium burden and a prominent raphe may define a particularly high risk phenotype. #JACCImaging https://t.co/aLxFXb7x44
❗Not all #bicuspid aortic valves (BAVs) behave similarly after #TAVI
⚠️ New high-risk phenotype identified: heavy cusp calcification + large raphe = >4× more periprocedural complications. @JACCJournals@ACCinTouch
check-out 👇
https://t.co/YbYhJZGCh0
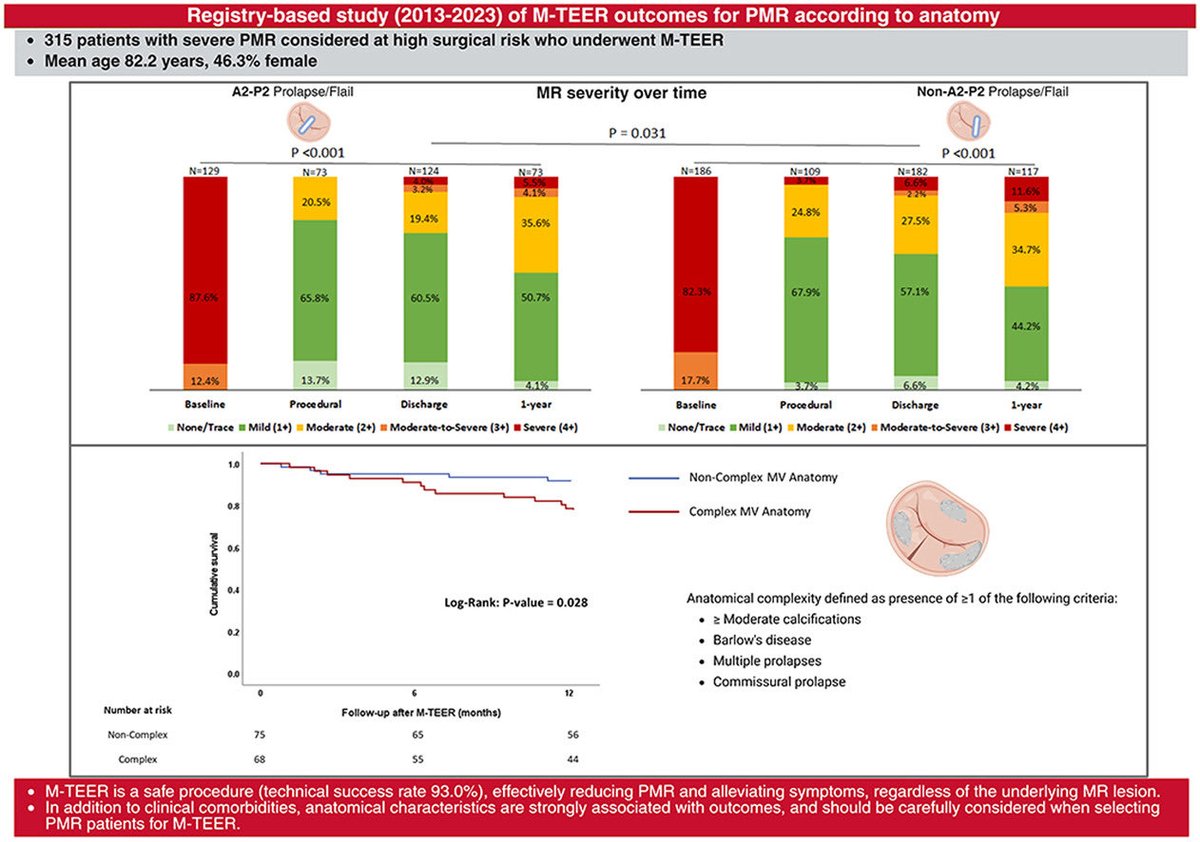
In our 10-year prospective study of PMR patients undergoing M-TEER, MV anatomical characteristics significantly influenced symptomatic improvement & 1-year all-cause mortality. These features should be carefully considered for patient selection. Checkout👇🏽
https://t.co/9Vk1jhQaSM
In a post hoc analysis of the SCOPE trial, patients with obstructive CAD who underwent TAVR had comparable survival, patient-reported health status, and VARC-3 clinical efficacy compared with patients without CAD through 3 years of follow-up. https://t.co/RF8PDs61bX
The extent of cardiac damage significantly affects 10-year survival of patients with moderate and severe aortic stenosis. Cardiac damage staging might be as important as aortic stenosis grading in defining the prognosis of patients with aortic stenosis.
https://t.co/BMu2HmsuLI
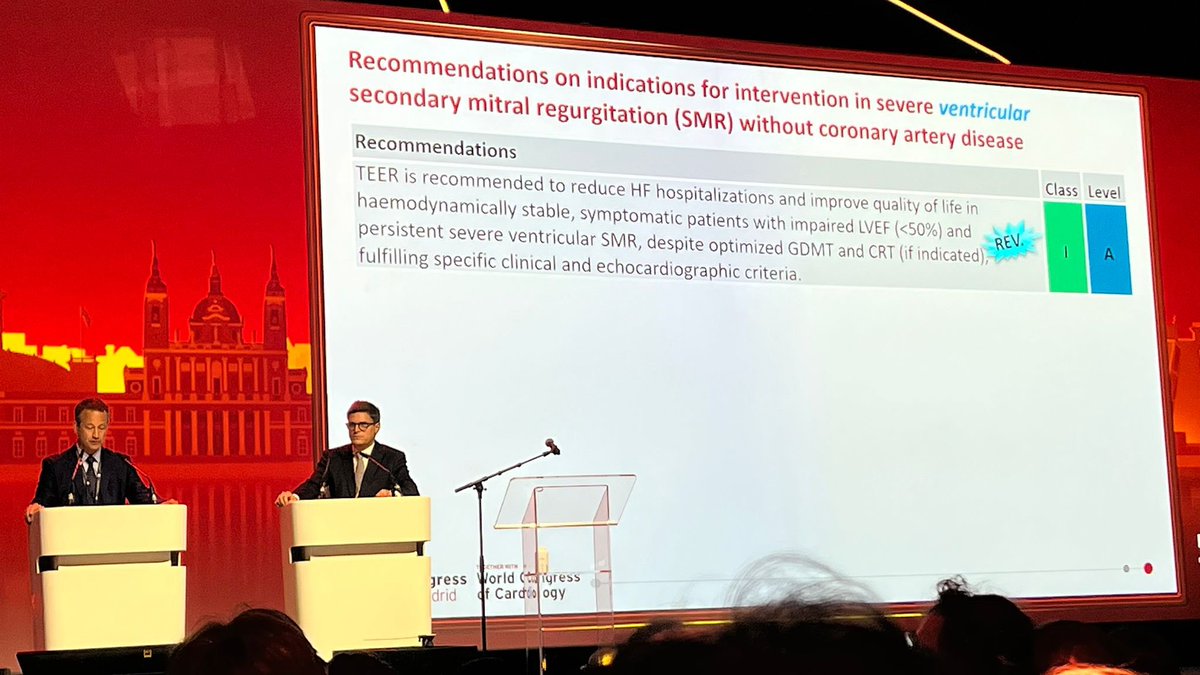
What’s new in the 2025 guidance on valvular heart disease?
📺https://t.co/zukV2M2KXU
@Sticchi_Alex interviews 🎤 @FabienPraz and Michael Borger, co-chairs of the 2025 ESC/EACTS Valvular Guidelines Task Force.
They discuss the major updates, including the central role of multimodality imaging, the lowered age threshold for TAVI, the distinction between atrial and ventricular secondary MR, evolving indications for tricuspid interventions, simplified antithrombotic strategies, and the importance of high-volume Heart Valve Centres.
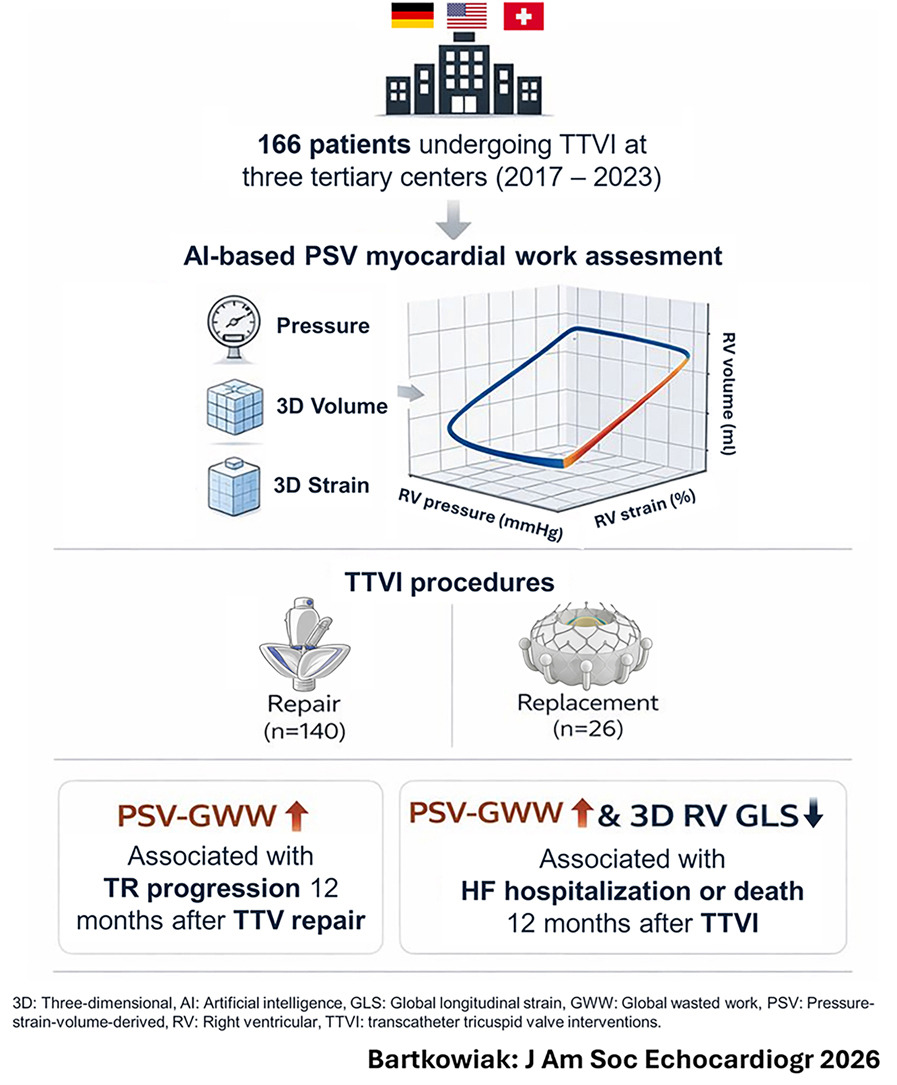
TRISCEND II subanalysis showed greater benefit of TTVR in massive/torrential TR, suggesting this may be the target population (https://t.co/OLkOdJCnH4). In our paper just published, massive/torrential TR did not reduce TTVI eligibility vs severe TR (https://t.co/s8wVRaNOH3)
Live from #ESC2025: @piccoloraf presents results of PARTHENOPE - showing that a personalised post-PCI DAPT strategy was superior to a standard 12m approach, mainly driven by lower rate of ischaemic events, albeit with no major difference in bleeding events with the two strategies
Great lecture by Prof. Gupta @aakriti_15 highlighting a more nuanced approach to timing intervention in patients with asymptomatic severe aortic valve stenosis — a new ! Class IIa indication for intervention in #VHD#guidelines#ESCCongress#esc2025#ESC
Congratulations to @hahn_rt on an outstanding lecture on the role of interventional imaging in transcatheter structural interventions, and on the well-deserved Award in Clinical Cardiology!
#ESCCongress#esc#esc2025
Main takeaways from new #esc25#VHD#guidelines:
Tricuspid and multivalvular VHD:
-> TV surgery if LHD surgery required + >= mod TR or dilated TV annulus
-> TTVI in high risk symptomatic severe TR
-> Treat symptomatic moderate AS&AR
-> Treat moderate AS&MR if EF <50%