IMHO, linezolid has replaced the awkward combination of {vanc + clinda} for toxin suppression & MRSA coverage in toxigenic skin/soft tissue infections
🔥easy dosing
🔥no nephrotoxicity
🔥little resistance among GAS
so the final regimen is {linezolid + beta-lactam}
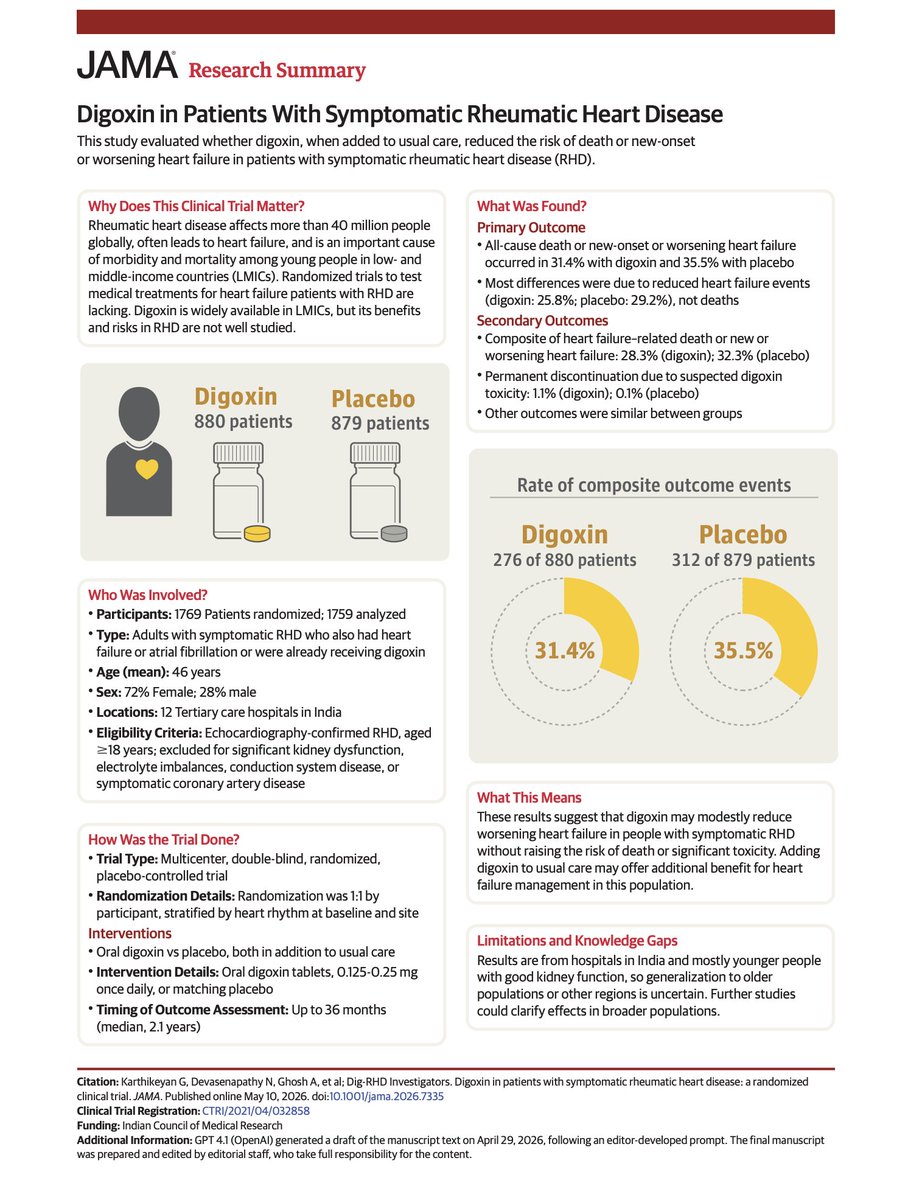
Dear @JAMA_current and @NEJM and other journals, the trend of doing "research summaries" or short videos to condense trial manuscripts is a bad idea
Details matter; supplements matter; critical appraisal means going deeper into the specifics
If modern-day docs are going to offer more than an LLM, we will need to learn to read deeper into studies
Rely on short summaries/central figures and you are at risk for being bamboozled, like the LAAO proponents
@ABsteward@BradSpellberg@DrToddLee CHEST guideline basically says albumin is only for cirrhosis with SBP or HRS
I agree w CHEST & I think this is current standard of care
SSC guidelines are always wonky I wouldn’t pay too much attention to them
dont use albumin in sepsis, thank u next
https://t.co/CbTygeC4T3
Are we realising the potential of our networks to make change happen?
Most innovation emerges from collaborative projects where teams openly “borrow” & adapt each other’s (often small but powerful) ideas. Many networks & communities of practice could achieve so much more by experimenting together around collective priorities to generate & share new solutions.
This is beyond spreading known “best” or “good” practices. It is about innovating to design new solutions collectively.
So I appreciated this piece from Ed Morrison of @Strategic_Doing about three different kinds of networks:
- Advocacy networks are communities that seek to mobilise people, creating pressure to shift policies, priorities or messages in a particular direction. Their aim is to connect & influence rather than to change how they themselves work.
- Learning networks are communities of practice. They share knowledge, compare practice & build shared capability. Learning networks often excel at spread & improvement of existing practice, but only sometimes move into structured innovation work.
- Innovating (or transforming) networks are communities that combine their assets - ideas, relationships, data, capabilities - to create new value that none could produce alone. They manage collaboration as a process of experimentation: agreeing a shared outcome, running multiple connected tests of change, learning by doing & amplifying what works across the network.
https://t.co/70NcTsBLjl
Every learning network has the potential to become an innovating/transforming network. Some actions to enable this:
1. Build a foundation of strong, trusting relationships within the network, understanding each member’s starting point & motivation for change
2. Focus on helping each other to succeed; listen to each others’ stories & plans, co-coach, give advice to each other & build shared inquiry
3. Move from “sharing” or “raising awareness” to some concrete outcomes the network want to change together through collective experimentation
4. Agree some simple norms for the network so that members help each other to make progress, make it safe to try things, fail fast & share incomplete work
5. Encourage multiple, parallel tests of change around similar outcome so projects can “steal with pride” from one another & quickly refine promising ideas
6. Put simple routines in place for noticing patterns (what is shifting where & why), capturing these insights & amplifying them across the network
7. Add additional success metrics including innovations tested, adapted & adopted in multiple places
Graphic by Ed Morrison.
Content with added inspiration from @juneholley.
Antibiotic duration for bacteremia is something most of us learned by habit, not by trial data. In the latest episode of Beyond Journal Club, a collaboration between @COREIMpodcast and NEJM Group, we walk through the BALANCE trial and use it as a lens to revisit how the factors of host, organism, and source should guide treatment; when is shorter really enough, and when isn’t it?
🎧 Listen to the full episode: https://t.co/lHuFPllzHf
📖 Further reading
Original Article by N. Daneman et al.: Antibiotic Treatment for 7 versus 14 Days in Patients with Bloodstream Infections https://t.co/3Z5oQ8yrg8
Didn’t match in Cards?
Did Crit Care freeze you out?
Is that hospitalist job looking little too intellectually bankrupt?
Don’t get mad, become a nephron!
We have a spot in the July 2026 class that would fulfill dreams you didn’t;t know you had!
DMs are open
(Please RT)
Reading a medical chart. Same errors repeated over and over again by people relying on copy/paste.
Yes it's fast and yes it's easy. But it's lazy, obvious, and it makes for a shitty note. Please stop doing this.
I said what I said.
would not start antihypertensives, would discharge home immediately. this question stem feels like the beginning of some horrible sequence of iatrogenic events.
Three antibiotic myths that simply refuse to die — penicillin allergies, the “must finish every dose” rule, and the idea that antibiotics help colds.
New post -- link on next tweet👇
Healthcare workers, remember our oath & stay engaged. We are trusted voices for our patients & the public at large. This is an incredible honor. Don’t jeopardize it or squander it.
#MedTwitter#NurseTwitter#Pharmacy
Really proud of this one: https://t.co/mabvWA4pTU
“The expertise of an ID pharmacist should not be a luxury reserved for well-resourced academic medical centers but a necessity for an adequately staffed ID consult service (remote or local) at any care facility.”
1/
Grateful to @CIDRAP and @mtosterholm for highlighting our collaborative vaccine RCT table in their latest viewpoint.
This kind of recognition reinforces the value of collective, evidence-based efforts to bring clarity to vaccine research.
@BradSpellberg
https://t.co/j3XF23W5du