Consultant in Medical Affairs | Structural Heart Diseases and Emergency Medicine | Epigenetic | Integrative quantic and holistic medicine | Philanthropy
PARTNER 2A at ten years is a genuinely important paper. Extending a randomised TAVI-versus-surgery trial to a full decade, in an elderly intermediate-risk cohort, is hard, expensive, and exactly the long-horizon evidence the field has lacked. So this isn’t a critique of a flawed study — it’s a note on why two of its headline numbers, both pointing the same way, carry different evidentiary weight.
Start with what the authors did well. Reintervention was analysed as a cumulative incidence function with Gray’s test, accounting for the competing risk of death — precisely the right estimand in a cohort with ~83% ten-year mortality. They even report the naïve Kaplan–Meier (16.1% vs 2.7%, HR 4.26) transparently as a sensitivity analysis, flagging it as the one that overstates risk by treating death as independent censoring. The model isn’t the issue.
The limitation lies upstream, and the authors are candid about it. Nonfatal outcomes did not use the vital-status sweep. Mortality was recovered to ~90% completeness from public records — an impressive salvage. Reintervention runs on the on-study cohort alone. At year six, mortality has ~380/396 patients at risk per arm; reintervention has 174/159. After the five-year reconsent cliff, the durability endpoint is estimated on less than half the randomised population.
What’s worth adding is how much that missingness matters. Among surgical patients alive at five years, 59.3% (270/455) declined reconsent and left at the start of years five to ten — the very window the paper flags as vulnerable for bioprosthetic failure. The 1.6% surgical estimate rests on eight events, three in that late window, while the cohort most likely to generate late events is largely unobserved. Dropout was differential (more in surgery). Reconsent that tracks health is informative censoring, which can bias the CIF itself, not only its variance — and the asymmetry favours surgery looking more durable.
To put a number on it: reconstructing the published CIFs (Aalen–Johansen, validated to reproduce 6.3% / 1.6% and a p-value near the reported Gray’s test), how many unobserved surgical reinterventions would change the conclusion? About ten erase significance; ~25 reach parity. Across the ~425 surgical study-leavers, ten events is a reintervention rate of only ~2–4%.
The literature says that’s a low bar. Around 15% of the trial’s surgical valves were Mitroflow and Trifecta — known early failures; Mitroflow reintervention at ten years ran ~22% Annalsthoracicsurgery. Even durable comparators show late attrition: in NOTION at ten years, with near-complete follow-up, surgical severe structural deterioration was ~10% and bioprosthetic valve failure ~14% PCRonline nih. Reintervention also undercounts failure, since frail octogenarians are often never reoperated — as the authors note. So 1.6% is a floor on a partly observed denominator.
In statistical terms this is a fragility issue, not a flaw: a four-fold relative claim resting on eight events, in an arm that shed ~45% of its follow-up non-randomly, is hard to lean on — however well Gray’s test was applied. The direction is believable; the XT device genuinely predicts more TAVI reintervention (second-generation frame, no CT-based sizing, no 29 mm valve for the first 42.5% of enrolment). What the data can’t pin down is the magnitude.
Contrast the mortality endpoint, where the paper is strongest: HR 1.13 (1.02–1.25), ~90% complete via the sweep, concordant in the ITT sensitivity analysis. That holds up. Its nuances — RMST over years five to ten non-significant, the excess confined to TA/TAo while transfemoral was neutral — are matters of careful reading, not missing data.
So the honest summary is generous: a landmark, methodologically sound trial that delivers a robust mortality result and a directionally sound but quantitatively soft durability signal. The two rest on different foundations — one recovered, one necessarily incomplete — and the authors give us everything we need.
Worldwide first commercial #EVOQUE case today at @unimedizinMainz and #HeartValveCenter closing the loop from interventional innovation to clinical reality, result of robust science and a fantastic newly assembled heart team.
@vonBardelebenRS, H. Treede, T. Goessler, Tobias Ruf
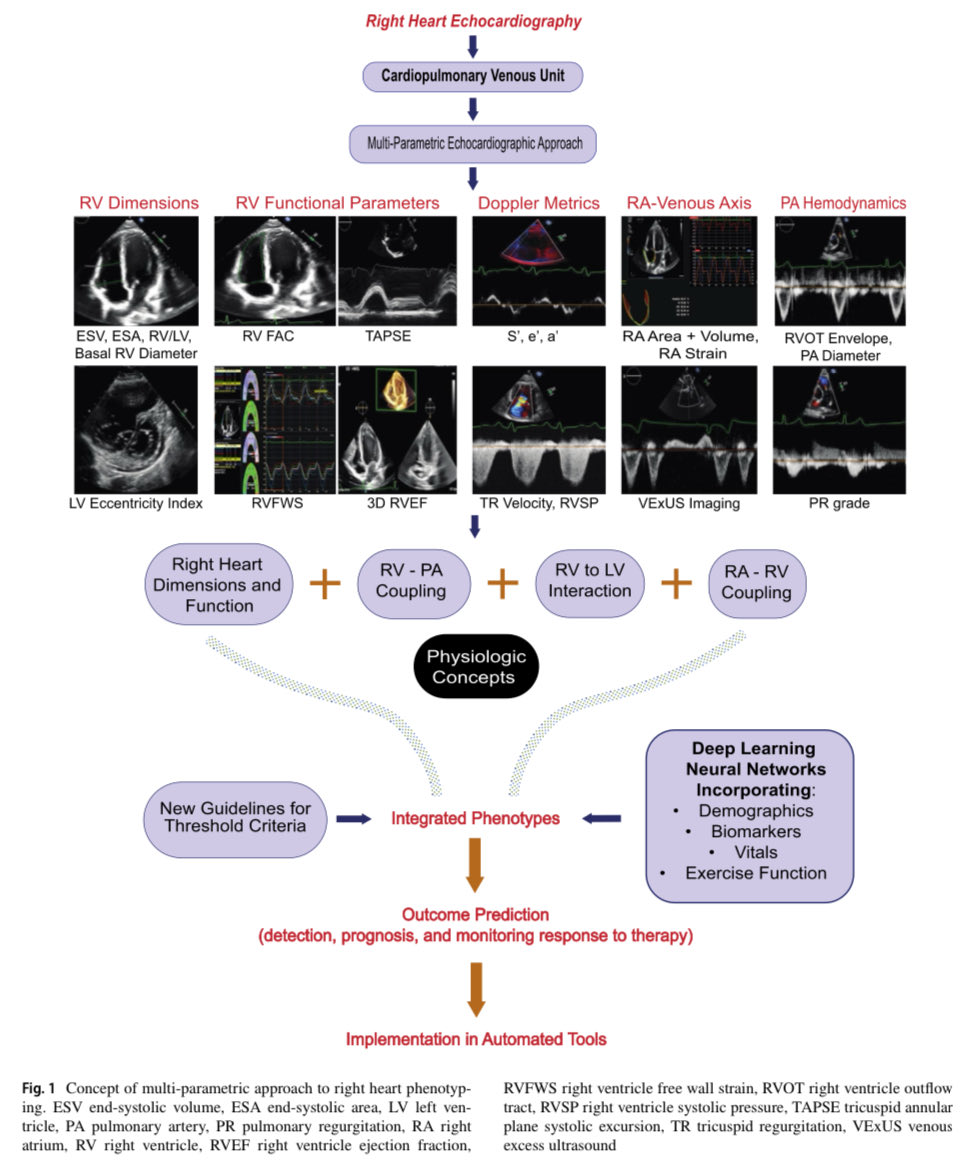
🧩AS and HFpEF: A shared Phenotypic Puzzle
Similar
💡Cardiac Struct/Function
💡Cardiopulm exc
💡Congestion
EAT & Fluid Overload
🎯Prognostic Markers (staging)
🎯Tx Targets
🌐 https://t.co/idE1eX5egC
Honored to share this w/ @azeemlatib@CardioMDPhD@MonteHeart@ESC_Journals
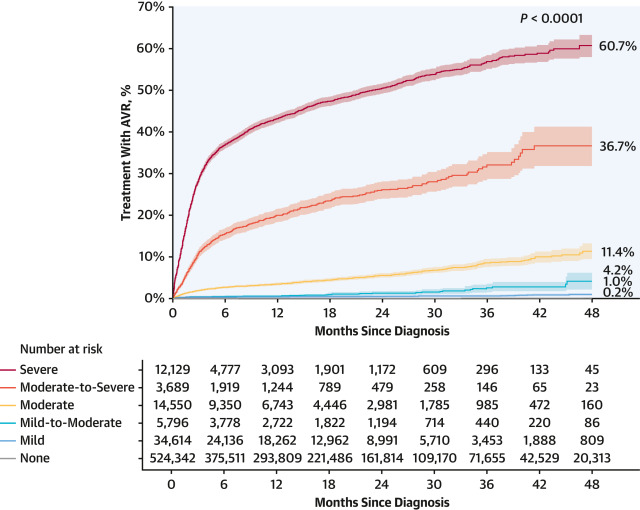
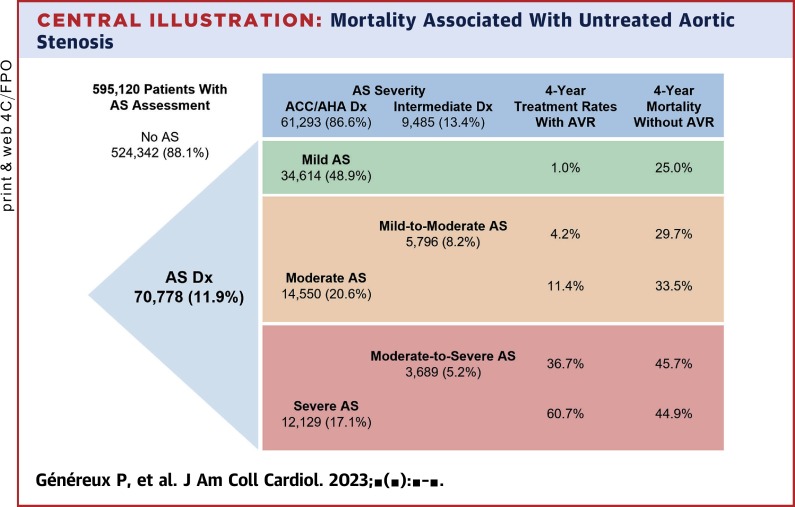
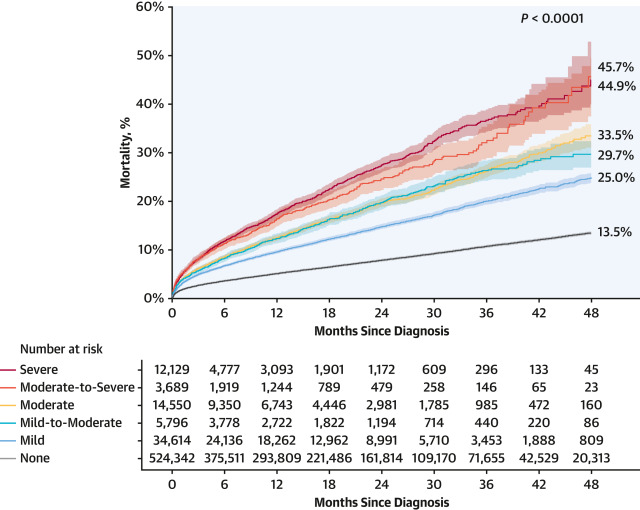
Major Study including >1 million patients from 24 US centers demonstrating the mortality burden of the different degrees of severity of aortic stenosis. And with an editorial from the godfather of AS Dr. E. Braunwald!
https://t.co/GaCYHst2ZF
Partner 3 equivalent great outcomes at 5 yrs for TAVR and Surgery (low risk). Both with all-cause mortality </= 10%!! Published online @NEJM https://t.co/WoY3pxAqm2
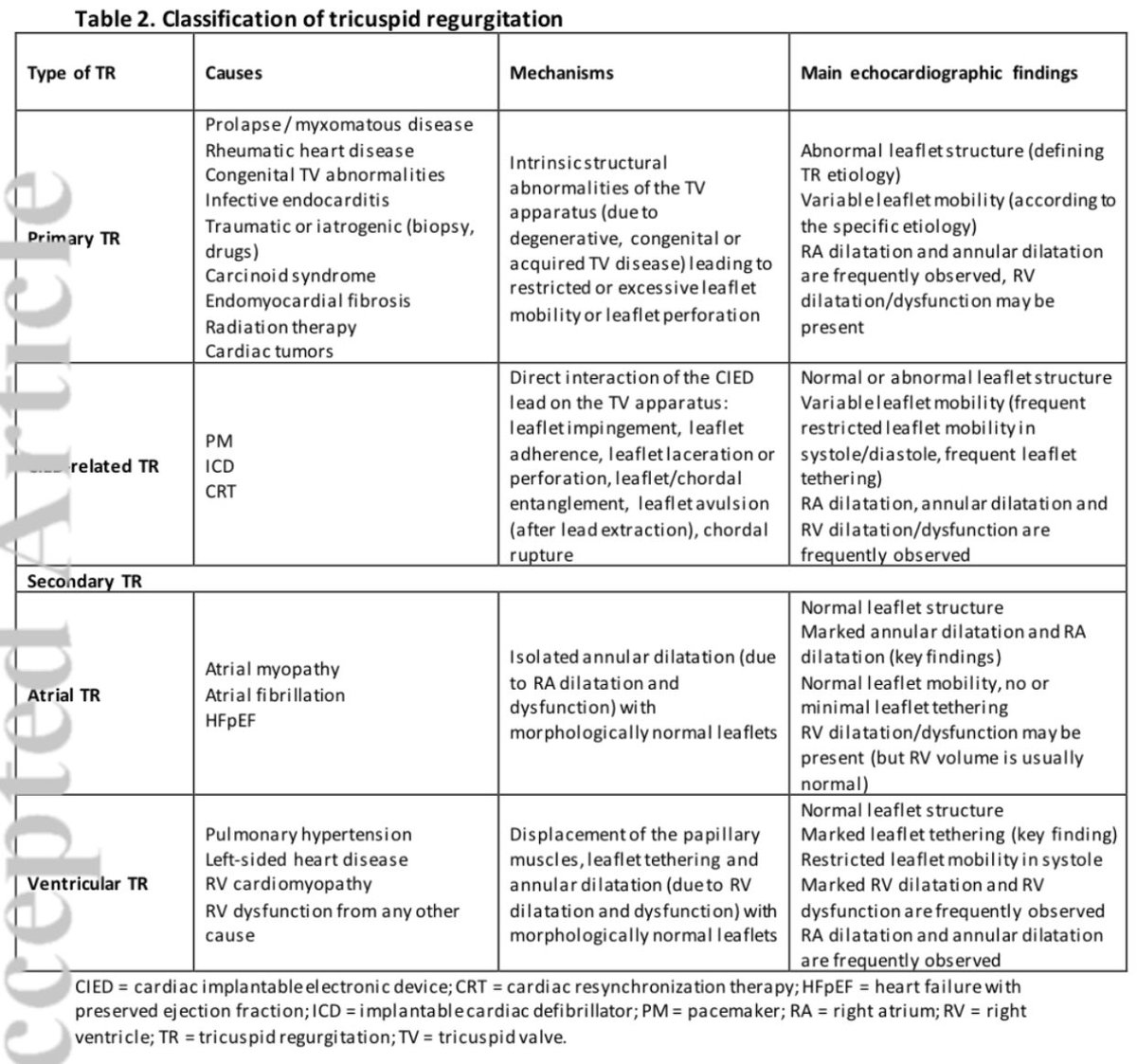
If you missed it, my tricuspid case with PASCAL precison TEER yesterday at #EuroPCR2023@PCRonline. Using IntraCardiac Echo to visualise leaflet capture better in the presence of a pacemaker lead. @EdwardsLifesci
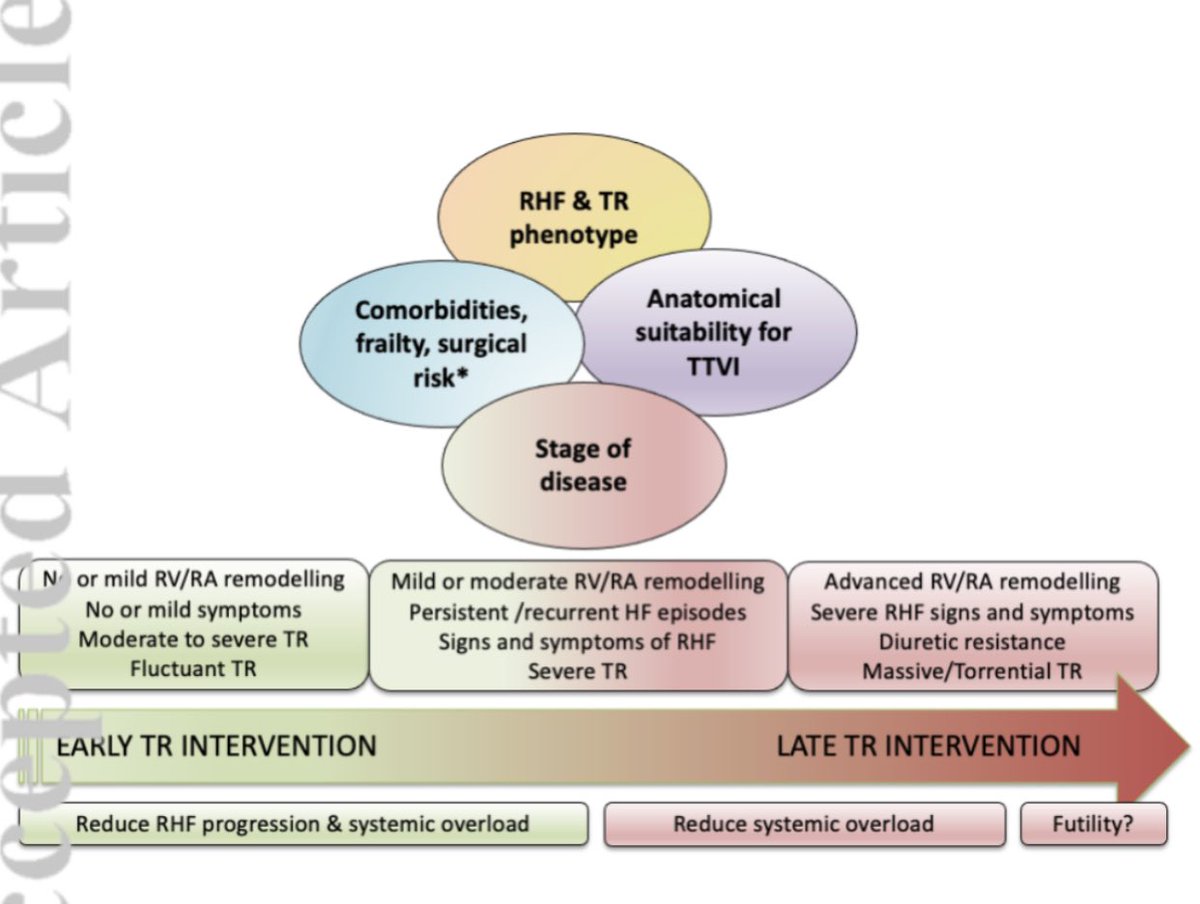
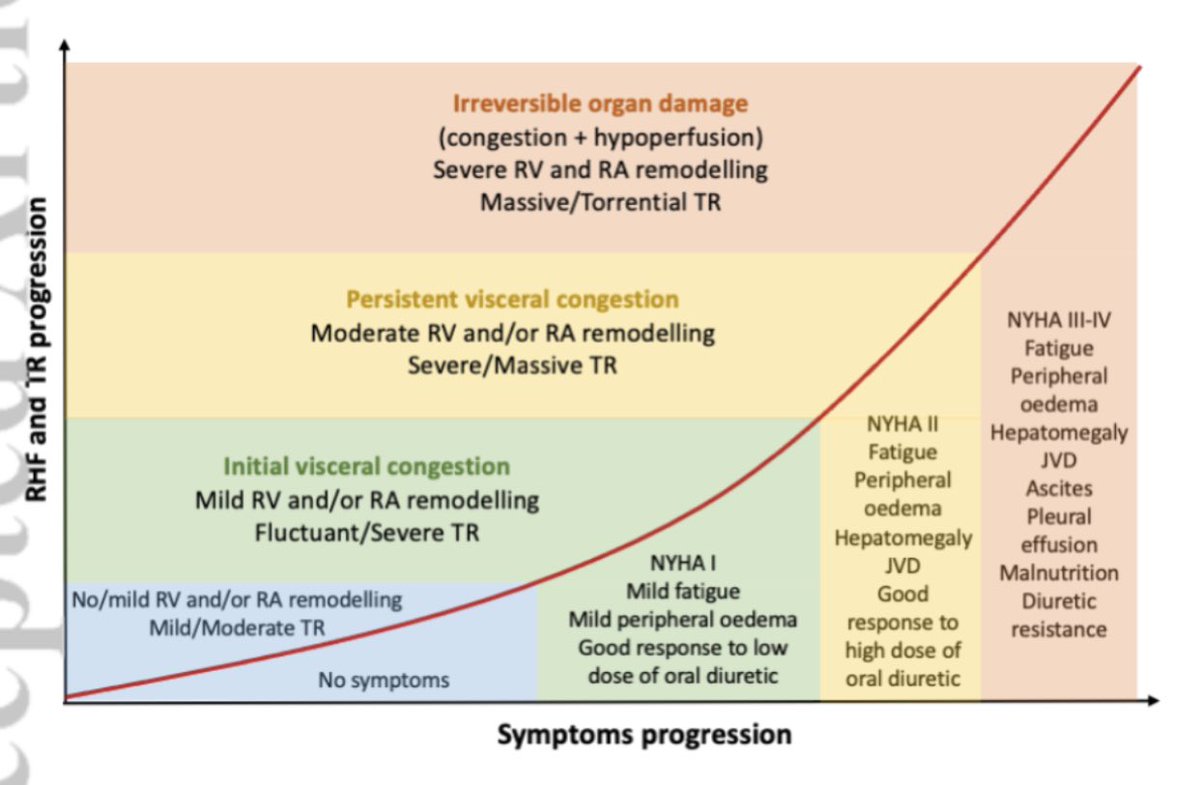
RV/PA coupling predicts outcomes following transcatheter tricuspid intervention but with different thresholds in women vs. men.
From @jaccjournals https://t.co/iE0LFDTA15