I hereby submit my twitter petition for all journal article pdfs to automatically include the supplementary materials at the end. Extra clicks + pain of organizing extra PDFs >>> a few extra wasted KB of hard drive space @JUrology
First ever locally injectable immunoactive agent with proven DFS benefit in localized prostate cancer.
Tandem randomized Phase II in surveillance forthcoming.
Origin: Baylor basic science lab (support research!)
https://t.co/gGOjo9eMa5
*maybe* FDA will approve based on MFS, but significant doubt will remain among treating docs (myself included) without OS data -- even if we heed @DrSpratticus's main point here and use conventional imaging to define MFS.
Discussion around PROTEUS highlights lack of consensus in accepting MFS as a surrogate endpoint for OS for perioperative systemic therapy trials. hopefully this will drive trials to follow long enough to get OS.
4/n #ASCO26
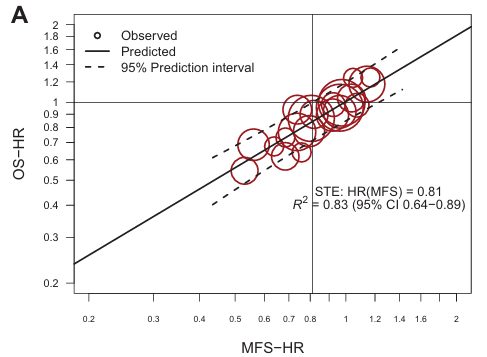
The ICECaP group (@ChrisSweens1) showed using semi-newer trials than the original publication, a slightly weaker treatment effect correlation of MFS and OS, with a surrogate threshold effect (STE) of 0.81 (more on this shortly!). Notably almost none of these trials are surgery trials. The only surgery trial of RP+/- systemic therapy included was CALGB90203.
Surrogacy is treatment and disease state specific.
Ignoring this, MFS was based on conventional imaging.
@AmarUKishan@I_Migowski@TylerSbrt
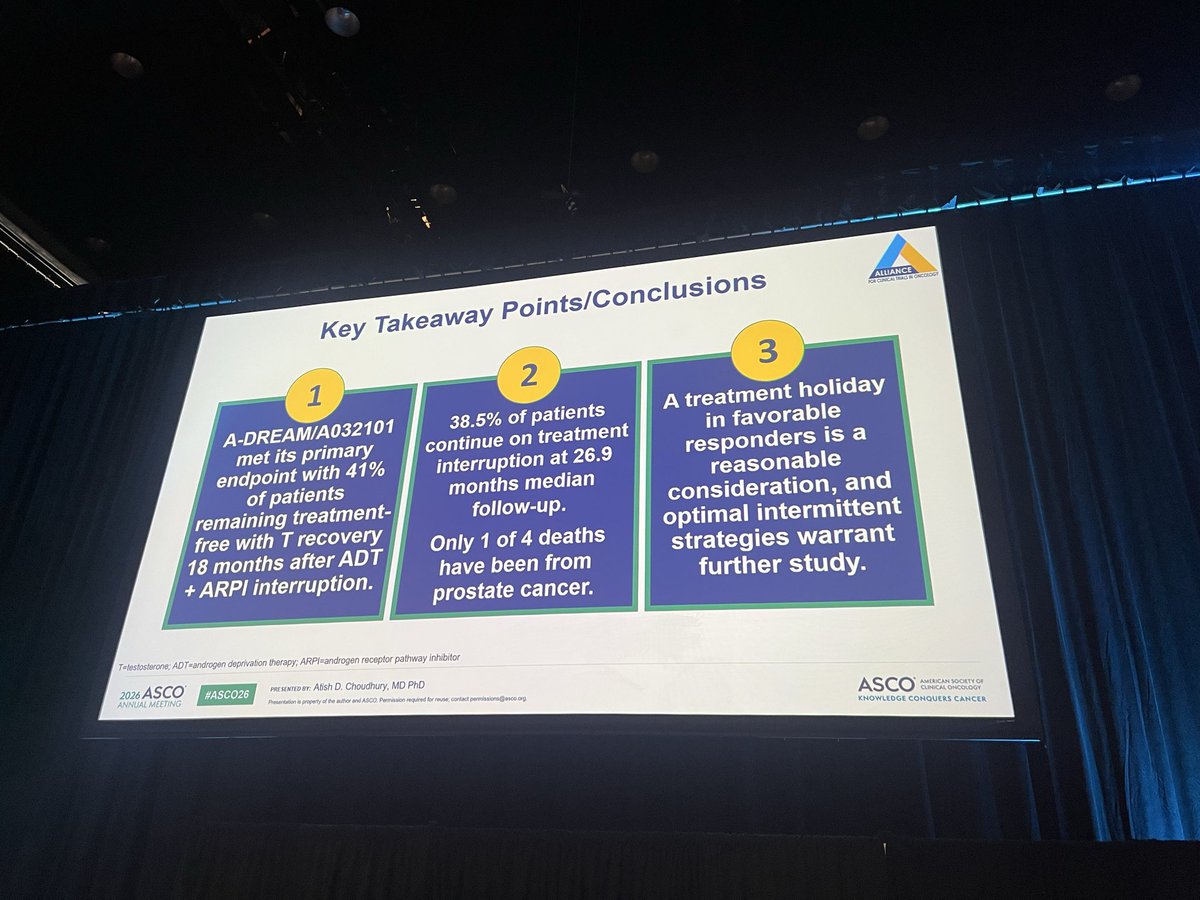
@DanaFarber and @DanaFarber_GU 's very own @AtishChoudhury presents compelling de-intensification data from A-DREAM/A032101 in mHSPC: 41% of favorable responders remained treatment-free with testosterone recovery 18 months after ADT + ARPI interruption, supporting treatment holidays as a promising strategy in selected pts.
#ASCO26 #ProstateCancer
@OncoAlert@ASCO@OncBrothers
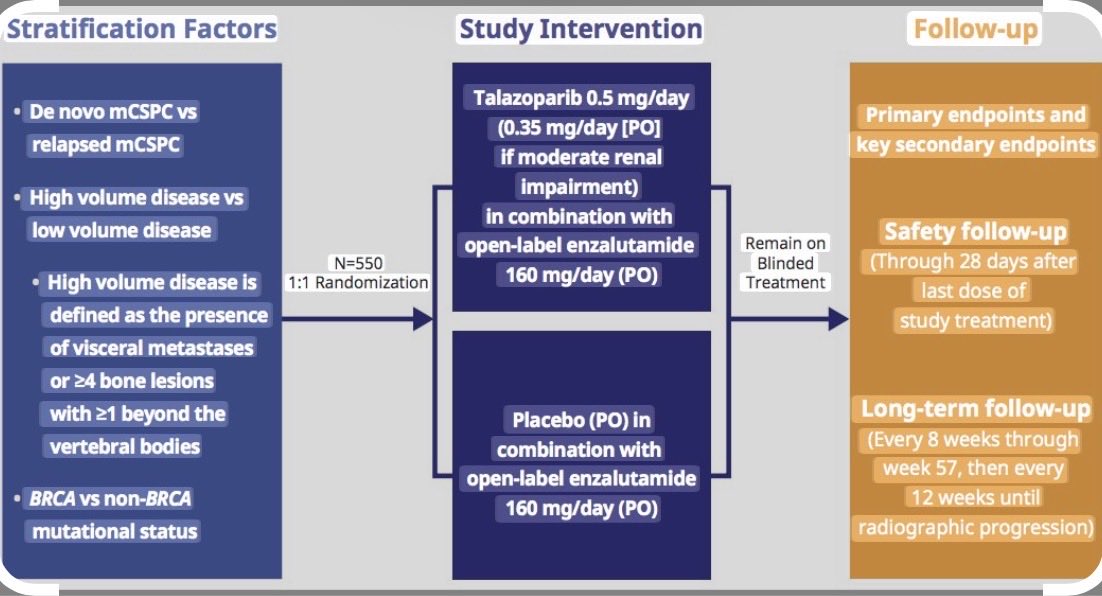
TALAPRO-3 #ASCO26 talazoparib + enzalutamide in HRR-altered mCSPC prostate looks the most impressive PARPi data to date. Efficacy in the non-BRCA HRR population is impressive IMO. Long term treatment is associated with long term side effects. @neerajaiims@OncoAlert
#ASCO26
1/2 ctDNA analysis (Signatera 16-plex and 64-plex) from KN564
Baseline ctDNA remained ⬇️(5.4% & 8.2%) yet ctDNA positivity consistently identified patients with worse DFS
ctDNA clearance was ⬆️with pembro & ctDNA dynamics correlated with DFS
@OncoAlert@DrChoueiri
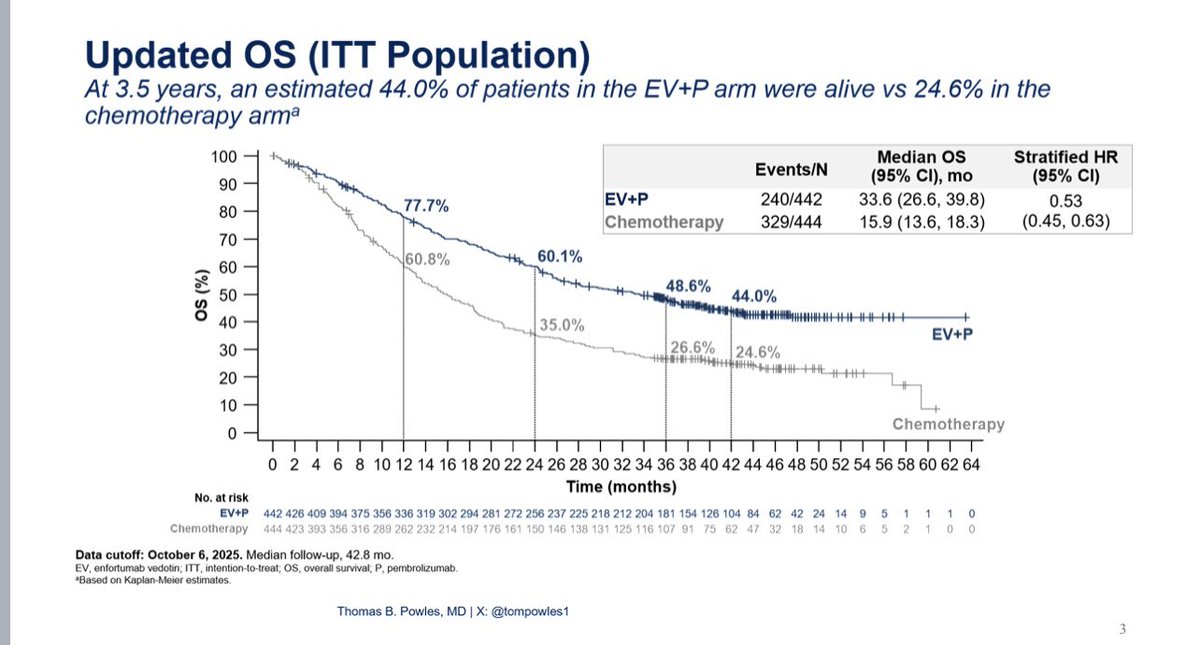
The 3.5yr OS from EV302 continues to show transformative benefit (HR 0.53 (0.45-0.63)) #ASCO26 for EV/pembro. The landmark OS for the CR population (30%) is ~90%. Median time to CR is 4.5 months (responses mature over time). Response rates of platinum chemo after EVP is 21% (OS 11 months). This should be considered a 2nd line standard. Median duration of EV was 7 months - longer in responders. Optimal duration of EV trials are needed. @OncoAlert
The OncoAlert🚨 GU faculty’s TOP 10 abstracts In GU Oncology for #ASCO26 are here — selected by our leads and finalized through a Delphi voting process with our senior GU cancer experts across #ProstateCancer#KidneyCancer#BladderCancer .
A snapshot of what will shape GU oncology at #ASCO26 👇
1️⃣ LBA5007 — TALAPRO-3
Talazoparib + enzalutamide vs placebo + enzalutamide in mCSPC with HRR alterations
2️⃣ LBA1 — PROTEUS
Perioperative apalutamide + ADT vs ADT in high-risk localized/locally advanced prostate cancer (final Phase 3)
3️⃣ 5001 — ENZAMET genomic analysis
Decipher >0.85 to identify benefit from adding docetaxel to ADT + enzalutamide
4️⃣ LBA4511 — KEYNOTE-564 ctDNA
ctDNA dynamics in RCC treated with adjuvant pembrolizumab vs placebo
5️⃣ 4502 — RAMPART
Durvalumab vs active monitoring after resection in RCC (Phase 3 RCT)
6️⃣ 4500 — RADICAL (A031801)
Radium-223 + cabozantinib in RCC with bone metastases
7️⃣ 4507 — EV-302 long-term follow-up
Enfortumab vedotin + pembrolizumab vs chemotherapy in 1L LA/mUC
8️⃣ 4513 — AMBASSADOR (A031501)
HRQoL with adjuvant pembrolizumab vs observation in high-risk MIBC
9️⃣ 4503 — SAKK 06/19
Perioperative intravesical rBCG + chemo-IO strategy in MIBC (primary analysis)
🔟 4510 — KEYNOTE-905
HRQoL with perioperative enfortumab vedotin + pembrolizumab in cisplatin-ineligible MIBC
Leads
@nataliagandur@scocmem@AmandaNizamMD@WeOncologists
Senior Faculty
@montypal@DrDanielHeng@apolo_andrea@DrChoueiri@PGrivasMDPhD@TiansterZhang@neerajaiims@amerseburger@Silke_Gillessen@tompowles1@AndreaNecchi@cdanicas@AOmlin
Pinging
@crisbergerot@HHammersMD@ravikanesvaran@sonpavde@drenriquegrande@scserendipity1@EfstathiouEleni@BraunMDPhD@brian_rini
🔥 POISE-3 Urology published in European Urology 🚨
In the largest randomized placebo-controlled #urology analysis of #TranexamicAcid (TXA), #TXA reduced major #bleeding risk by 37% (from 9.5% to 6.1%) with no clear increase in #thrombosis
More at https://t.co/Yypy7vb9Jz
#EBM
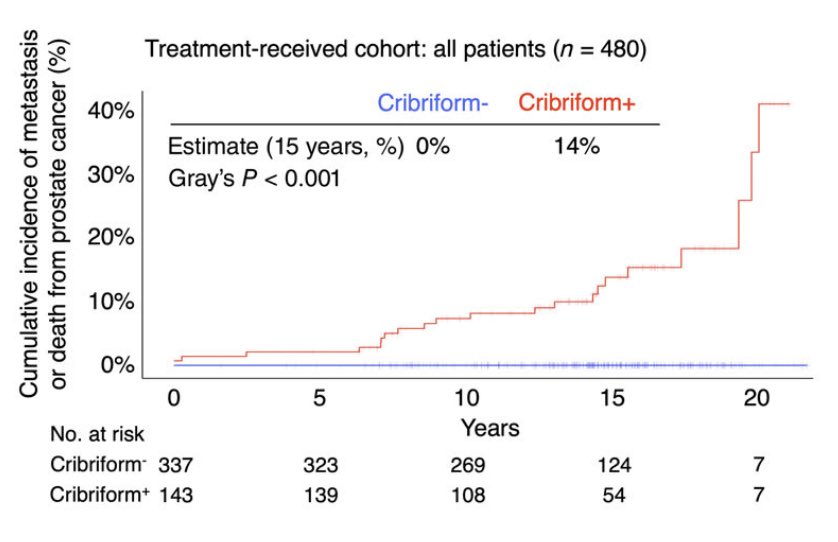
9️⃣ years later, the story of dual immune checkpoint blockade in metastatic RCC is still being written.
The final "very" long-term follow-up of CheckMate-214 confirms what many hoped in 2018: durable survival, deep responses, and a subset of patients who may experience long-term disease control with nivolumab + ipilimumab.
A short 🧵 on what 9+ years of follow-up teach us about immunotherapy in kidney cancer since Bernard Escudier @myESMO 2018 plenary presentation
https://t.co/l77lPkeLrl
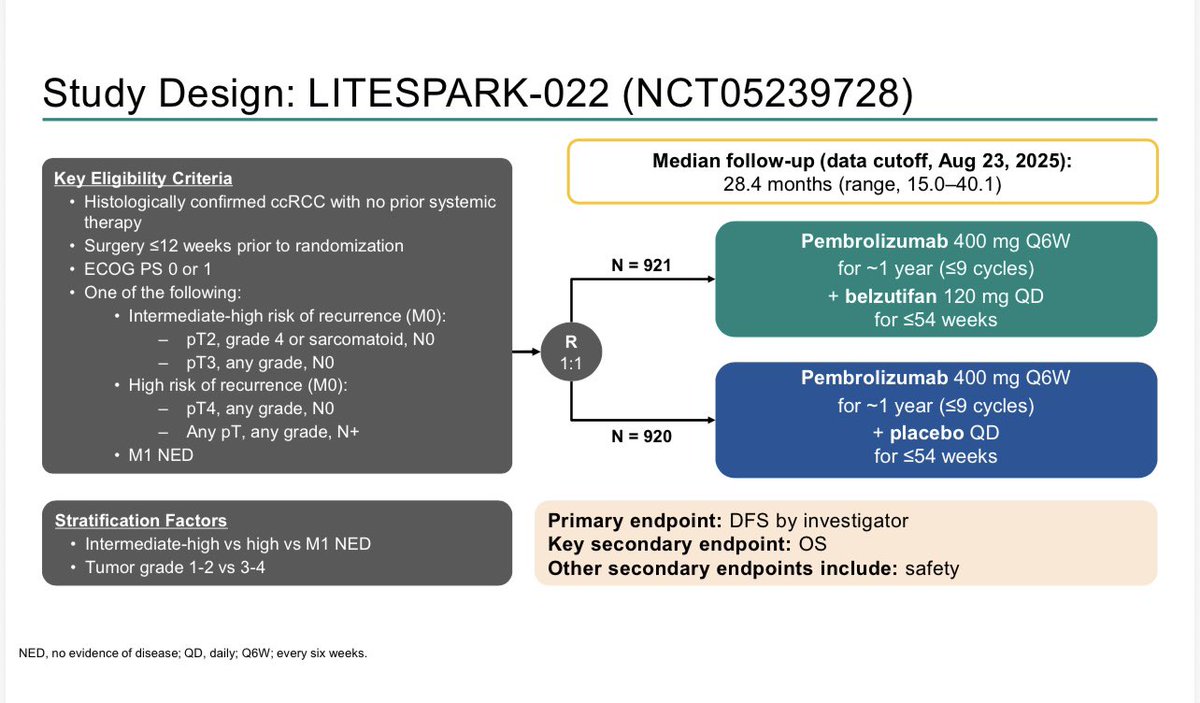
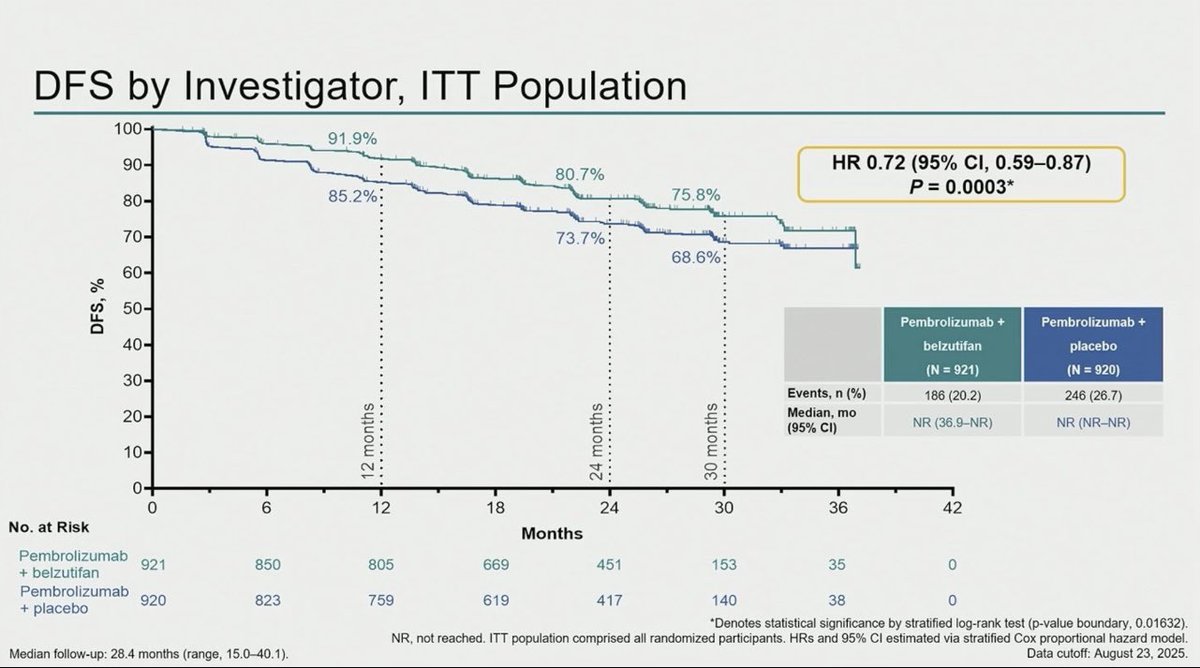
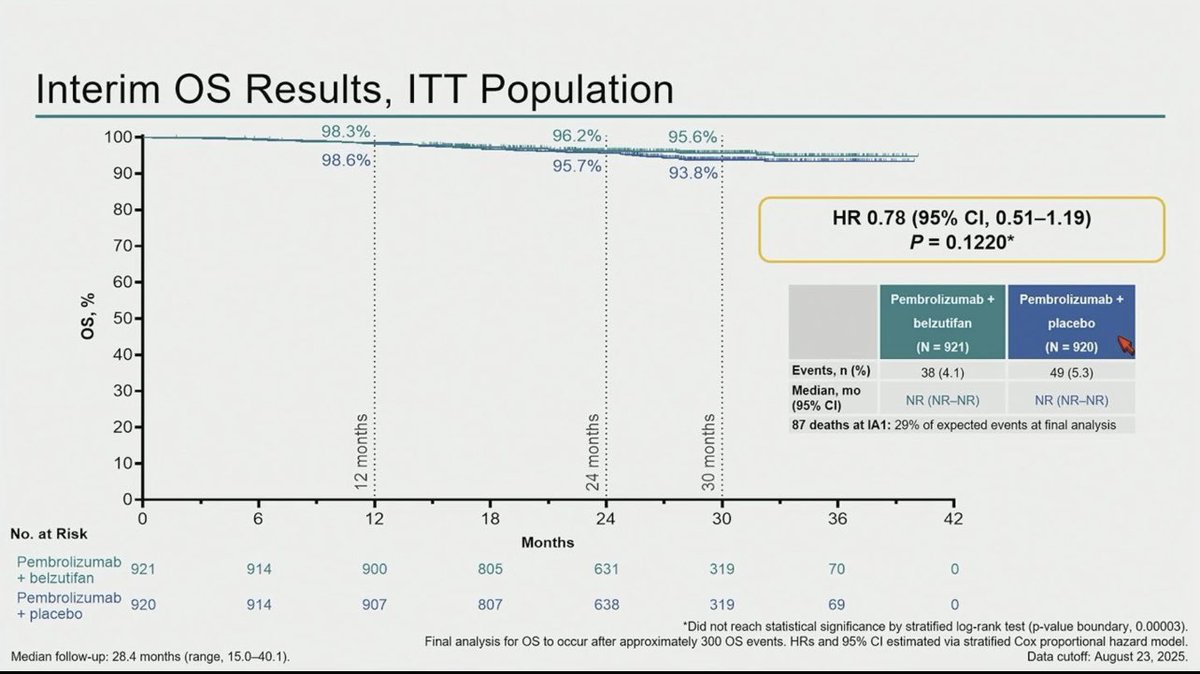
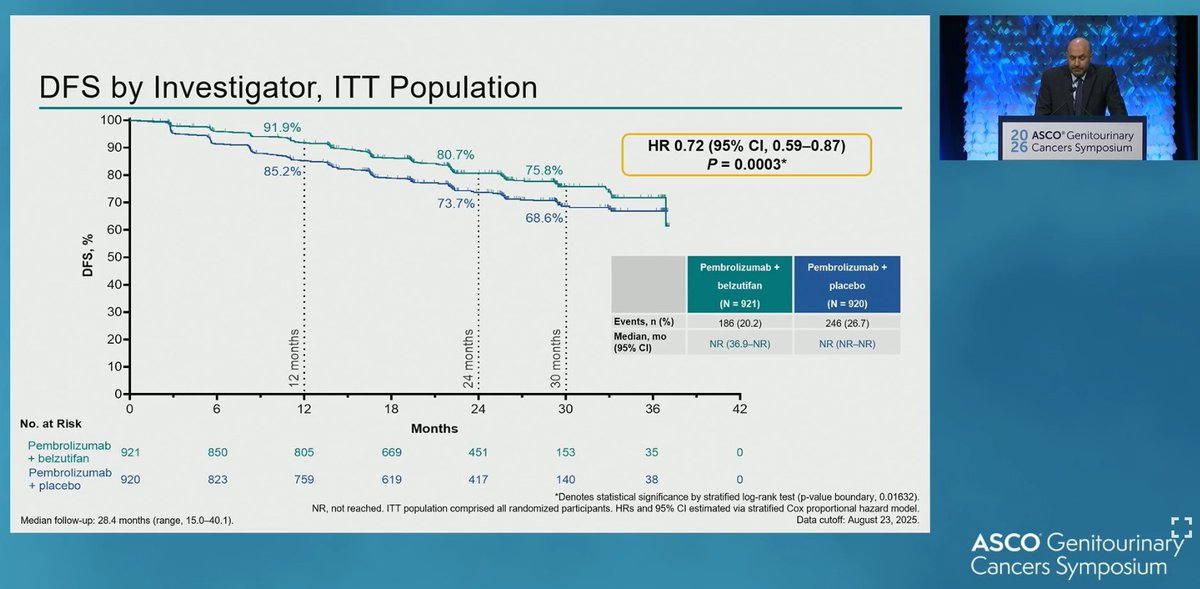
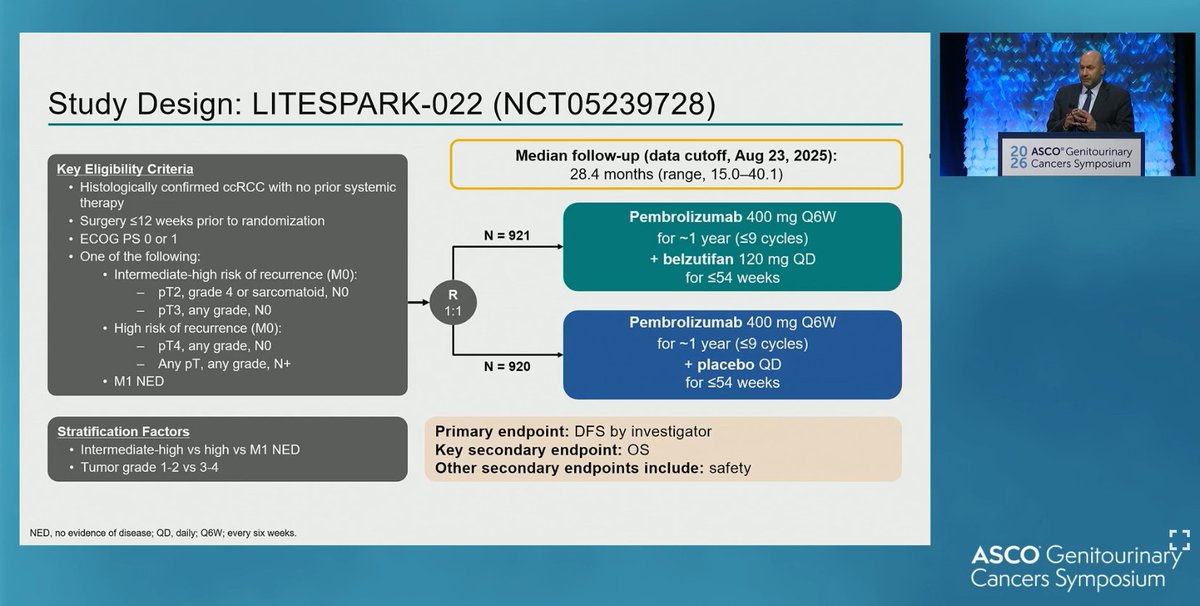
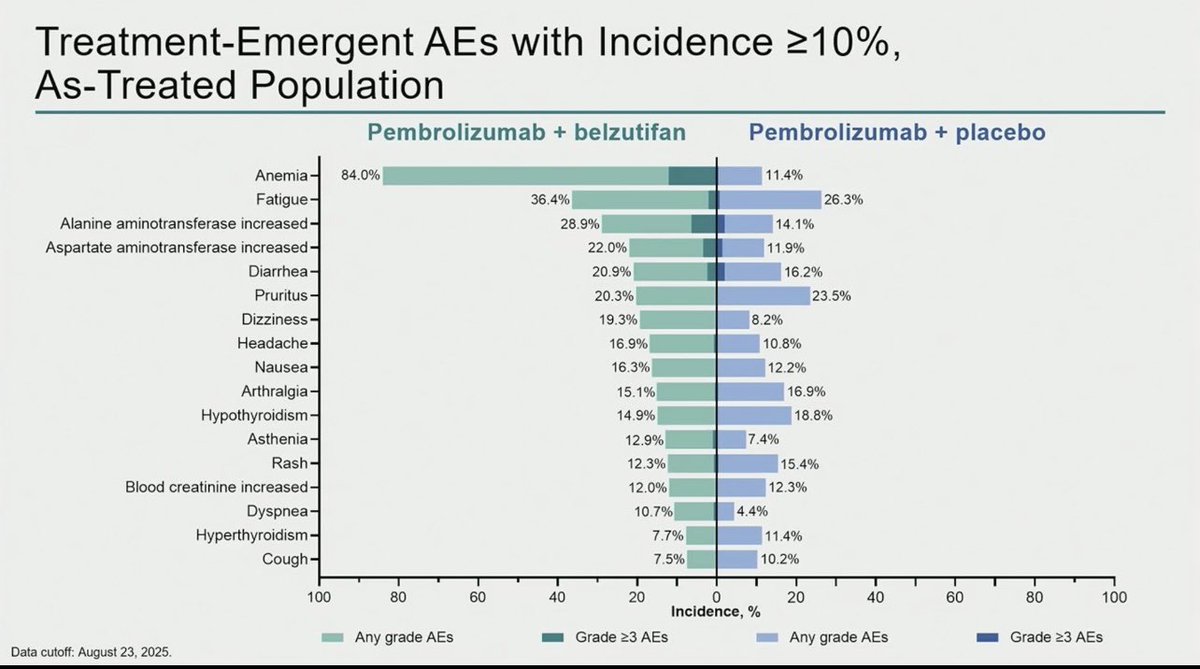
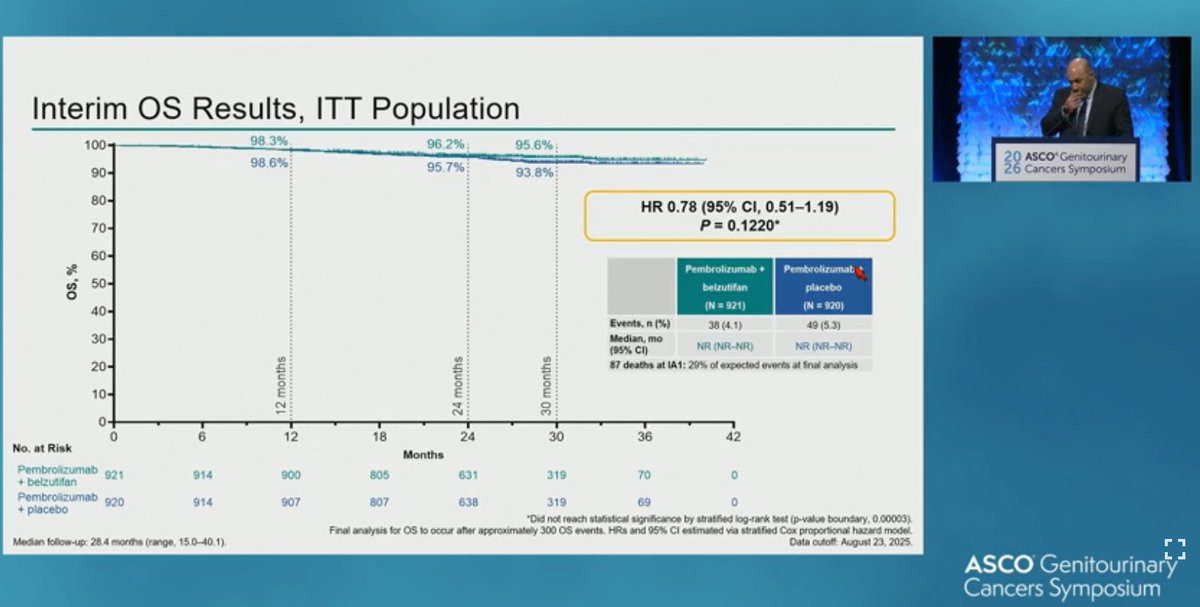
R3 LITESPARK-022: Adjuvant Pembrolizumab + Belzutifan vs Pembrolizumab for Clear Cell Renal Cell Carcinoma #GU26 showed significantly delayed DFS HR 0.72 (95% CI, 0.59–0.87) active across all subgroups. Immature OS (30 mnth OS 93% CDs 96%). ⬆️ Anaemia fatigue and transaminitis but only 4% discontinuation rate for belzutifan. The shape of the DFS curve and early OS trending the right way looks like initial analysis of KN564 and we know where that ended, making pem/bel attractive. @OncoAlert@DrChoueiri
🆕adjuvant combo for #RCC : LITESPARK-022 #GU26
DFS: HR: 0.72‼️
OS: inmature data..... but comparator arm was THE most effective active treatment available.
@DrChoueiri@tompowles1@BourlonMaite@ASCO
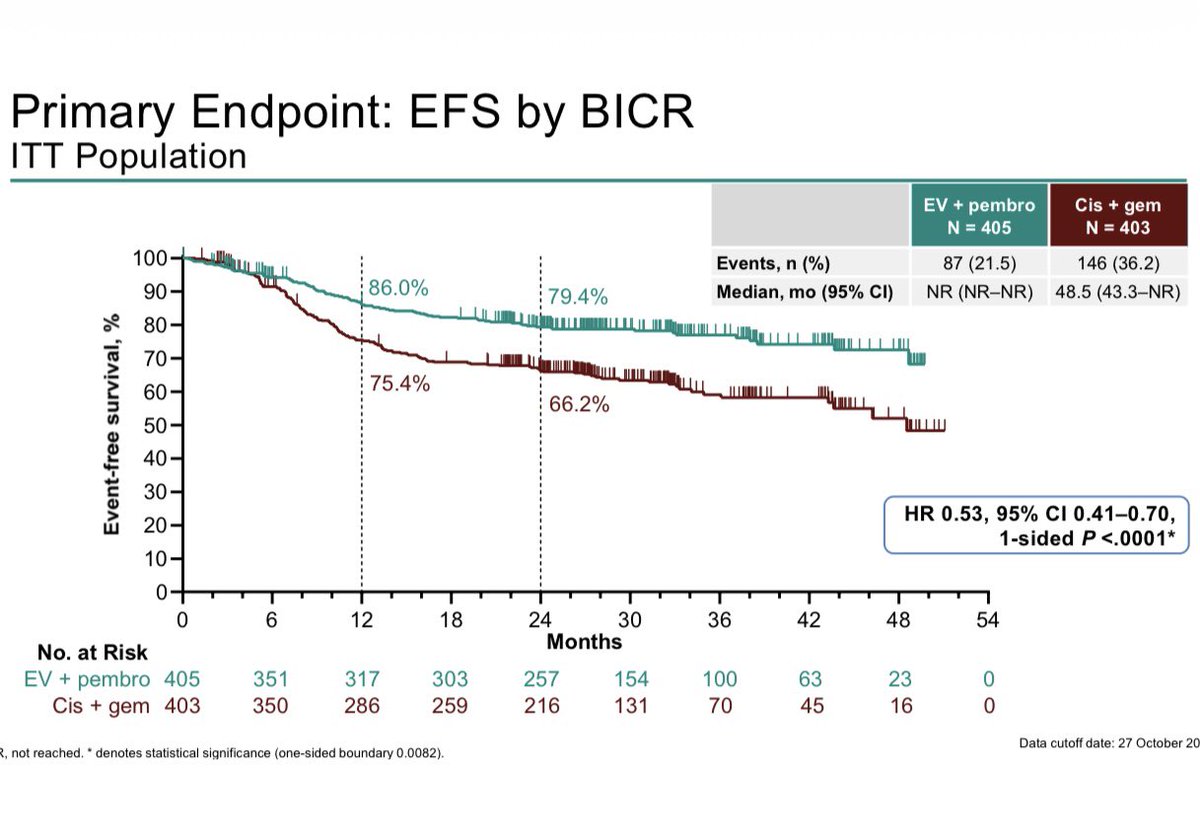
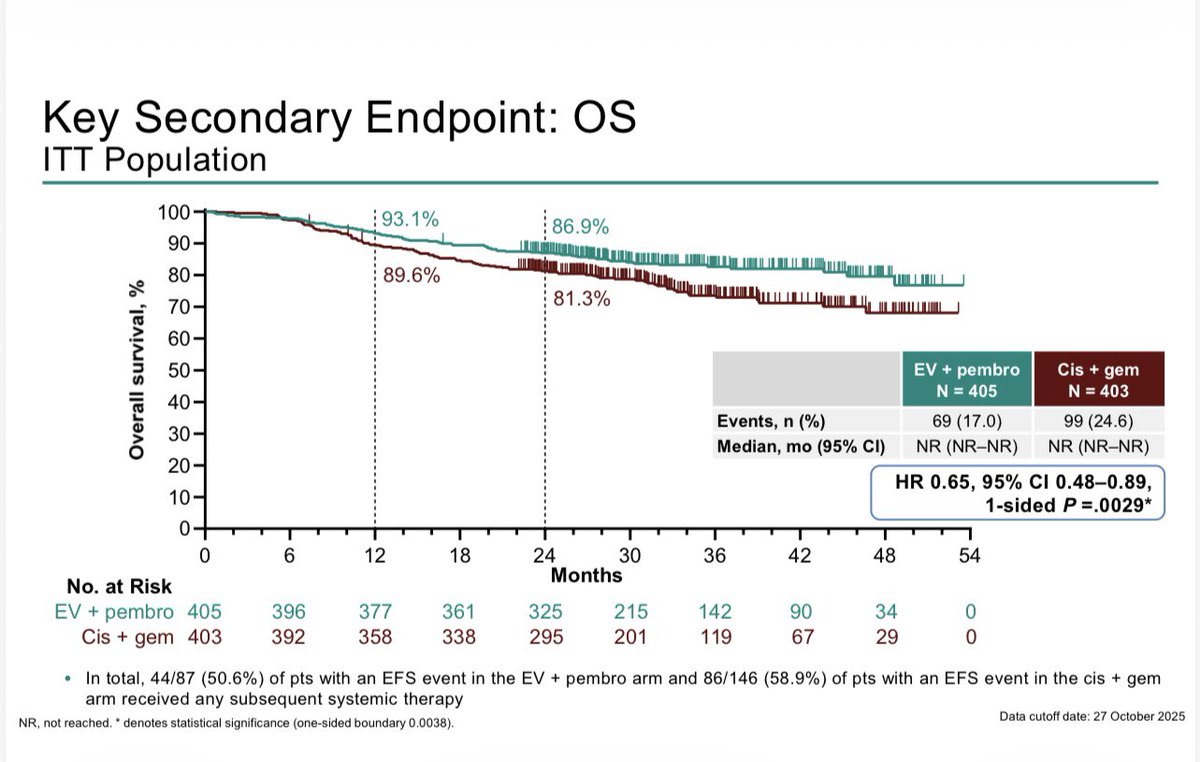
KN-B15/EV303: R3 Perioperative EVP vs Gem/cis in MIBC shows EFS HR 0.53 (0.41–0.70), OS HR 0.65 (0.48-0.89), pCR 56% vs 33%, G3+ tox 76% vs 67% #GU26. About half the patients completed 9 cycles of EVP. These are great results. Gem/cid is harder to beat when not all patients are at risk of relapse. Bladder sparing approaches for cCR (~60%) will be where this ends. ‘EVP 1st, ask questions later’. These studies are needed soon.