Must-read Review in Nature Medicine from @DanielJDrucker: a masterclass on how GLP-1 medicines moved from glucose control to reshaping obesity, CV, liver, kidney, neuro and addiction care.
https://t.co/8ydiYIxdS0
Estradiol fluctuations across the life course shape #MASLD risk, with risk rising once estrogen levels fall after #menopause.
@EndoSocJournals
https://t.co/oreNGGxaIA
The gastrointestinal side effects of GLP-1 drugs are mediated by the brain, not the gut. The gut-brain axis at work @jclinicalinvest
https://t.co/8meow41j83
🪨🫀 Seventeen years to change practice: will the 2025 ESC/EAS lipid guidelines finally move the needle?
This 2026 Atherosclerosis state-of-the-art review by Ray & Kronenberg asks a blunt question many clinicians quietly share: why does it take nearly two decades for lipid guidelines to meaningfully change real-world care—and will 2025 be different?
🧠 What’s genuinely new in 2025
The update modernizes lipid care in important ways:
📊 SCORE2 & SCORE2-OP now include fatal + non-fatal events and extend risk prediction up to age 89, correcting long-standing underestimation in women and younger adults
🧪 Non–HDL-C replaces total cholesterol, a biologically smarter move
💊 Expanded therapies: bempedoic acid, evinacumab, clearer positioning of icosapent ethyl
🚑 Acute coronary syndrome care flips the script: early, upfront combination therapy instead of slow stepwise escalation
🧬 Universal Lp(a) testing once in adulthood—finally explicit, finally serious
⚠️ But the Sisyphean problem remains
The authors are unsparing about what still holds us back:
Guidelines assume monotherapy first, despite clear evidence that 50–80% of high-risk patients need combination therapy from day one
Persistent inconsistencies across ESC documents (prevention, diabetes, dyslipidaemia)
Risk thresholds remain arbitrary, short-term, and poorly aligned with lifetime risk
Above all: implementation failure—evidence moves fast, practice crawls
🧠 The real insight
This is not a science problem.
It’s an implementation science failure.
Publishing better guidelines without embedding behavioral change, digital tools, feedback loops, and system-level incentives simply restarts the 17-year cycle.
🔮 Bottom line
The 2025 ESC/EAS update is scientifically stronger, more modern, and more honest than its predecessors.
But unless guidelines are designed for how clinicians actually work, the rock will keep rolling back downhill.
👉 The question is no longer what we recommend.
🧭 It’s how we make it happen—this time faster than 17 years.
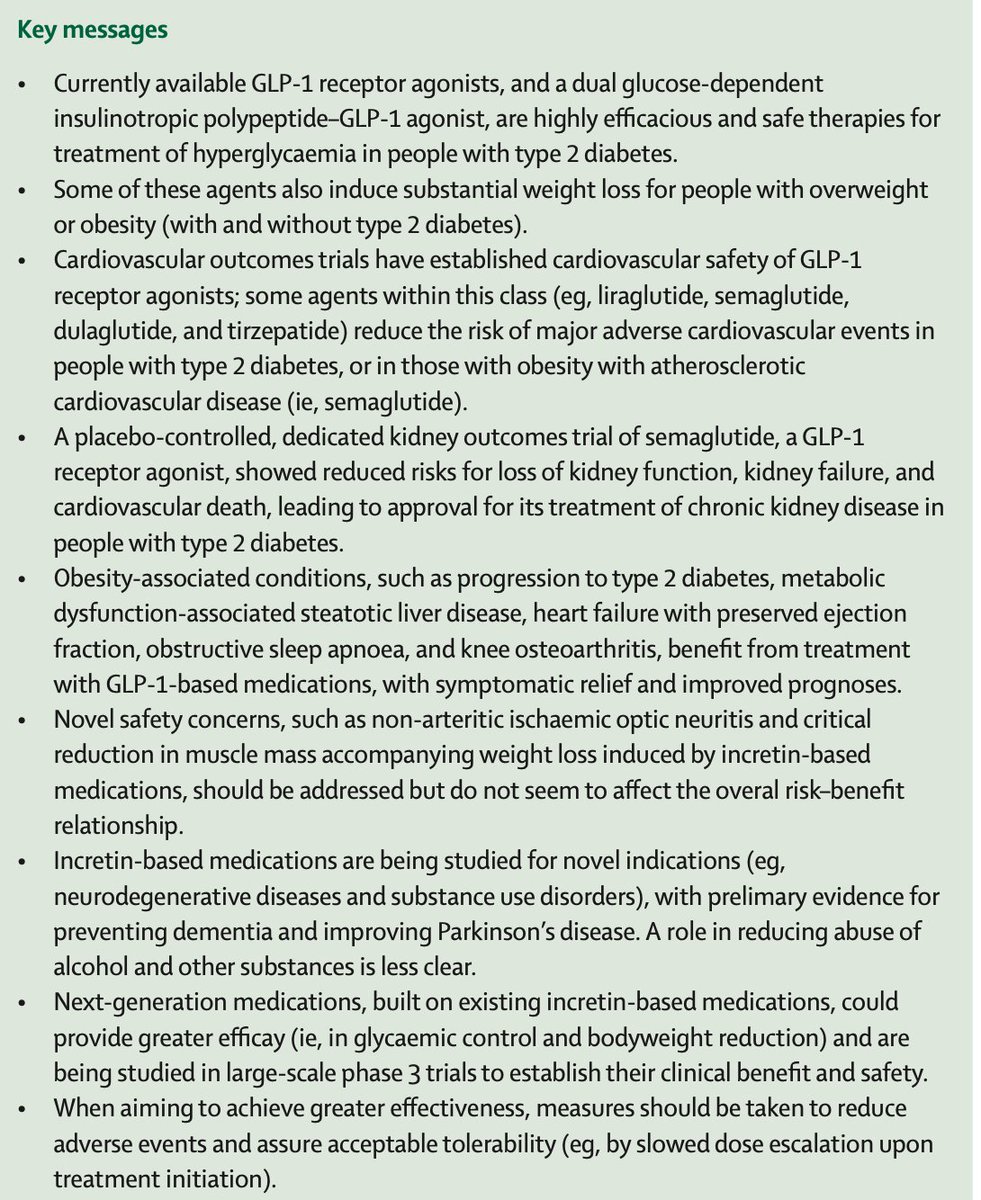
A 5★ new review of the GLP-1 drugs, what they have achieved, and where the field is headed with so many new molecules and combinations @TheLancet
https://t.co/E1Xa15fk1q
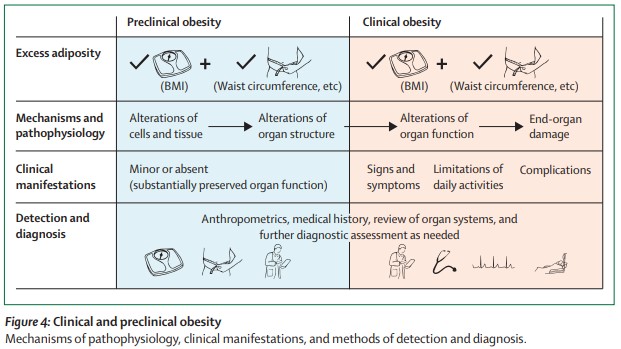
Our #MostRead article in 2025:
Definition and diagnostic criteria of #clinical#obesity https://t.co/cM8pyJ2UG9
#FREE to read with registration (also FREE)
I'm obsessed with cognitive biases.
A "cognitive bias" is a systematic error in thinking that destroys decision-making.
11 most powerful (and dangerous) cognitive biases I've found: 🧵
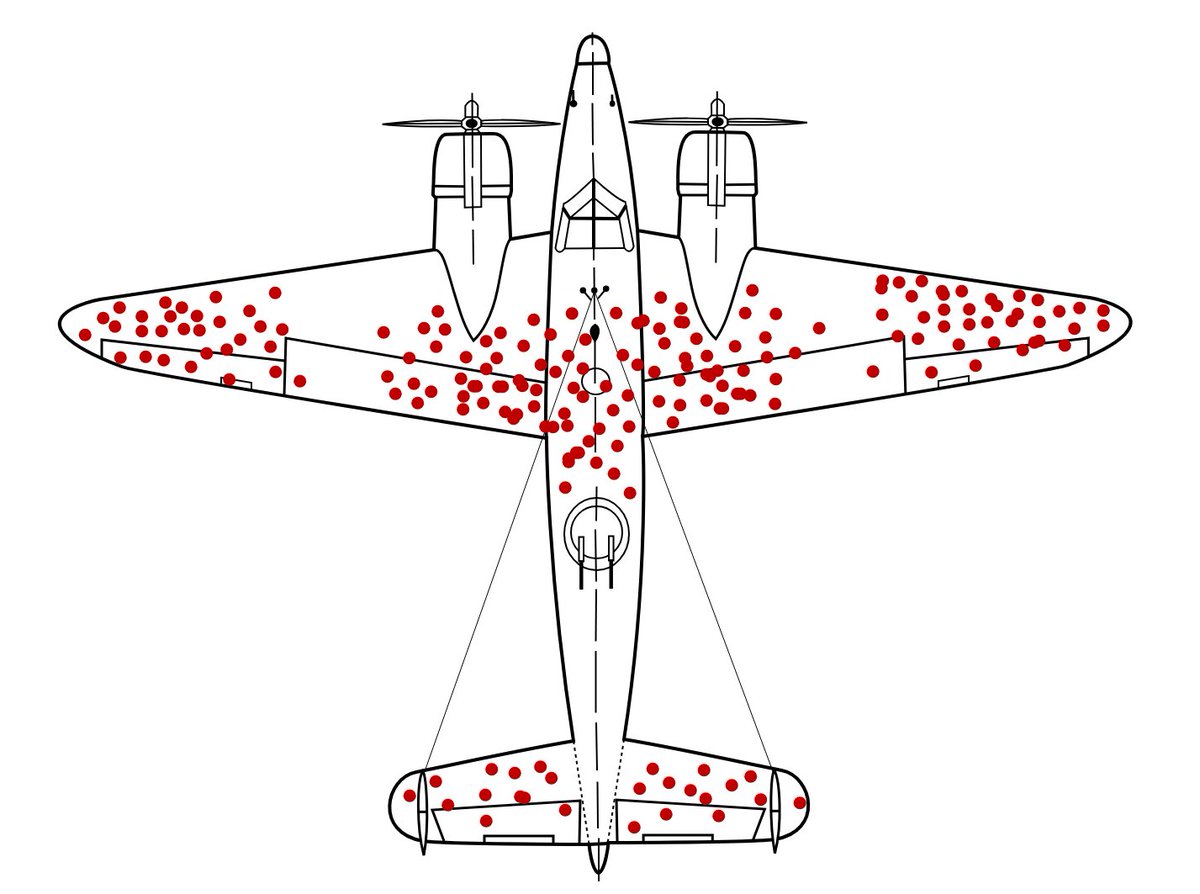
1. Survivorship Bias:
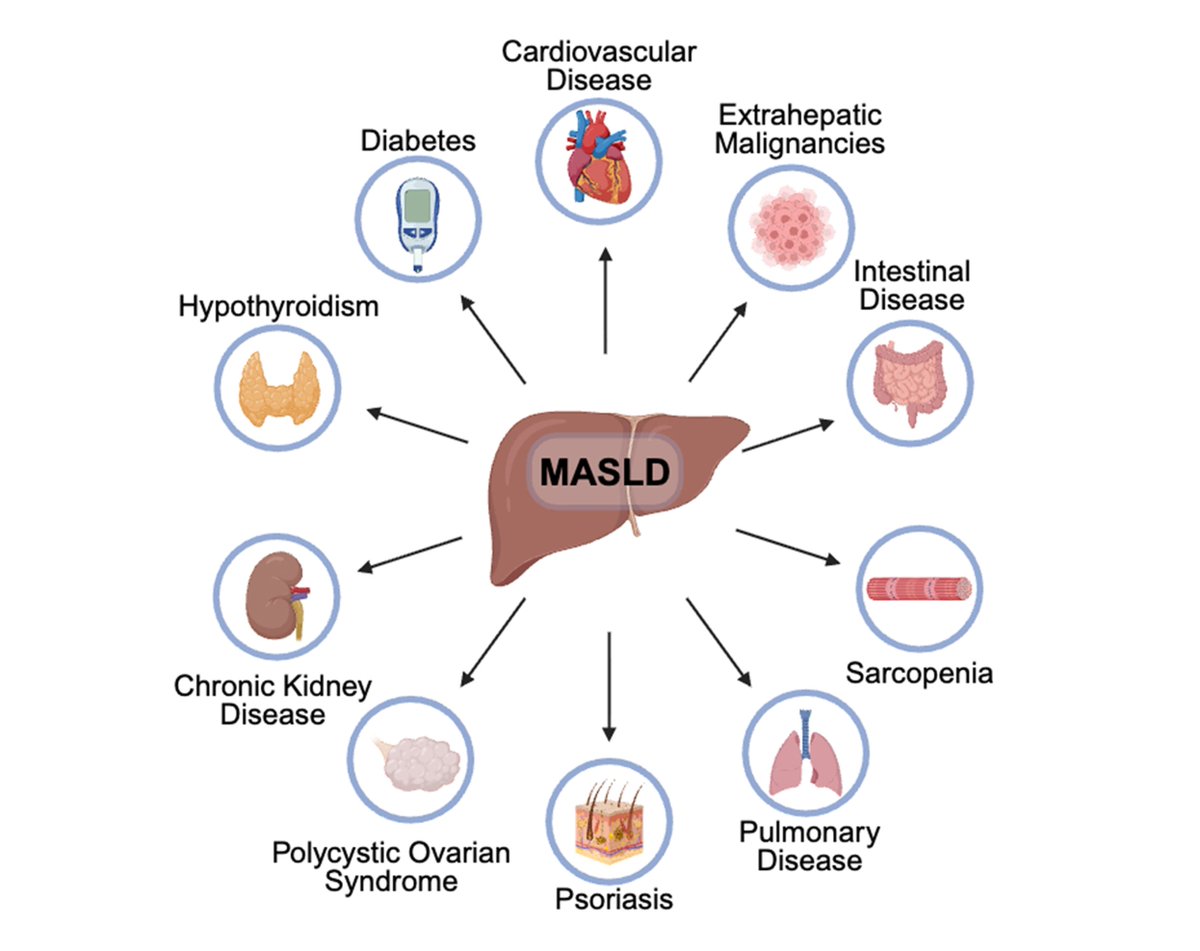
New review frames insulin resistance as the crossroads of metabolic inflammation, MASLD/MASH, CVD, organ failure & cancer. Simply “fixing IR” is necessary but not sufficient once the dysmetabolic fire is lit.
https://t.co/XFiMM7zMEL
🚨This week's #WednesdayWebinar – Management of epithelial precancerous conditions and early neoplasia of the stomach (MAPS III): Case-based highlights
📆 Wed, Dec 3, 19:00 CET
🔗https://t.co/Cymhr9qTAN
Explore Clinical cases that illustrate key concepts & practical approaches