Big congrats our BCAN Quale Fellows. And thank you to all the reviewers in this incredibly competitive application cycle We are fortunate to be in a golden age of bladder cancer progress. Thrilling to see that we are able to recruit such talent to the field.
@BladderCancerUS
Congratulations to the 2026 John Quale Travel Fellowship recipients! We are proud to support the next generation of bladder cancer researchers and clinicians as they join us at the 2026 Bladder Cancer Think Tank. Your dedication to advancing bladder cancer research will help shape the future of patient care. @UofCalifornia@MSKCancerCenter@WeillCornell@Yale@theNCI@UW@MoffittNews@UHhospitals
Interesting thought experiment. If you take the 5% absolute difference in RFS, and instead give BCG +IO as reinduction after the 10% of all patients recur at 3mo, would you get same benefit of IO and limit toxicity/over treatment? @WesKassouf@UroDocAsh
Agree. The other question is does combo therapy for all outperforms sequential therapy for only some ( ie bcg for hr-nmibc then IO upon HG recurrence). I have not yet seen convincing data to suggest outcomes would be different between the two approaches
Agree. The other question is does combo therapy for all outperforms sequential therapy for only some ( ie bcg for hr-nmibc then IO upon HG recurrence). I have not yet seen convincing data to suggest outcomes would be different between the two approaches
6. Finally, we need to better understand why Alban was negative, CREST was marginally positive but company pulled FDa registration for now (unclear exactly why) & POTOMAC approved based on marginal improvements
7. Multiple trials in same space force us to interpret collectively
1) Approval based on marginal improvements in efficacy (without improvement to CSS/OS)
2) Toxicity that isn't G5 (death) doesn't seem to impact approval. 10-15% serious autoimmune AEs in NMIBC is deemed ok
3) little weight given to efficacy vs toxicity balance of a drug
4. Any NMIBC patient I am considering for early cystectomy i think reasonable to consider BCG +IO if patient wants bladder preservation
5. Trials didn't address who is highest risk, but we know multifocal HGT1 w/CIS is the bad actor so these folks who may benefit. Time will tell
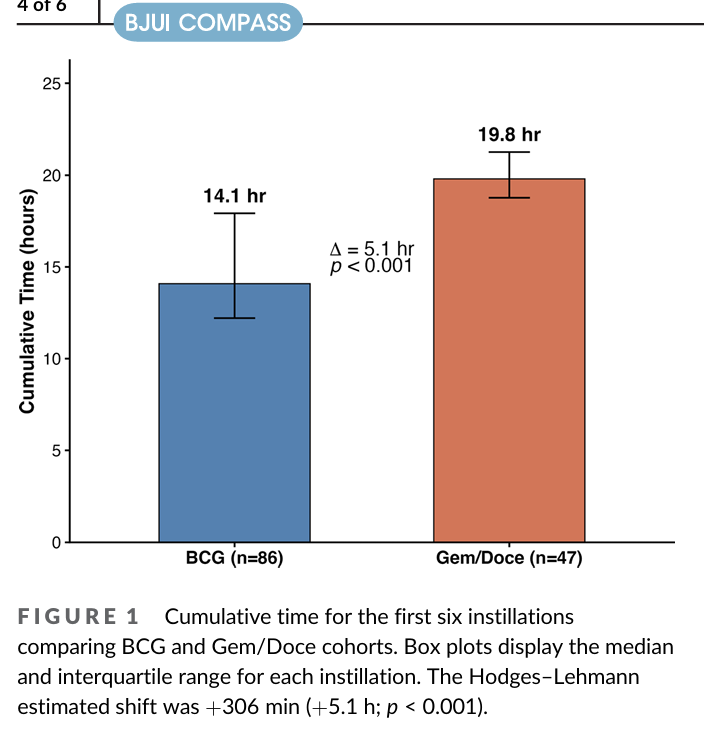
If BRIDGE shows non-inferiority (I think likely)... need to choose treatments in real world. One of main issues if Gem/Doce is logistics, especially in community.
But there is also a time burden on the patient which can impact shared decision making
https://t.co/zyzToUgypq
Collaboration in Action!
Our Working Groups bring together multidisciplinary experts committed to advancing bladder cancer research and care. Together, we’re tackling the most pressing challenges and turning ideas into impact.
Stay tuned to learn more about the people/progress
View our schedule for the final day of #AUA26!
Thank you to everyone from @brady_urology who presented, attended, and contributed to the #AUA26 Annual Meeting!
You can find our full AUA schedule and more resources for clinicians here: https://t.co/RgYW0IkIUo
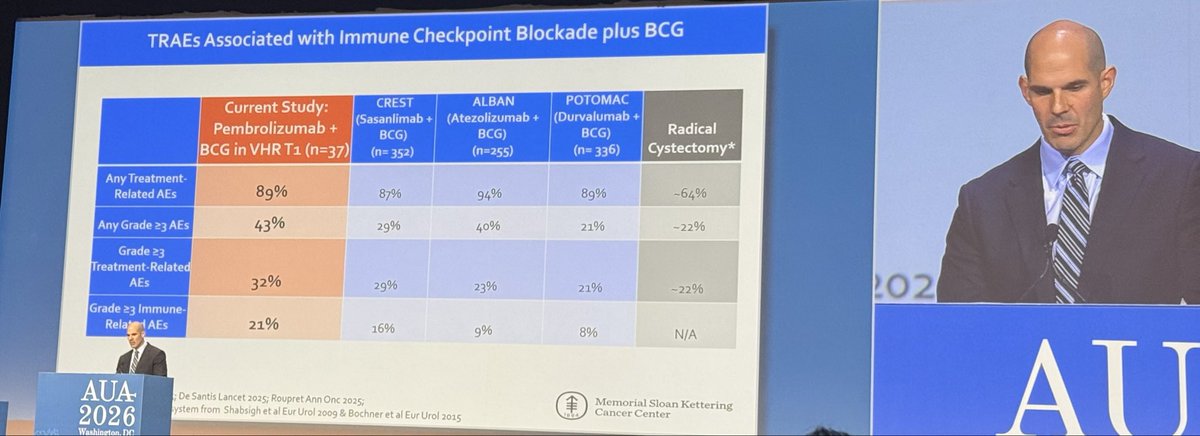
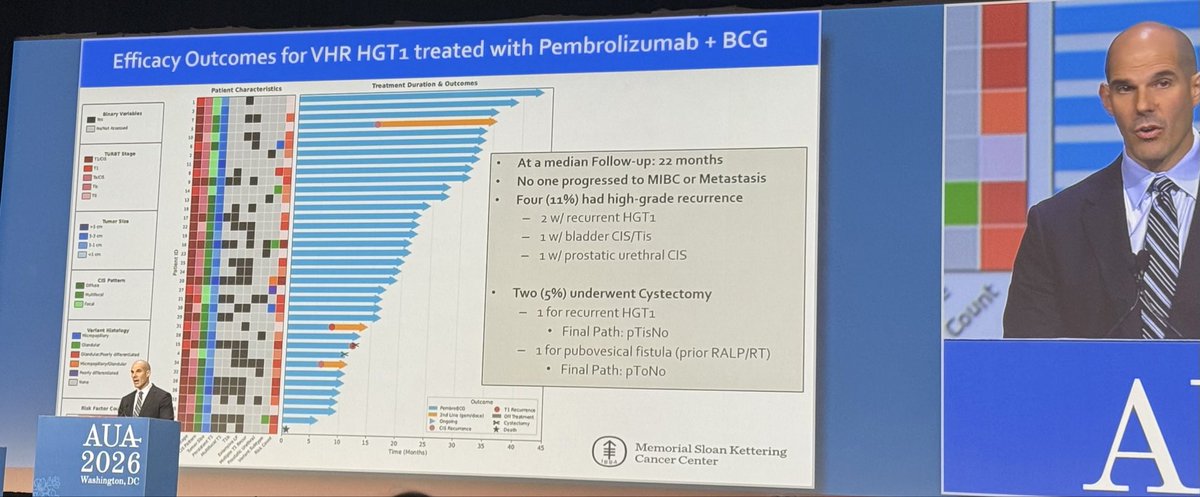
@eugene_pietzak incrediblely elegant P2 on bcg + Pembro in VHR T1. 92% response, 94% RC- free. 1 early death and 21% iAEs. n=37 but great job to consider risk - based strategy. #AUA26
The #EMBRACETrial: An enhanced recovery after surgery pathway for transurethral resection of bladder tumors. @mihiggins22 & @MaxKates@brady_urology join @UroCancerMD to discuss an enhanced recovery protocol for ambulatory TURBT which improved Quality of Recovery-15 scores by 12 points—well above the 6-point clinical significance threshold—and reduced urethral pain, dysuria, incontinence, and 30-day outpatient visits. #WatchNow to learn more > https://t.co/I9sK9TBuwX
The #EMBRACETrial: An enhanced recovery after surgery pathway for transurethral resection of bladder tumors. @mihiggins22 & @MaxKates@brady_urology join @UroCancerMD to discuss an enhanced recovery protocol for ambulatory TURBT which improved Quality of Recovery-15 scores by 12 points—well above the 6-point clinical significance threshold—and reduced urethral pain, dysuria, incontinence, and 30-day outpatient visits. #WatchNow to learn more > https://t.co/I9sK9TBuwX
An exciting step toward more personalized, precise care! Dr. Armine Smith (GBCI) is advancing AI-driven biomarkers for bladder cancer. This real-world study highlights how AI can support clinical decision making and is already gaining global attention. https://t.co/wVNMtjnwhS
Reintroducing the GBCI.
Bringing together global, multidisciplinary experts to drive innovation in research, prevention, and treatment. Focused on bladder, upper tract urothelial cancer, and women’s bladder cancer.
Understand. Prevent. Cure.
May is Bladder Cancer Awareness Month 🎗️Learn the facts about bladder cancer, including who’s at risk, how it's diagnosed, and the latest treatment options.
Bladder Cancer Q&A | Max Kates, M.D. https://t.co/kqDqVdXd87 via @YouTube