Most doctors don’t have a time problem.
They have a systems problem.
The careers that compound aren’t built on motivation.
They’re built on small actions repeated for years.
📖 Read the full article below 👇
Congratulations to Manju Sengar on being the recipient of the "International Women Who Conquer Cancer Mentorship Award"
https://t.co/RNz0LgURJg
@HCC_HemeCancer@jayastuMD@NitinJainMD
Newer clinicians may not know this or appreciate how important this is : Acidosis, particularly with a pH <7.20 , significantly impairs the effectiveness of vasopressors by reducing vascular reactivity to catecholamines (norepinephrine, epinephrine) and decreasing cardiac contractility. This leads to refractory hypotension and worsened shock. The primary management focus is reversing the underlying cause of acidosis. Bicarbonate will temporize->but you need to get to the route problem.
When someone is hypotensive-it’s often or commonly multifactorial. When addressing it - you must pull the appropriate levers. Address each individual contributor. Is the patient on calcium channel blocker, but also now septic ? Consider reversing it with CaCL.
Blood pressure is mediated by the tank (volume), the pump (LVEF), heart rate, and vascular tone (peripheral resistance). The reason why zestoretic and entresto are so powerful at treating HTN is they attack 2 of the levers at the same time.
You should optimize each lever in treating shock/hypotension. People with profound shock shouldn’t have a HR in the 50s. Treat ALL reversible causes that maybe contributing. Don’t just treat hypotension. It’s a vital sign… when vital signs are abnormal ask yourself why is it abnormal! There is a differential diagnosis. Each pressor pulls each level with different strength. Don’t engage in pharmacological warfare! Avoid dilt drips for afib when the patient is in shock on pressors. @HeartOTXHeartMD@MKIttlesonMD@DrMarthaGulati@kidney_boy
Pay attention to the kidneys often they are smarter than you are. IF you notice hourly UOP trending down (less than 30cchr) please make sure the MAP is sufficient and the tank is adequate.
Some practicing pearls from the front line.
Given the heartwarming response to the Foundation Day photo of @TataMemorial, here are some details on the founding of this remarkable institute. Tata Memorial Hospital was inaugurated on 28 February 1941, as Asia’s first comprehensive cancer hospital.
Parentalism instead of paternalism - what a perfect term @adamcifu. Thanks for writing this!
The practice of giving clear guidance regarding the best course of action, based on knowledge, beneficence, & familiarity with patient values.
https://t.co/LCPshiF9tZ
Grateful to our Paediatric Oncology team for making this happen: one of our children with an incurable cancer had two last wishes: meet MS Dhoni, and ride a @Lamborghini. Today, we could make one of these happen. If any of you have contacts with MSD, pls connect us.
IT IS THIS TIME OF THE YEAR AGAIN!
TOP 10 GU clinical trials in 2025!
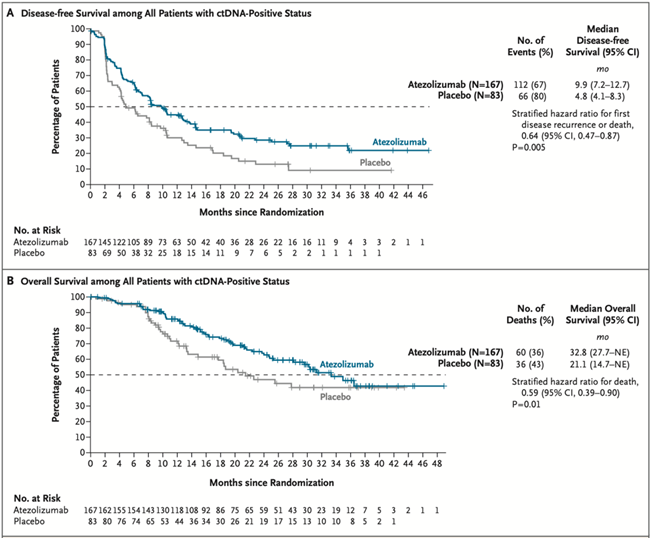
1/ Practice-changing IMvigor011: In ctDNA+ MIBC post-cystectomy, adjuvant atezo improved DFS (HR 0.64) & OS (HR 0.59) vs placebo. ctDNA- pts spared therapy w/ 2-yr DFS ~88%.
@tompowles1@DrYukselUrun@OncoBellmunt@NEJM #ESMO2025 Plenary @myESMO
https://t.co/mbl2VKLZ2N
Among pts with ER+/HER2+ MBC, maintenance HP (control arm) had a PFS of:
-29.1 mo in PATINA
-16.3 mo in HER2CLIMB-05
The difference? In PATINA all pts also received ET (only 45% in H2C-05).
Reminder that, besides fancy new drugs, ET can REALLY make a difference in this disease!
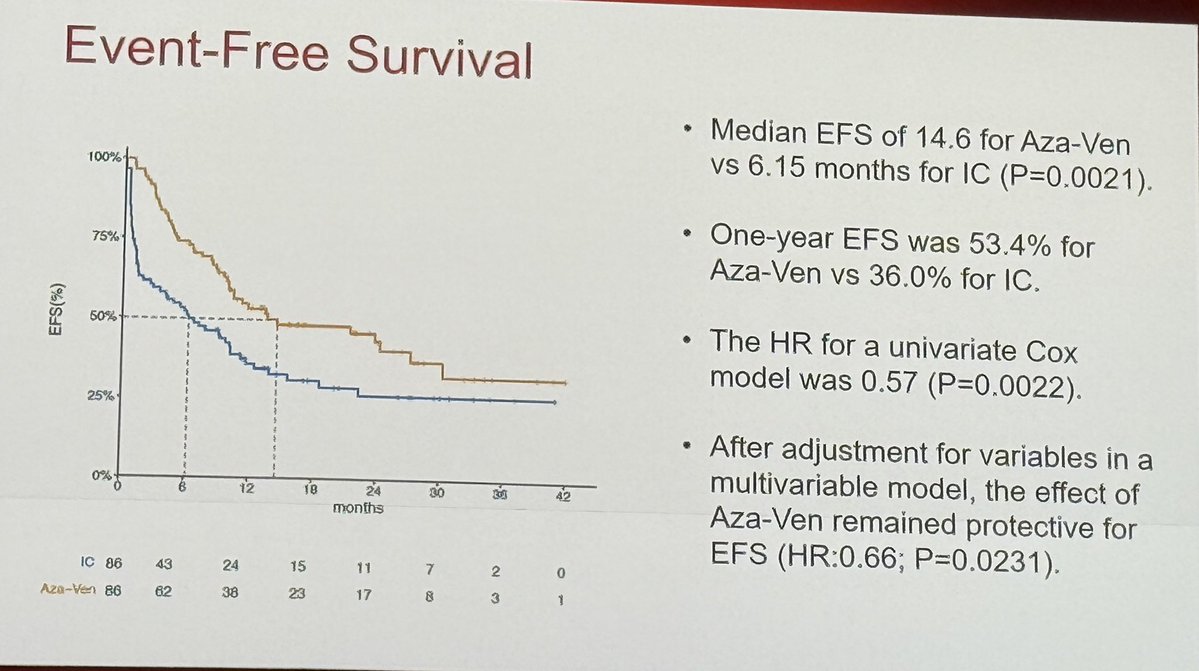
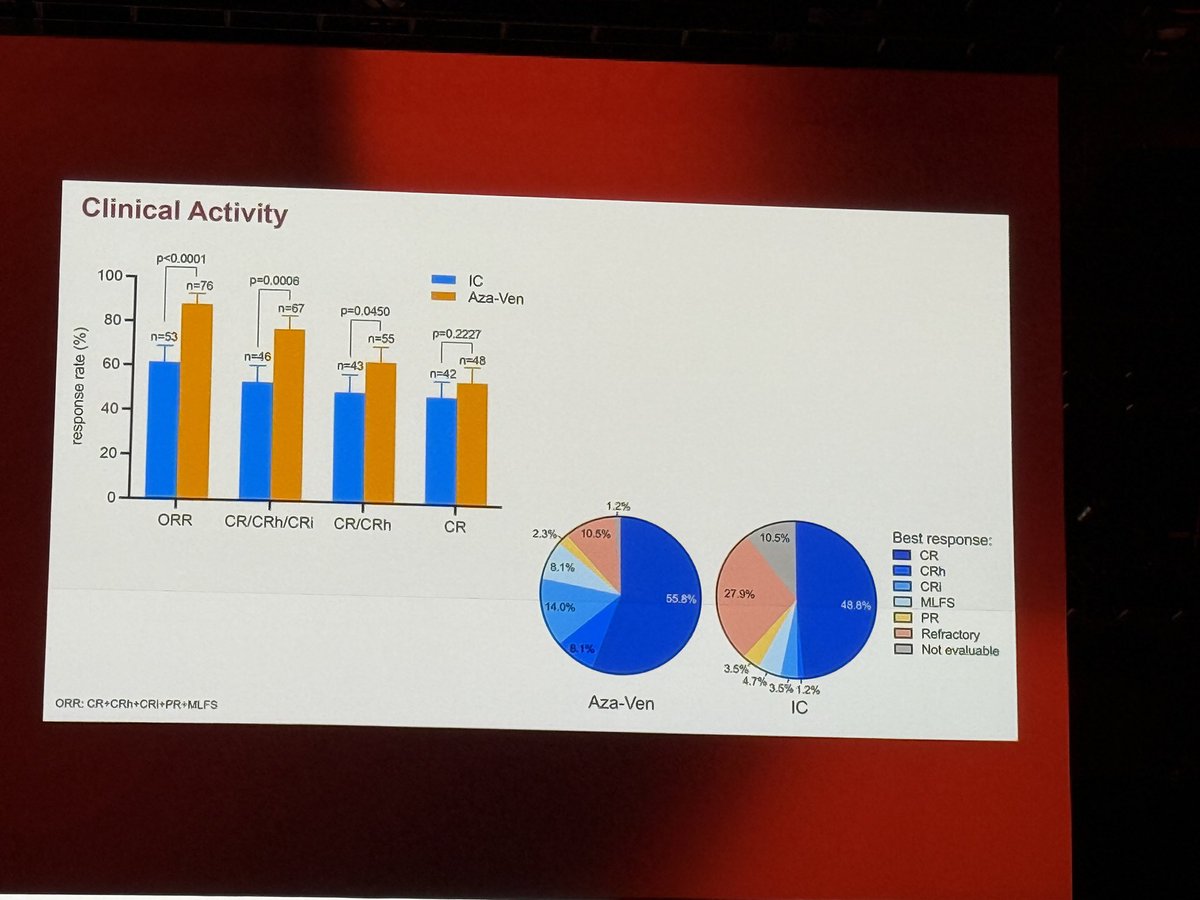
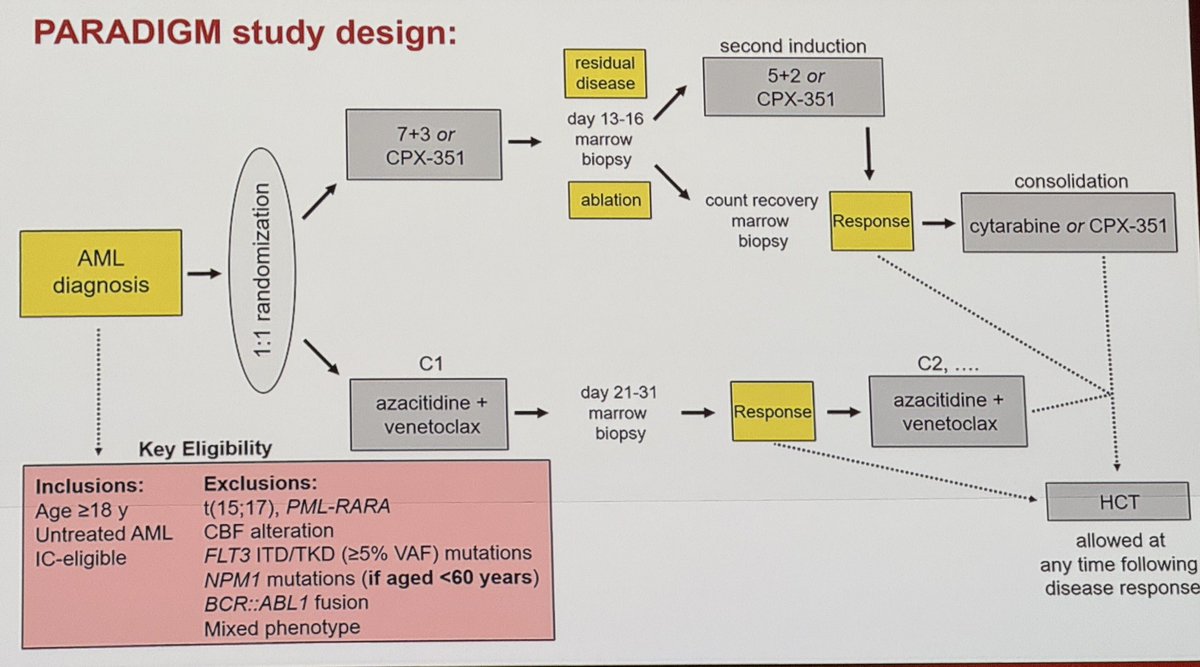
#ASH25#ASHPlenary#PARADIGM trial
Great work, congratulations to Dr. Fathi and colleagues! #AML#leusm
Summary:
The study met PE for EFS.
Higher ORR and CR in VEN+AZA gp
More pt received transplant in VEN+AZA gp
Better QOL
The first new adjuvant endocrine treatment to improve outcomes for breast cancer in decades. Tucatinib improving outcomes in the first line HER2+ setting. First phase 3 data with SG in chemo-naive pts with HR+ MBC. And so much more. See you in a few days in San Antonio! #SABCS25
Just published in @CancerMedicine
15 years of PBSC mobilization experience in Myeloma
Even in the CAR-T era, collecting sufficient PBSCs is crucial.
- GCSF+plerixafor comparable to chemo mobilization
- If prior RT (to hematopoietic sites - spine, pelvis), chemo-mobn is better