Fascinating TRACERx/PEACE study on the evolutionary biology of NSCLC metastasis. Extended Data Fig. 3 is also a particularly neat visual of metastatic seeding patterns to me.
Many potential applications for IO + MDT/LCT with colleagues like @IyengarPuneeth, Daniel Gomez, @CJTsaiMDPhD and liver mets with @MattMcMillanMD@DrPaulRomesser. Also intriguing to consider whether markers of chromosomal instability could eventually help guide which patients, and perhaps which lesions, are most likely to benefit from local consolidative therapy. So much to learn.
Congrats to @CharlesSwanton , @SonyaHessey , and the TRACERx/PEACE teams. https://t.co/ltw754TYir
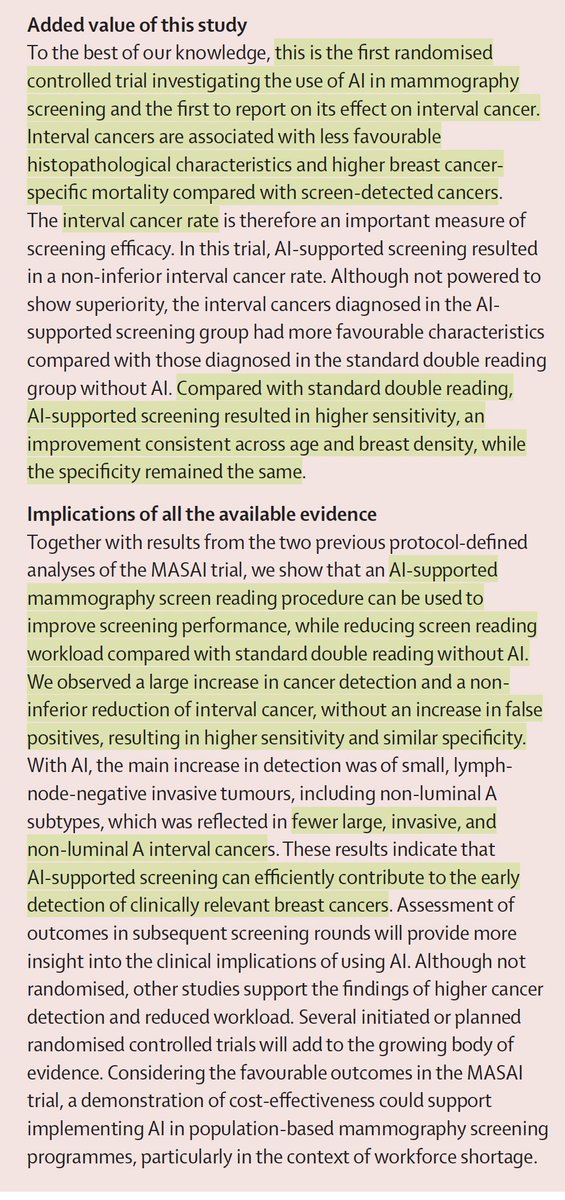
The largest randomized trial of medical A.I.
—Over 100,000 women in Sweden
—radiologist + AI vs 2 radiologists, in follow-up
—AI added led to 29% more cancer detected, 44% reduced workload, and
—Less cancer dx in subsequent 2 years, and, when found, less aggressive
https://t.co/e1hY3F0cGo
The new FLAURA2 OS data presented at #WCLC25 is exciting - nearly four years of median OS with osimertinib + chemotherapy is remarkable progress for our community!
Alongside the MARIPOSA data, it's essential to remember -- this isn't about competition. There is no one-size-fits-all "best" treatment for #EGFR #NSCLC. It's about patients and families.
Clinicians need the right tools to match the right treatment with the right patient. That is why I implore companies to invest in research that helps us understand who benefits most from each approach, through biomarkers, disease characteristics, AND A REAL understanding of #QOL from #PROs (Safety/AE grades are endpoints for trials, not tolerability) - THAT is personalized medicine and how progress becomes meaningful.
As the discussant @danieltanmd said, we need GPS maps to help guide patient treatment pathways. Options are hope, but only if we know how to navigate them.
#LCSM #LungCancer @EGFRResisters #OptionsAreHope
Pts with NSCLC 🫁 and asymptomatic brain mets 🧠, is a poor Px popul.The intensification of 1st line with addition antiCA4 drug (Nivo+Ipi+2 cycles CT like CheckMate9LA) did not reached primary endpoint in NIVIPI-Brain trial.CT+IO remains SoC and new agents are awaited #WCLC2025
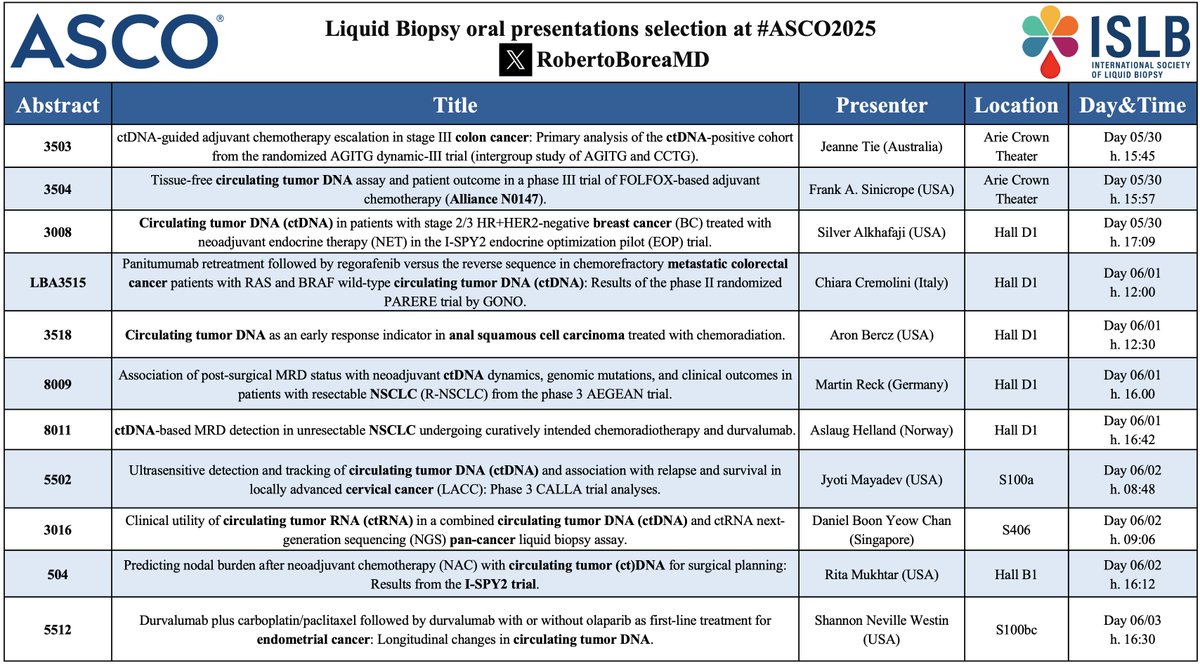
🚨 #LiquidBiopsy in the spotlight at #ASCO25!
From early detection to MRD and real-time monitoring, groundbreaking presentations are highlighting how LB is advancing into clinical practice
📍 Don’t miss them! Stay tuned 🔬
@ASCO@isliquidbiopsy@OSUCCC_James@rolfolab
Best of #ASCO25 - LMIC version
1. CHALLENGE - Exercise for Resected colon ca survivors post chemo
2. Chronoimmunotherapy
3. 15-year SOFT and TEXT update
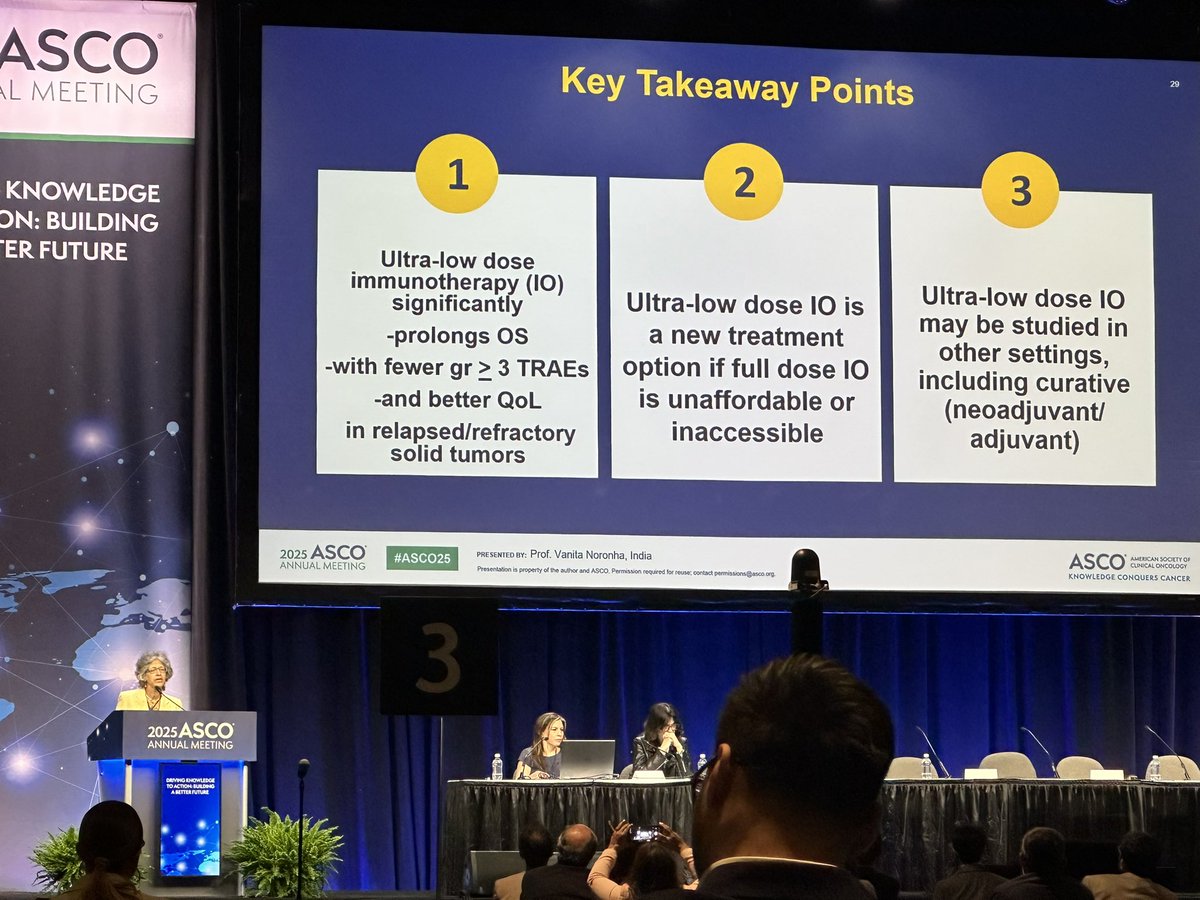
4. Ultra-low-dose I/O for solid tumors in relapsed/refractory setting
@OncoAlert#bcsm#lcsm#crcsm#Immunotherapy
The most practice changing trial from #ASCO25 is now live on @NEJM .If this was a drug, this would be approved today. Globally relevant and low-cost intervention that is not only delaying relapse but actually improving survival.
Perfect case example of a #cancergroundshot trial.
https://t.co/ZnqeplJ7IA
Presented at #ASCO25:
A 3-year structured exercise program after adjuvant chemotherapy for colon cancer improved disease-free and overall survival, physical functioning, and fitness, as compared with health education alone. Full CHALLENGE phase 3 trial results: https://t.co/j3kWJDjuVz
@ASCO
A standing ovation for #CHALLENGE trial at #ASCO25 - first in world to definitively show exercise reduces recurrence and improves survival:
“For every 16 people, exercise prevents 1 person from recurrent/new cancer”
“For every 14 people, exercise prevents 1 person from dying”
A lot of exciting data came out of #ASCO25—but some presentations were a sobering wake-up call.
As @Sonyareid07 highlighted, nearly 50% of patients with mTNBC don’t receive any treatment beyond first-line therapy.
This is unacceptable. In 2025, this should not be the reality. It should alarm every oncologist.
Our patients deserve better—we must innovate, advocate, and push for access to more effective therapies.
#bcsm #mTNBC
This is a major story from #ASCO25. Randomized phase 3 trial of time of day of immunotherapy infusion. Randomized to infusion before or after 3pm. Early infusion far superior: PFS 11.3 vs 5.7 HR 0.42, OS HR 0.45! Impactful, pragmatic, not costly. This should be a bigger story.
Trump’s tariff exemptions are less policy, more pay-to-play.
Remember when capitalism meant selling stuff people actually wanted?
Now it’s about getting blessed by a politician.
We didn’t kill the free market with socialism--we buried it in red tape and handshakes.
It’s not protectionism, it’s patronage.
Capitalism’s still here…
Just behind a paywall.
@DannyCopus I don't disagree, but it's rarely as neat. Obviously when nations counterpunch with retaliatory tariffs, exports suffer, offsetting gains. Your vision of global adoption is ambitious, but it assumes a level of cooperation rarely seen in trade disputes
NIH is a public good titan—cancer cures for all, not just the rich. >99% of FDA-approved drugs from 2010-2019 can be traced to NIH funding, which also powers ~80% of cancer therapies. DOGE dividends sound sexy, but flush taxpayers buy Teslas, not test tubes.
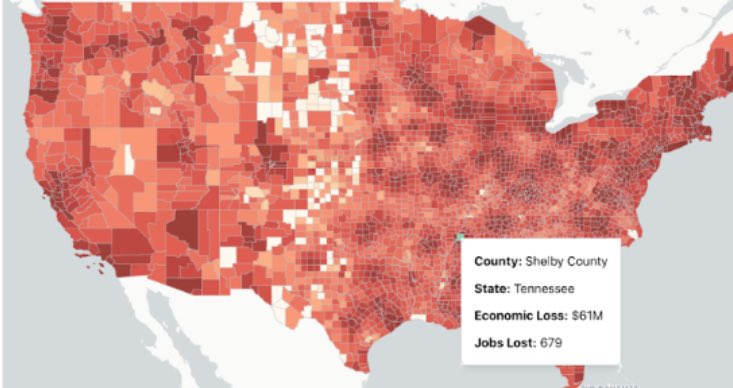
NIH funding cuts could cost the U.S. $16 Billion and 68,000 jobs. An interactive tool from @joshuasweitz and team shows the local impact across the U.S. - down to the county level. This isn’t abstract - these numbers affect real communities and real lives: https://t.co/2gPVnVwaLU
Happy to share our latest paper in @NEJM_AI , led by @IsabellaWies : "Deidentifying Medical Documents with Local, Privacy-Preserving Large Language Models: The LLM-Anonymizer" https://t.co/8wys0engCf
You can use our open source tool with local LLMs to robustly de-identify medical documents.
We just had one of the biggest days in AI.
-Deepseek-V3
-Google Gemini 2.5
-GPT-4o image generation
-Zapier MCP protocol
-H&M AI clones
-China’s AI training breakthrough
-AI cancer detections breakthrough
Here's EVERYTHING you need to know: