No one should be able to order a bioweapon through the mail.
@IFP & @JoinFAI are proud to co-lead an open letter calling for mandatory DNA synthesis screening & recordkeeping.
Signatories include:
- Sam Altman, CEO & Co-Founder, OpenAI
- Dario Amodei, CEO & Co-Founder, Anthropic
- David Baker, Director, Institute for Protein Design; 2024 Nobel Prize in Chemistry recipient
- Patrick Collison, CEO & Co-Founder, Stripe
- Paul Graham, Founder, Y Combinator
- Demis Hassabis, CEO, Google DeepMind; 2024 Nobel Prize in Chemistry recipient
- Emily Leproust, CEO & Co-Founder, Twist Bioscience
- Lawrence Lessig, Roy L. Furman Professor of Law and Leadership, Harvard Law School
- Gerald W. Parker, former Special Assistant to the President for Biosecurity and Pandemic Response
- Mustafa Suleyman, CEO, Microsoft AI
- Alex Tabarrok, Professor of Economics, George Mason University
- Alexandr Wang, Chief AI Officer, Meta; Founder, Scale AI
- Christine E. Wormuth, President & CEO, Nuclear Threat Initiative; 25th Secretary of the Army
Read the letter and see the full list of signatories: https://t.co/BwZiJXw3JT
Many DNA synthesis companies voluntarily screen orders to mitigate biosecurity risks, but no law requires them to do so.
Leaders in AI, biotech, life sciences, national security, and the nucleic acid synthesis industry agree that Congress should act to strengthen safeguards against biological threats.
@deanwball put it well in the WSJ:
“If you’re synthesizing the stuff that yields biological life and viruses, we’re asking you to screen to see whether it is dangerous in some way. That seems like a reasonable thing for society to insist upon.”
China is winning the drug discovery race. There's no better example of this than multiple myeloma.
https://t.co/YaJSUquRoa
It's one of the most painful cancers, destroying bone from within. For decades, patients endured cycles of brutal treatment and relapse. Then came Carvytki: a one-time CAR-T infusion that appears to cure some patients who have failed multiple treatments.
Its development story, beginning in 2016, was an early signal of a shift now making headlines: the US is losing biotech dominance to China. Though the foundational science was largely American, a nimble Chinese company moved faster with a better molecular engineering idea.
Unless the US addresses clinical-trial bottlenecks slowing early in-human data, more breakthroughs will be developed elsewhere, weakening the ecosystem American biopharma depends on.
Some key points from my article for @WorksInProgMag, with my friend Amol Punjabi, of @EvidenceOpen:
1) Multiple myeloma is not only extremely painful in and of itself, but also one of the most brutal cancers to treat. As first-line therapy, patients endure four drugs simultaneously, then a stem cell transplant, followed by continuous maintenance therapy. And most still relapse, with each treatment round carrying worse chances.
2) A drug called Carvykti, approved in 2022, is changing the treatment landscape. Carvytki acts as a single, one-time infusion. It's a CAR-T therapy, part of a new wave of transformative immunotherapies: made from the patient's own immune cells and reprogrammed to hunt cancer. In patients who had already failed 4+ other treatments, 33% were still disease-free after 5 years. The results as earlier line therapy look even more promising.
3) Most of the foundational science was American. Decades of CAR-T research, and in 2013 the NCI showed BCMA-targeted CAR-T cells could kill myeloma in the lab.
4) But the drug that ultimately changed myeloma, Carvytki, originates from China. Carvytki beats Abecma (the American CAR-T for myeloma) by a wide margin: 36 months of progression free survival in heavily pre-treated patients versus Abecma's 9 months.
5) In 2016, Legend Biotech was just beginning clinical trials. This was the same year the American team was publishing their first-in-human results. Legend started later, but moved faster. Clever engineering and China's ability to get drugs into humans quickly gave them the edge. Large American biopharma J&J ended up striking a deal with Legend and developing the therapy.
6) Never underestimate the llama: US-developed Abecma used mouse antibody fragments to target BCMA. Chinese startup Legend used llama nanobodies instead. These are smaller, more stable and bind more cleanly to BCMA. The usage of llama as opposed to mice antibodies is what is believed to lead to Carvytki's superior efficacy.
7) In retrospect, Carvytki should have been an early warning. China is winning the drug discovery race through deliberate policy. Their first-in-human clinical trials can launch in 6 months vs 18+ months in the US, letting them iterate faster between lab and clinic. The @nytimes recently reported that ~50 percent of major drug deals this year involve Chinese-origin drugs, up from nearly zero a decade ago.
8) The US still leads in late-stage development, as shown, but the pipeline feeding it is increasingly Chinese. The worry is that this will mirror what happened in solar, batteries, and EVs, where early-stage dominance eventually became control of the entire chain.
9) A proposal to streamline early stage trial regulatory requirements to keep the US competitive has made it into the President's 2027 budget for the FDA. But Congress has to act to make it a reality.
FDA rejection letters can act like roadmaps for drug development. But recently a law firm challenged FDA's authority to release them to the public. I wrote about why this challenge to FDA transparency matters. 🧵
4/ If FDA has learned something that could prevent failed trials, reduce uncertainty, and speed better drugs to patients, we should want that knowledge shared.
But the disclosure rules encourage the opposite.
@otis_reid Also, a CRO probably would need to vertically integrate or partner closely with sites to drive down costs. That's hard and expensive (some are trying, though!).
@otis_reid It's a good question! Risk aversion is part of it: the safest CRO will get picked over the cheapest CRO. But there's a few other factors hold back competition: The industry is consolidated and entry is hard. Switching costs are high.
First post!
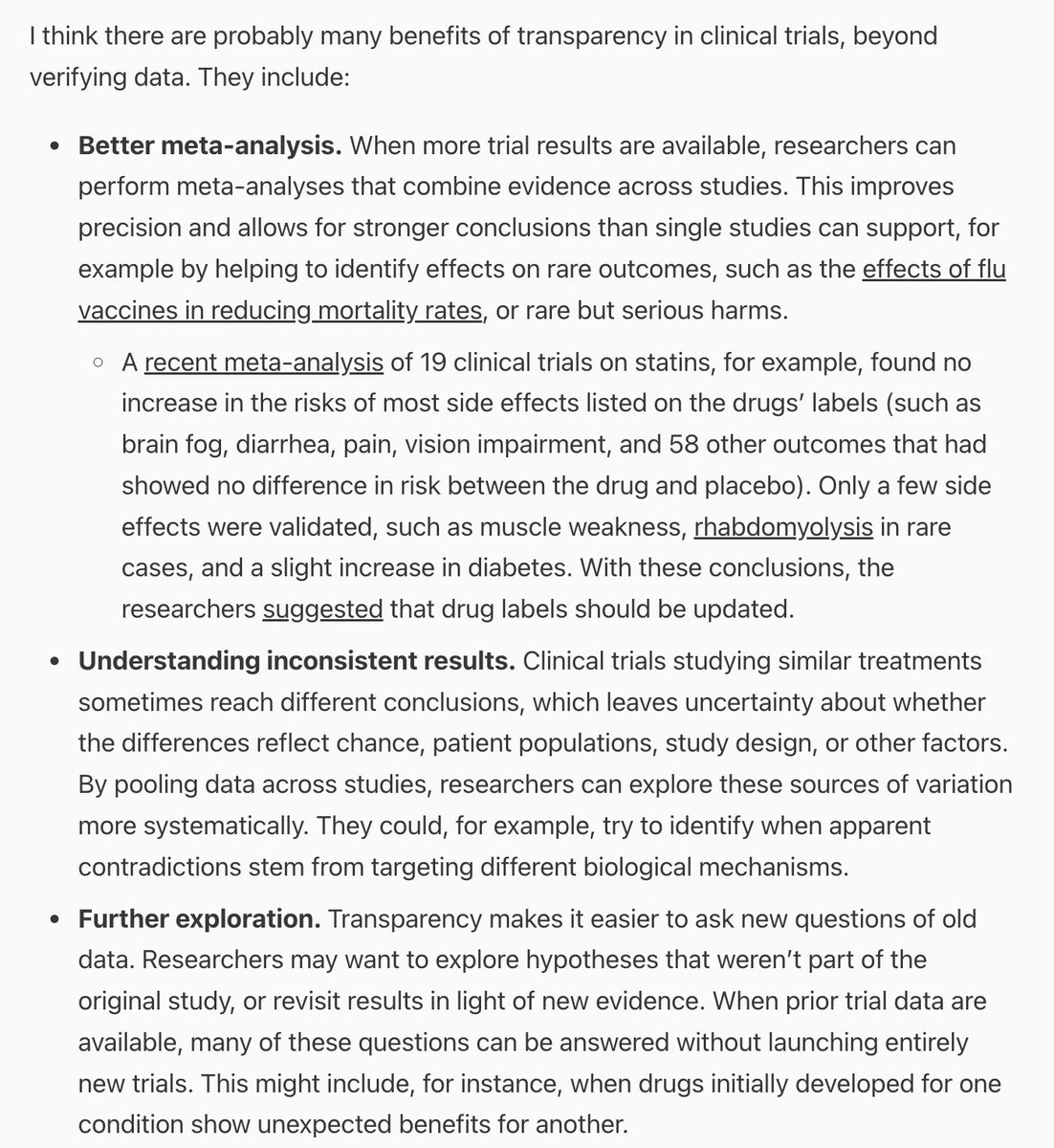
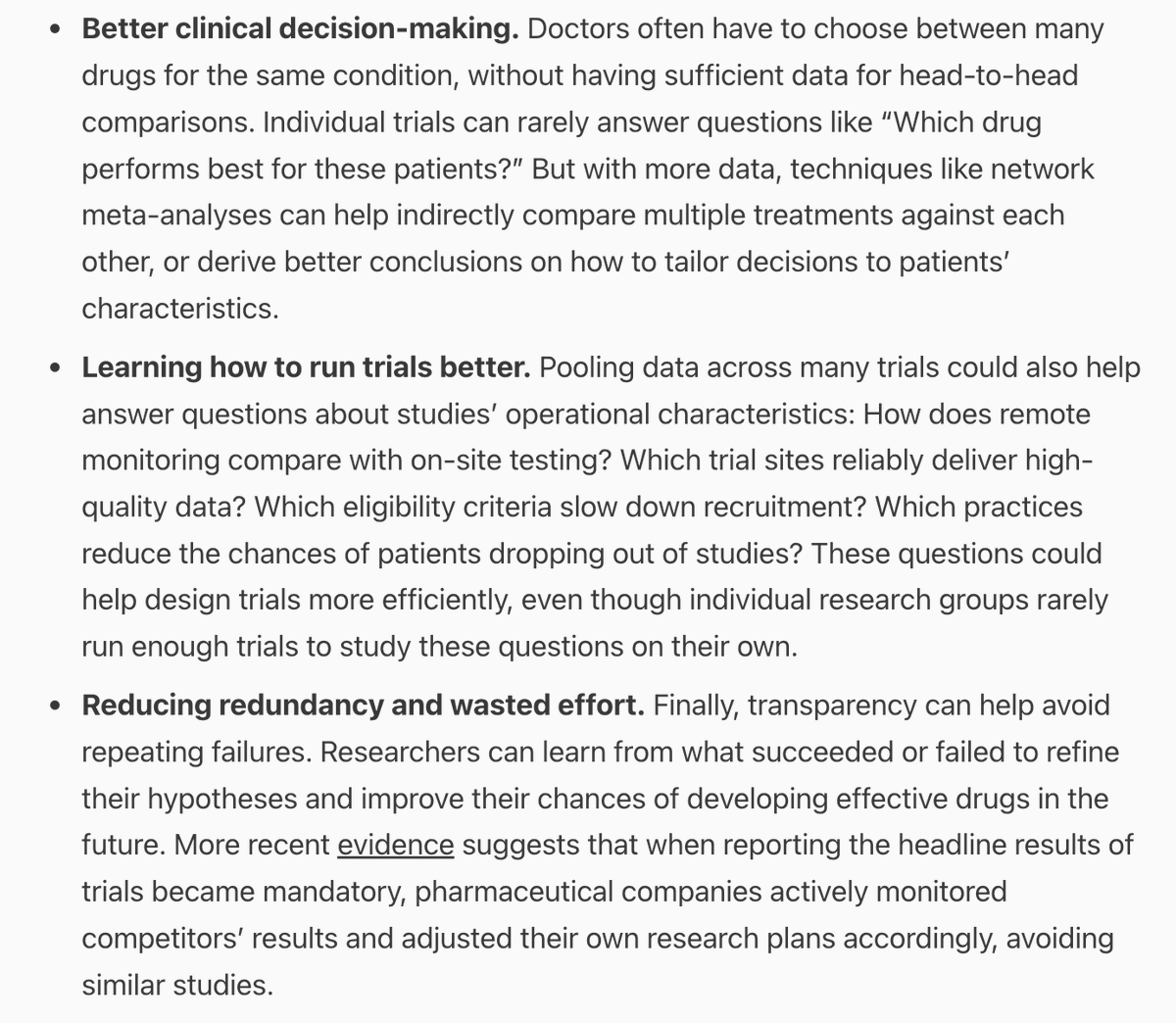
The case for sharing clinical trial data, by me.
Sharing individual patient data from clinical trials can make a lot of further research possible – including better meta-analyses and learning how to run trials more efficiently in the future.
https://t.co/F06APzZNin
NEW BLOG!
@RuxandraTeslo, @kroetscha, @vientsek, @NeuroStats, and I have started a joint blog on Clinical Trials Abundance!
We'll aim to publish weekly thoughts, commentary and ideas on how to make clinical trials more efficient & abundant.
Subscribe: https://t.co/yxZJ43R1At
@doc_BLocke@varma_ashwin97@calebwatney Agree. What looks like flexibility in the regulations can turn into ambiguity on the ground. We would benefit from more certainty - like safe harbors - so sponsors know what “good enough” looks like.
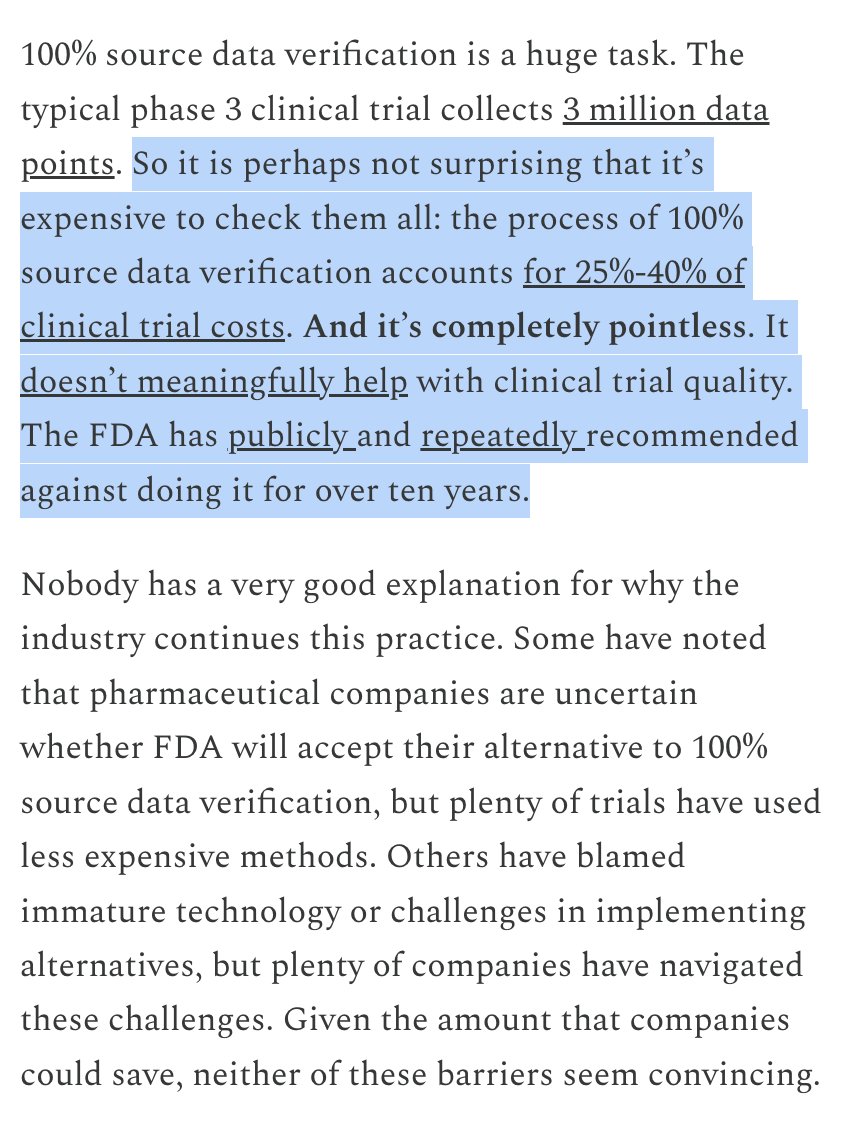
25-40% of clinical trial costs come from an excessive quality-check process that the FDA itself has recommended against for over a decade.
Great piece from a former FDA official on why the whole system is stuck in a "too big to fail" loop.
https://t.co/yX4gNVy04k
I'm very excited to announce a new research project: the Clinical Trials Efficiency Project. Through this work, funded by Coefficient Giving, we will be advancing systemic reforms to reduce clinical trial costs.
High clinical trial costs limit what we can study and limit the availability of new treatments for patients. To make trials cheaper and faster, we need systemic reforms to the policy, incentives, and infrastructure that underlie our clinical trials system.
So what do we do?
✔️ Clearer, more specific rules (safe harbors, measurable standards)
✔️ Proportionate penalties (to avoid overcompliance)
✔️ Strong, competent bureaucrats (yes, really) to keep cascades in check
Why do rules and regulations so often mushroom into binders of procedures, audits, and checklists—far beyond what government actually requires?
I call this the regulatory cascade. 🧵
The danger isn’t just inefficiency.
A culture of zero tolerance for “badness” can distort decision-making and stifle innovation.
More process ≠ more safety. Sometimes it just means more clutter.