For those who've asked in the DMs - Yes, 99% posted is bought (feel free to ask for pgs./opinions about spec. seforim & will try to accommodate). Strictly personal recommendations, hopes to show richness and depths of Torah & to bring to the fore lesser-known authors/titles.
@avidresearch@MirzaCPH $RHHBY's atezolizumab showed pMMR HR 0.92 @ 78% maturity - the most mature IO dataset in EC -essentially zero benefit in the exact pop. EC-042 targets, all while their FM is the CDx platform identifying every TP53wt pt who will receive $KPTI's selinexor.
https://t.co/b5uGGThpQt
@avidresearch@MirzaCPH $KPTI Xport-EC-042 PI agreed to Cantor institutional KOL call June 8, 2026 - weeks before EC-042 topline.
https://t.co/93vachXMOl
$KPTI Thank you Dr. Krivak @AHNtoday "I think SEINDO was I don't want say a sleeper trial... how did this slip by the radar... profound results... absolutely remarkable... tremendously exciting" h/t Dr. Gottfried Konecny @UCLAHealth Dr. Leslie Randall @VCUHealth and @OncLive
@docusalut@HematoHUSE@SonEspases LMS is predom. TP53wt same biomarker driving $KPTI seli in EC. This P1 confirms 60mg weekly as EC-042 delivering median OS of 39.5 mnths vs 12-18. historically w/ gemcitabine alone, with a 36month OS of 50.2% in one of oncology's most difficult diseases.
https://t.co/CczwD5Xy1Q
@harrisoncn1@sk_tantravahi $KPTI Selinexor is a Swiss army knife. 1 drug. 1 mechanism. Multiple indications across TP53wt tumors & XPO1-overexpressing cancers. Works at every Rux dose. Works as monotherapy and across all platelet counts. MF, EC, MM, MDS, AML, NSCLC, TNBC, GBM, ULMS, SGT & counting.
/427
$KPTI MF timeline. P1 update at ASH Dec. 2022, then April 2023 at AACR, initiates P3 June 2023, receive FT July 2023 (received OD in Oct. 2022), Nov. 2023 CEO @ Jefferies "Very open to the possibilities to make sure that we maximize the potential of Selinexor + Rux $INCY".
/1
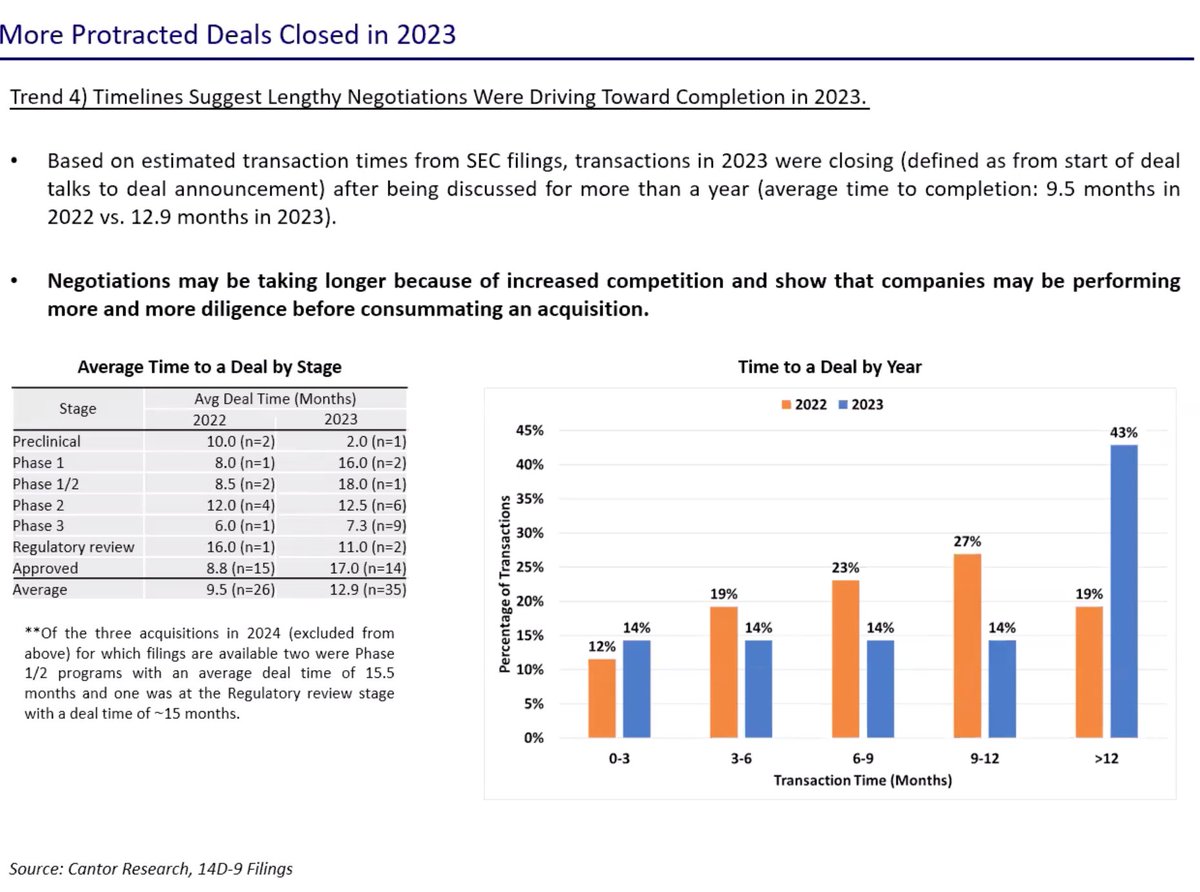
From Cantor: biotech M&A transactions took an avg of 12.9 mos in 2023. From start of deals talks to deal announcement. Assume deal talks start after data, confirming this and how long after data.
@rcoledude $KPTI to Participate in Webcast Featuring Endometrial Cancer Key Opinion Leader on June 8, 2026 Dr. Robert Coleman, MD, FACOG, FACS, a globally recognized gynecologist oncologist and Principal Investigator of the Phase 3 XPORT-EC-042 trial.
https://t.co/V0TsG2U9jP
$KPTI Patients want the therapy now they are more educated then ever & see the unprecedented/robust data & don't want to be on placebo. @Karyopharm do the right thing for patients and file for AA immediately.
@PositiveTopline@avidresearch Fundamental difference w/ SENTRY driven by selinexor's unique anticlonal mechanism (VAF suppression, blast prevention) that pelabresib and momelotinib etc don't have. Those drugs shrink spleens anti-inflammatorily. Selinexor kills the clone. Diff MOA > different OS relationship.
@avidresearch@PositiveTopline Agree. AA is for drugs waiting to show clinical benefit "reasonably likely to predict clinical benefit" selinexor already has it. Dr. Mascarenhas said it yesterday: "SVR35 correlates with survival benefit - this is not just important for this story, but important for the field."
@PositiveTopline@avidresearch FDA is looking for a branch to climb down - SVR35 as validated OS surrogate, instrument bias explaining the TSS miss (Dr. Mascarenhas) & VAF + blast suppression + OS HR 0.43 = disease modification profile no prior MF drug ever showed gives them exactly that branch.