🫀 Pulmonary vein anatomy is more variable than many clinicians realize.
Pulmonary veins are not only an anatomical structure—they represent the principal arrhythmogenic region in atrial fibrillation, harboring approximately 85% of AF triggers and 50% of the arrhythmogenic substrate. ⚡
📊 Common anatomical variants include:
🔹 Four separate pulmonary veins (70%)
🔹 Left common pulmonary vein trunk (30%)
🔹 Right middle pulmonary vein (20%)
🔹 More than four pulmonary veins (10%)
🔹 Right common pulmonary vein trunk (5%)
🔹 Other variants (5%)
Recognition of these anatomical patterns is essential for accurate imaging interpretation, procedural planning, and successful pulmonary vein isolation. 🎯
📖 Full AF guidelines (2026) 👉 https://t.co/YiCSHVTZ3y
#cardiology #medicaleducation #paramedic #MedstudentTwitter #CardioTwitter #FOAMed #MedEd #CardioEd #AFib #EPeeps
📄 Can CT + AI improve the diagnosis of Marfan and Loeys-Dietz syndromes?
🔗 DOI: https://t.co/rqUJN463Zm
🧠 Diagnosing heritable thoracic aortic diseases (HTAD) remains challenging—especially when classical criteria are inconsistent or delayed.
This study introduces a machine learning–based CT approach to redefine dural ectasia (DE) and improve diagnostic accuracy.
✨ Why this matters:
👉 Dural ectasia is part of the Ghent criteria, but:
❗ No standardized definition
❗ Poor specificity
❗ Limited diagnostic value in practice
✨ Study highlights:
📊 Cohort:
93 Marfan patients (FBN1 variants)
Loeys-Dietz cohorts (TGFBR1/2, SMAD3)
Matched controls
🔍 Key innovation:
👉 A machine learning algorithm based on just:
✔ 3 vertebral levels (L1, L2, S1)
✔ 4 simple CT measurements:
Spinal canal diameter
Vertebral scalloping
➡️ Designed for accuracy + clinical usability
📈 Results:
🔹 Conventional DE criteria → poor performance
➡️ AUC ≈ 0.68
🔹 New ML-based criteria:
➡️ AUC 0.84 for Marfan
➡️ Accuracy up to 94%
➡️ Outperformed modified Ghent criteria
🔹 Also effective for Loeys-Dietz:
➡️ AUC 0.83 (TGFBR1/2)
➡️ AUC 0.80 (SMAD3)
💡 Clinical implications:
👉 A simple CT scan (already done for aorta evaluation) can now:
✔ Improve early diagnosis
✔ Reduce reliance on delayed genetic testing
✔ Enable earlier referral and management
🚀 Bonus:
👉 A user-friendly online tool provides probability of diagnosis based on CT measurements
🚨 Bottom line:
Machine learning transforms dural ectasia from a weak criterion into a powerful, practical diagnostic tool for Marfan and related syndromes.
#Cardiology #CardiacImaging #CT #ArtificialIntelligence #MarfanSyndrome #LoeysDietz #Aortopathy #PrecisionMedicine #MedicalInnovation 🧠🫀📊
Our ESC Clinical Consensus Statement on Women’s Heart Centres is published in @EurHeartJ merging 4 associations @EACVIPresident@EAPCIPresident@HFA_President@ACVCPresident
Link ➡️ https://t.co/xLwBaHexh9
ESC press release ➡️ https://t.co/SAjnOuePpZ
This is the first statement to define what a Women’s Heart Centre actually is: its structure, its team, its referral pathways, and the training standards clinicians need to lead one.
The problem: CVD is the #1 killer of women. Yet women face systematic delays in diagnosis and treatment and the conditions most likely to affect them (INOCA, MINOCA, pregnancy-related CVD) remain underdiagnosed everywhere.
Our solution: hub-and-spoke Women’s Heart Centres, embedded in existing CV systems, not parallel structures. Advanced diagnostics, multidisciplinary care, research coordination.
For the first time we define:
✅ The nucleus clinical team
✅ Adjunct specialties (cardio-obstetrics, oncology, rheumatology, psychology and more)
✅ Core vs advanced competencies
✅ A pathway toward subspecialty certification
We also set milestones for national and institutional adoption.
This has been a Herculean effort and an important task to lead this document with enormous gratitude to senior author @DrMarthaGulati for her mentorship and friendship - really grateful to @Drroxmehran@rafavidalperez@mmamas1973@HeartDocSharon@Bharatishivalka@PrSusannaPrice1@Cosyns@VictoriaDe32503@d_trabattoni@Marta33717088@ARakisheva@yappelman@mirvatalasnag@lesleejshaw@alessia_gimelli
#WomensHealth
#Cardiology
#WomensHeartDisease
#CardioTwitter
#ESC
#EACVI
#HeartDisease
#WomensHeartCentre
#CVD
#CardioEd
📄 4D-flow CMR meets diastology: can we finally assess E/e′ with MRI?
🔗 DOI: https://t.co/RH5Q07U7FM
🫀 Diastolic dysfunction (DD) is a key early marker of heart disease—but CMR has traditionally struggled to assess it.
This study introduces a novel solution:
👉 CMR-derived 4D-flow E/e′ for biventricular diastolic function assessment
✨ What’s new?
👉 Combines:
✔ 4D-flow transvalvular velocity (E)
✔ CMR-derived tissue velocity (e′)
➡️ Recreating the classic echo parameter (E/e′) using MRI
📊 As shown in the graphical abstract (page 2):
👉 simultaneous evaluation of LV + RV diastolic function
✨ Study at a glance:
🔹 132 participants
75 healthy controls
57 CVD patients
🔹 Full biventricular assessment with 4D-flow + strain/annular motion
✨ Key findings:
📈 4D-E/e′ is higher in CVD patients
➡️ reflecting impaired relaxation
📊 Excellent diagnostic performance:
➡️ LV DD detection: AUC ~0.90
📌 Best method:
👉 annular velocity–based e′
📉 Hidden disease uncovered:
👉 Among patients WITHOUT prior diastolic assessment:
➡️ 71% had abnormal LV diastolic function
➡️ 61% had abnormal RV diastolic function
⚠️ A major proportion of DD is currently missed in clinical practice
📊 Strong validation vs echocardiography:
✔ E velocity: r = 0.81
✔ E/e′: r = 0.77
➡️ As shown in Figure 3 (page 6):
👉 strong correlation with echo
🧠 Why this matters:
👉 CMR already performed in many patients
➡️ Now it can also provide:
✔ diastolic function assessment
✔ biventricular evaluation
✔ detection of early/subclinical disease
⚡ Key innovation:
👉 First robust demonstration of:
integrated flow + tissue metric (4D-E/e′) using CMR
➡️ Overcomes limitations of:
❗ 2D flow
❗ static imaging planes
💡 Clinical take-home message:
👉 CMR is no longer “systolic-only”
✔ 4D-flow enables comprehensive haemodynamic assessment
✔ Can detect undiagnosed diastolic dysfunction
🚨 Bottom line:
4D-flow CMR brings echocardiographic E/e′ into MRI—unlocking a new era of full functional cardiac assessment.
#Cardiology #CMR #4DFlow #DiastolicDysfunction #HeartFailure #CardiacImaging #EoverEprime #PrecisionMedicine #DigitalHealth 🫀📊
#CardioNuggets™
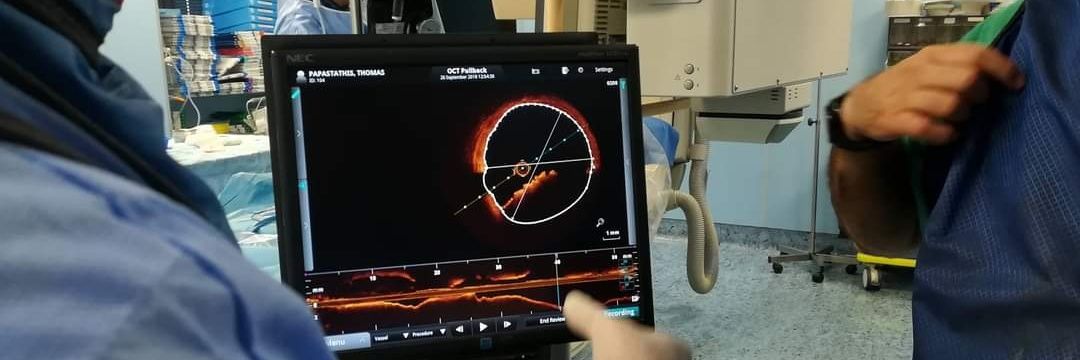
Microvascular obstruction (MVO)
After a STEMI, restoring epicardial flow with PCI doesn’t always mean true myocardial reperfusion. In >40% of reperfused MIs, the downstream coronary microcirculation is damaged/plugged by:
• distal embolization of thrombus/plaque
• endothelial swelling
• inflammation & edema
• capillary destruction
➡️ Result: blood can’t adequately enter the infarcted myocardium despite a patent epicardial artery (“no-reflow phenomenon”).
Why it matters:
MVO is a marker of severe reperfusion injury and predicts:
• larger infarct size
• adverse LV remodeling
• lower EF recovery
• HF admissions
• ventricular arrhythmias
• higher mortality
How is it diagnosed?
🩺 Angio clues: slow/no-reflow despite open vessel (↓TIMI myocardial perfusion grade)
🫀 Echo: poor myocardial contrast replenishment on myocardial contrast echo
📍Gold standard = Cardiac MRI
• seen as a dark hypoenhanced core within bright late gadolinium enhancement infarcted tissue
• early MVO = first-pass perfusion defect
• late MVO = persistent dark core on LGE images
High-yield pearl:
A patient can have TIMI 3 flow after PCI and still have major myocardial injury because the microvasculature never truly reperfused.
#CardioNugget #MedEd
Image source: https://t.co/vcgvUTP00s
7 Sci-Hub Alternative Websites
Paper you need to ask for payment & can't use sci-hub?
You don't have to pay to read academic papers.
These are 7 sci-hub alternative websites to download papers for free.
👉 Unpaywall --> https://unpaywall. org/
Install this browser extension on Chrome and read the paper directly on the journal website legally and for free.
👉 Open Access Button (OAB) --> https://lnkd. in/dXVVQpUf
Copy and paste the link paper or DOI on the OAB website. This will be accessible on the next page. Legal.
👉 PaperPanda --> https://paperpanda. app/
Like Unpaywall, this Chrome extension allows you to access millions of research papers in one click.
👉 DOAJ --> https://doaj. org/
As the name implies, DOAJ (Directory of Open Access Journals) provides access to millions of scientific papers from around the world for free.
👉 OA[.]mg--> https://oa. mg/
Like Google which is made specifically to search for academic papers. There are more than 250 million papers available for access.
👉 Core --> https://core. ac. uk/
The world's largest database of research papers with more than 298 million papers from around the world that can be accessed for free.
👉 arXiv --> https://arxiv. org/
Especially for lovers of natural sciences and economics, this website provides access to 2.4 million academic papers for free.
Tip: Remove any spaces in the URLs if you encounter issues accessing the websites.
🫀 SPIRIT-HF at #ACC26: Spironolactone, an aldosterone blocker, compared with placebo, did not show any significant improvement in terms of HF hospitalizations and cardiovascular death at 24 months in patients with #HFpEF or #HFmrEF.
See the results ➡️ https://t.co/OVTyBhYHfM
Among patients with acute #HF in the #CLOROTIC#RCT
💠 #Diuretic resistance -> worse outcomes
💠#Hydrochlorthiazide effect on weight loss was consistent across categories of diuretic resistance
Trial led by @jc_trullas, subanalysis by Ambarish Pandey
https://t.co/gkQAoZClIV
🫀🔥 Post–Cardiac Injury Syndrome (PCIS): a true paradigm shift in care
This 2025 JACC: Advances State-of-the-Art Review reframes post–cardiac injury syndrome (PCIS) as a modern, increasingly relevant inflammatory disease—no longer a rare post-MI curiosity, but a frequent consequence of today’s cardiac procedures .
🧩 What is PCIS today?
PCIS includes:
🫀 Post–myocardial infarction syndrome (Dressler)
🩺 Post-pericardiotomy syndrome (PPS)
🧷 Post-traumatic / iatrogenic pericarditis
With the explosion of cardiac surgery, PCI, device implantation, and ablation, PPS and post-traumatic pericarditis now dominate—while classic Dressler syndrome has become rare.
🧠 Pathophysiology: inflammation at the core
PCIS is driven by an autoinflammatory immune response triggered by myocardial or pericardial injury:
DAMPs → NF-κB activation
NLRP3 inflammasome → IL-1α / IL-1β releaseThis explains why targeted anti–IL-1 therapies work in refractory disease.
🖥️ Diagnosis: imaging changes everything
Symptoms and biomarkers are nonspecific. The real shift is multimodality imaging:
🩻 Echo → effusions, hemodynamics
🖥️ CT → pericardial thickness, effusion characterization
🧲 CMR (game-changer) → edema + LGE = active inflammation
CMR enables diagnostic confidence, phenotyping, and therapy guidance.
💊 Treatment: from empiric to precision
First line: NSAIDs + colchicine
Steroids: selective use only
🚀 Refractory cases: IL-1 inhibitors (anakinra, rilonacept)
Emerging oral agents targeting NLRP3 are on the horizon
⚠️ Key limitations
Access to CMR and biologics is uneven; costs and equity remain major barriers.
🔮 Bottom line
PCIS care is shifting from symptom-based treatment to imaging-guided, mechanism-based precision medicine.
Less guessing. More biology. Better outcomes.
🫀🔥 Acute myocarditis in daily practice: what clinicians really need to know
This 2025 European Heart Journal – Acute Cardiovascular Care expert review offers a rare, practical roadmap for managing acute myocarditis (AM)—a condition that remains highly heterogeneous, unpredictable, and frustratingly evidence-poor .
🧠 Why myocarditis is so challenging
Acute myocarditis is not one disease but a spectrum: from mild, self-limiting chest pain to fulminant cardiogenic shockin young patients. Despite advances in imaging, virology, and genetics, specific therapies are still largely lacking, and management relies heavily on expert judgment.
🏥 First decision: who needs hospital care—and where?
Risk stratification is key:
⚠️ High-risk features (shock, ventricular arrhythmias, AV block, severe LV dysfunction) → Level 3 CICU
🟡 Intermediate risk → Level 2 monitoring
🟢 Truly low risk → short observation or ward care
The review strongly advocates for a multidisciplinary “myocarditis team”, especially in unstable patients.
🖥️ Imaging hierarchy
Echo → first-line for function and complications
CMR → gold standard for diagnosis (updated Lake Louise criteria) and prognosis
Coronary angiography / CCTA → essential to rule out ACS
PET & spectral CT → emerging tools for complex cases
🧪 Endomyocardial biopsy: when it matters
EMB is not routine, but crucial in:
fulminant or recurrent myocarditis
persistent LV dysfunction
suspected eosinophilic, giant cell, or immune checkpoint inhibitor–related forms
💊 Treatment: less certainty than we’d like
Supportive HF therapy is central
Immunosuppression is not routine—reserved for selected phenotypes
Mechanical circulatory support can be lifesaving as a bridge to recovery
🏃 Discharge & activity
Exercise restriction for 3–6 months is advised, especially if LGE or LV dysfunction persists—though evidence remains weak.
🔮 Bottom line
Acute myocarditis demands early recognition, structured triage, team-based care, and humility about evidence gaps.
Until RCTs deliver answers, expert-driven, phenotype-based management remains the best tool we have 🧭
🫀🧠 HFpEF is not just “diastolic dysfunction”: the microcirculation is the missing link
This 2025 JACC: Advances state-of-the-art review reframes heart failure with preserved ejection fraction (HFpEF)through a crucial, often underrecognized lens: coronary microvascular dysfunction (CMD) .
📊 How common is CMD in HFpEF? Very.
Up to 75% of HFpEF patients—even without obstructive coronary disease—have CMD. And this is not an innocent bystander:
CMD is independently associated with higher HF hospitalizations
Increased mortality and MACE
Worse quality of life
Yet, CMD is rarely sought and even more rarely diagnosed in routine HFpEF care.
🧠 Why CMD matters pathophysiologically
CMD disrupts the heart at multiple levels:
🔻 Reduced coronary flow reserve (CFR) → subendocardial ischemia
🔥 Microinfarctions & fibrosis → stiff myocardium
⚙️ Impaired cardiac–coronary coupling → blunted flow during stress
🧬 Inflammation & endothelial dysfunction → vicious cycle of ischemia and diastolic failure
HFpEF and CMD reinforce each other in a bidirectional loop, rather than a simple cause–effect relationship.
👩⚕️ A sex-specific disease
Women are disproportionately affected:
Higher CMD prevalence
Smaller coronary vessels, higher resting flow
Postmenopausal estrogen loss → inflammation, fibrosis, reduced CFR
This helps explain why HFpEF is more common and more complex in women.
🧪 Diagnosis: we’re under-testing
CMD can be assessed by:
PET or CMR perfusion
Invasive coronary functional testing (CFR, IMR, acetylcholine)
But there is no standardized diagnostic pathway in HFpEF—yet.
💊 Therapy: signals, not solutions
Some treatments show promise (SGLT2i, statins, RAAS modulation, lifestyle, GLP-1/GIP agonists), but no therapy specifically targets CMD in HFpEF so far.
🔮 Bottom line
HFpEF is not only a myocardial disease—it’s a microvascular disease.
If we keep ignoring CMD, we will keep failing HFpEF patients.
👉 Understanding and treating HFpEF may finally require looking beyond the ventricle—into the microcirculation.
#EHJIMP 🫀 📊 Severe AS significantly alters supra-aortic blood flow velocities on duplex ultrasound. Findings suggest that carotid ultrasound velocity thresholds may underestimate internal carotid artery stenosis severity in patients with concomitant aortic stenosis. https://t.co/MUfnUvHoq1
#EHJIMP ⏳✨
–7 | End-of-year countdown of the most cited articles 📉📚
On Christmas Day at number 5, another highly influential article that has made a strong impact in cardiovascular imaging, contributing to scientific progress and clinical practice 🫀🖥️📈
🔗 DOI: 10.1093/ehjimp/qyaf054
#CardiovascularImaging #TopCited #ScientificImpact #HeartImaging #Echo #CMR #CardiacCT #ResearchHighlights #EndOfYearCountdown ✨


































![ScholarshipfPhd's tweet photo. 7 Sci-Hub Alternative Websites
Paper you need to ask for payment & can't use sci-hub?
You don't have to pay to read academic papers.
These are 7 sci-hub alternative websites to download papers for free.
👉 Unpaywall --> https://unpaywall. org/
Install this browser extension on Chrome and read the paper directly on the journal website legally and for free.
👉 Open Access Button (OAB) --> https://lnkd. in/dXVVQpUf
Copy and paste the link paper or DOI on the OAB website. This will be accessible on the next page. Legal.
👉 PaperPanda --> https://paperpanda. app/
Like Unpaywall, this Chrome extension allows you to access millions of research papers in one click.
👉 DOAJ --> https://doaj. org/
As the name implies, DOAJ (Directory of Open Access Journals) provides access to millions of scientific papers from around the world for free.
👉 OA[.]mg--> https://oa. mg/
Like Google which is made specifically to search for academic papers. There are more than 250 million papers available for access.
👉 Core --> https://core. ac. uk/
The world's largest database of research papers with more than 298 million papers from around the world that can be accessed for free.
👉 arXiv --> https://arxiv. org/
Especially for lovers of natural sciences and economics, this website provides access to 2.4 million academic papers for free.
Tip: Remove any spaces in the URLs if you encounter issues accessing the websites.](https://pbs.twimg.com/media/HE69ZiEb0AAQR6M.png)
![AHAScience's tweet photo. Key updates to this guideline include:
➡️ The use of the American Heart Association PREVENT-ASCVD equations to guide primary-prevention and lipid-lowering therapy decisions.
➡️ Testing Lp(a) at least once in a lifetime and selective apolipoprotein B measurement to improve risk assessment and guide treatment
➡️ The return of LDL-C and non-high-density lipoprotein cholesterol treatment goals (with lower targets for higher-risk groups)
➡️ Expanded use of coronary artery calcium scoring to reclassify risk[ME1.1]
✍🏼 @rblument1 @tygluckman @RonBlankstein @PamelaBMorris @pnatarajanmd @AnnMarieNavar @SethShayMartin @APRN_CNS @nyulangone @DrMichaelShapir @kgradneyrd @eugeniagianos @virani_md @KellieMcLain1 @ijeomaheartdoc @SamiaMoraMD @DrHeatherJohn @dmljmd](https://pbs.twimg.com/media/HDPXv0SXsAIEPMD.png)