bought an advance rental plan (399 monthly plan, +91-5223118002) on 15 june, 2025. in november billing cycle Rs 30.38 is shown as payable amount. Secondly 15 days extra on 6 months prepaid offer not showing in bill.
Installation is completed on 15.06.25, 06:40pm
( email
I accidentally discovered how to read a complete book in 30 minutes.
A Harvard student showed me the workflow. Here's exactly what he does.
He doesn't open a book and start reading from page one.
He said that's the slowest, most inefficient way to absorb a book ever invented. You read linearly, your brain has no context for what matters, and by chapter four you've already forgotten chapter one.
He does something different.
He uploads the entire book into NotebookLM first.
Then he runs one prompt before touching a single page.
"What is the single central argument this book is making? What does the author believe that most people don't? And what are the 5 most important ideas I need to understand before everything else makes sense?"
That prompt does something most people don't realize. It gives your brain a skeleton before the flesh goes on. You are no longer reading to discover what the book is about. You already know. Now every page you read is confirming, extending, or challenging something you already hold in your head.
That is a completely different cognitive experience.
The second prompt is the one that saves the most time.
"Which chapters or sections contain the core ideas? Which ones are examples, case studies, or repetition of things already said?"
Most nonfiction books are 60 to 70 percent padding. Not because the authors are dishonest. Because publishers want 250 pages, not 80. The actual argument usually lives in four or five chapters. The rest is illustration.
NotebookLM tells him exactly which four chapters to read. He reads those. He skips the rest.
He is not missing anything. He is cutting everything that was never the point.
The third prompt is what separates this from summarizing.
After reading the core chapters, he goes back and asks: "What questions does this book not answer? What would a hostile critic say is wrong with the central argument? Where does the evidence feel weakest?"
This is the move that most people never make. They read. They absorb. They move on. They have opinions given to them by the author and they carry those opinions around as if they built them themselves.
He stress-tests the book before he closes it. He knows where it holds and where it doesn't. That is not reading. That is thinking with the book as a sparring partner.
The final prompt is the one I use every time now.
"If I had to explain this book's core idea to a smart 14-year-old in three sentences, what would I say? And what is the single most actionable thing the author wants the reader to do differently after finishing?"
That prompt forces compression. And compression forces understanding. You cannot compress what you do not actually understand.
I read four books last month this way.
I retained more from each one than I have from any book I read cover to cover in the last two years.
The average person reads a 300-page book in six hours and forgets most of it within a week. He reads the same book in 30 minutes and can still argue its central thesis six months later.
The book didn't change. The interface did.
Most people are reading books the way they were designed to be sold.
He reads them the way they were designed to be understood.
Dear friends, as promised, the citizens funded generics vs. branded drugs project is now published after 4 months in peer review. It was hardwork, but worth the effort because all of you helped us realize this important work.
You can read the full detaild paper here: https://t.co/jZhm8ZcPCq
Here is a simplified summary:
Do cheaper generic medicines work as well as expensive branded ones? It's a question that worries patients and even many doctors, who often quietly assume that a low price must mean lower quality. This doubt has real consequences in India, where medicines make up nearly two-thirds of what families spend out of their own pockets on healthcare — a burden that pushes millions into poverty and forces people to split doses or stop treatment altogether.
To put the question to a fair, independent test, our team at the Mission for Ethics and Science in Healthcare (MESH) carried out a fully citizen-funded study, paid for entirely by donations from ordinary members of the public, with no money or influence from any drug company.
We bought 131 samples of 22 commonly used medicines — covering heart disease, diabetes, infections, pain, acidity, and more — from seven different kinds of outlets across Kerala, including government stores like Jan Aushadhi, private generic chains, and premium branded pharmacies. Every sample was then coded, blinded, and sent to a top accredited laboratory for rigorous testing against the Indian Pharmacopoeia 2022 standards. What makes this study unusual is that very few before it have tested branded and generic versions from the same market side by side, included government-supplied medicines, and combined strict quality testing with a hard look at price — all at the same time.
The result was striking in its simplicity: every single one of the 131 medicines passed every quality test. 100%. It made no difference whether a pill was generic or branded, cheap or expensive — they were all equally good in their active ingredient content, their purity, and how they dissolve in the body.
Yet the prices told a completely different story. Generic medicines were, on average, 48.6% cheaper than their branded twins, and the most expensive brand cost up to 13.9 times more than the cheapest generic of the very same drug. Government Jan Aushadhi stores were the cheapest source for 18 of the 22 medicines tested, with potential savings running into thousands of rupees a year per medicine — for instance, over ₹16,000 a year on a single liver drug.
For doctors, this is reassuring, hard evidence that prescribing a quality-assured generic is not a compromise on care; it is the same medicine at a fraction of the cost. For patients, it means you can stay on your treatment without it draining your savings, which is exactly what keeps people healthier over the long run.
And this is precisely why independent, publicly funded projects like this matter so much for the future of healthcare in India: they answer the questions ordinary people actually have, free from commercial pressure, and they build the trust that programmes like Jan Aushadhi need to truly succeed. Affordable and high-quality are not opposites — in a well-regulated market, they go hand in hand.
More here: https://t.co/jZhm8ZcPCq
If someone you love is stuck in anxiety, send them this.
Follow @Lorwen108 for more insights on the journey to authenticity.
Repost if this helped you. 🙏
Recap — 8 daily fixes for 3 AM wake-ups:
1. No food 3h before bed
2. 9 PM open-loop dump
3. Map vs territory check
4. Name the primal loop
5. 4-8 breathing before bed
6. 'What does my body feel?' at 3 AM
7. Stop willpower-ing back to sleep
8. One true thing before sleep
Thyroid cancer used to affect people aged 60. Now it's the most common cancer in young adults between 16 and 33 years old. According to the National Cancer Institute, diagnoses have tripled since the 1990s.
Here are 8 things that damage your thyroid without you realizing it:
1. Tap water
@DrDhruvchauhan@advsatyamrajput Good initiative, Dr dhruv, incompetent auditories
NTA> Paperleak
MCC> Delayed counselling,
national board (NBE) Always delaying examination courses they affiliated
NMC> Irregularities in affiliation of pvt. Medical colleges, no grading/ ranking system of Medical institute
One of my clients was 26 kg overweight, struggling with a big belly and low confidence. He set a clear goal—to reach 12% body fat in 2026.
Here are the 25 rules that helped him completely transform his body and life:
Rule 1. STOP RUNNING.
Agree with you Anoop. Very important to flag issues which are relevant to Indians. Few people are aware that HbA1c increases with age. A 70 year old with HbA1c of 6.1 with normal fasting and 2 hour glucose values on OGTT is dubbed as Prediabetes and started on Metformin. Lab standardisation of A1c is also a huge issue. Also those with isolated A1c increases often do not have other cardio metabolic risk factors. Congratulations on continuously bringing these issues to the attention of public 👏👏
Schizophrenia: Beyond Dopamine D2 Blockade
1. Dopamine is necessary—but not sufficient.
For nearly 70 years, all approved antipsychotics have relied on D2 receptor antagonism. While this effectively reduces positive symptoms (hallucinations, delusions), it offers minimal benefit for negative symptoms and cognition, which drive long-term disability.
2. Unmet needs define modern schizophrenia care.
Persistent social withdrawal, anhedonia, impaired executive function, and high cardiometabolic mortality remain largely unaddressed by conventional antipsychotics.
3. Schizophrenia is biologically heterogeneous.
Genetic and neurobiological data confirm multiple pathophysiological pathways, making a “one-drug-fits-all” model biologically implausible. Precision-based, multi-target therapy is the future.
BREAKTHROUGH: NON-DOPAMINERGIC ANTIPSYCHOSIS
4. Muscarinic receptor modulation is the first true paradigm shift.
The approval of xanomeline + trospium (M1/M4 muscarinic receptor agonist combination) marks the first effective antipsychotic not based on D2 blockade.
• Improves psychosis without dopamine antagonism
• Potential advantages for cognition and negative symptoms
• Reduced risk of extrapyramidal and hyperprolactinemic adverse effects
Clinical Insight: Antipsychotic efficacy is achievable without direct dopamine blockade, validating cholinergic modulation as a therapeutic axis.
EMERGING TARGETS: MULTI-DOMAIN STRATEGY
5. Glutamatergic modulation (NMDA-related pathways).
Agents targeting glycine sites, metabotropic glutamate receptors, and NMDA receptor hypofunction show promise for cognitive and negative symptoms, though clinical results remain variable.
6. GABAergic and serotonergic pathways.
Selective 5-HT receptor modulators and GABA-interneuronal enhancers may refine symptom control and reduce affective and cognitive burden.
7. Neuroinflammation and immune mechanisms matter.
Evidence increasingly links schizophrenia to microglial activation, cytokine dysregulation, and immune signaling. Anti-inflammatory and immune-modulating strategies have shown domain-specific benefits in selected patients.
SAFETY & MORTALITY: A CRITICAL CONSIDERATION
8. Cardiometabolic risk is not a side issue—it is a leading cause of death.
Current antipsychotics exacerbate obesity, dyslipidemia, insulin resistance, and cardiovascular disease, contributing to markedly reduced life expectancy in schizophrenia.
Clinical Pearl: Future therapies must demonstrate not only symptom control but metabolic neutrality or benefit.
TRIAL FAILURES ≠ TARGET FAILURE
9. Negative trials reflect complexity, not futility.
Several agents with novel mechanisms have failed in broad populations but later demonstrated benefits in specific symptom domains or patient subgroups, supporting a stratified treatment model.
PRACTICE IMPLICATIONS
10. Schizophrenia management is entering a multi-mechanism era.
• Dopamine antagonists will remain foundational for acute psychosis
• Muscarinic agonists introduce a new non-dopaminergic class
• Future regimens may combine dopaminergic, cholinergic, glutamatergic, and immunomodulatory approaches
• Symptom-domain targeting (positive vs negative vs cognitive) will define rational prescribing
TAKE-HOME MESSAGE
Schizophrenia is not a single-pathway disorder.
The approval of xanomeline/trospium confirms that effective antipsychosis is possible without D2 blockade, opening the door to mechanism-based, symptom-domain-specific, and metabolically safer treatments. The next generation of schizophrenia therapy will be biologically informed, multi-targeted, and personalized.
https://t.co/pjn75OqGx6
💬 Viewpoint: Recent evidence shows that routine contralateral tonsillectomy in p16-positive tonsillar OPSCC offers minimal oncologic benefit and increases morbidity, suggesting practice change may be warranted. https://t.co/G4CK6fQGN5
मुकेश अंबानी का लूट का किस्सा....
मैं शहर में रहता हूँ, और महीने में 4–5 दिन अपने गाँव जाता हूँ।
नेटवर्क की भारी समस्या के कारण मैंने मजबूरी में गाँव में Jio AirFiber लगवाया।
प्रति माह ₹706 का रिचार्ज करता हूँ।
चार दिन पहले गाँव गया और ₹1178 Jio को पेमेंट किए।
लेकिन इंटरनेट...?
स्क्रीन पर सिर्फ़ एक लाइन - “No Internet”
शिकायत करी तो जवाब आया👇
“टावर में समस्या है, इसलिए इंटरनेट उपलब्ध नहीं कराया जा सकता।”
ठीक है, मान लिया टावर में समस्या है।
लेकिन जो ₹1178 मैंने दिए, उनका क्या...?
ना इंटरनेट,
ना रिफंड,
बस कंपनी का सीधा-सा जवाब - हम कुछ नहीं कर सकते।
यही है कॉरपोरेट लूट का नया मॉडल
पहले भरोसा बेचो,
फिर मजबूरी में पैसा लो,
और आख़िर में जिम्मेदारी से पल्ला झाड़ लो।
अंबानी ऐसे ही अमीर नहीं बने,
ऐसे ही करोड़ों लोगों को चूना लगाकर बने हैं।
अगर आपको भी Jio का नेटवर्क, इंटरनेट या सर्विस बेकार लगती है, तो ज्यादा से ज्यादा शेयर करें।✊🔥
@reliancejio@JioCare
#अम्बानी_चोर_है
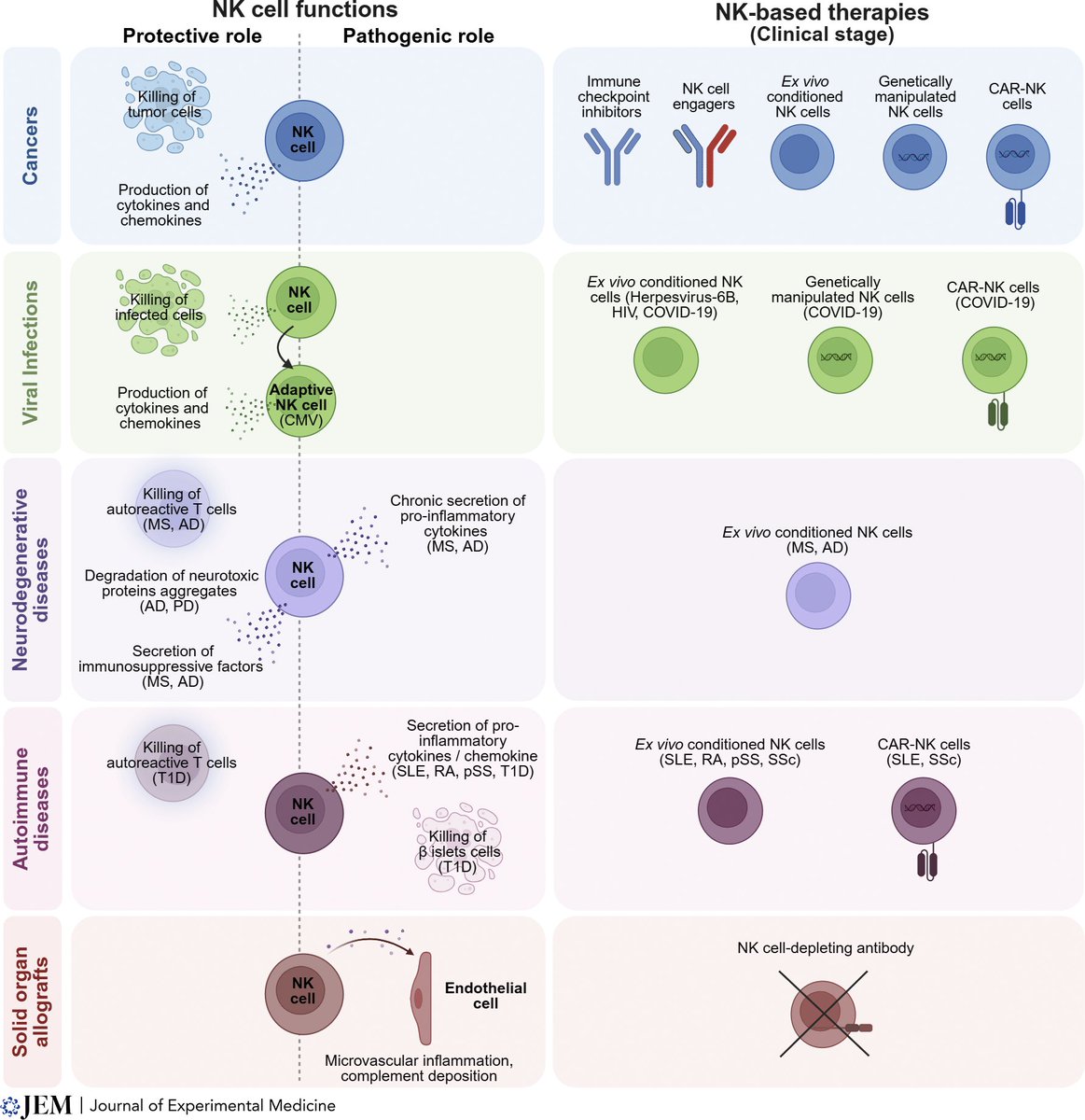
Natural killer (NK) cells are primarily being assessed to treat cancer, but they have substantial potential for Rx of neurodegenerative diseases, viral infections, and autoimmune conditions. A first-rate review @JExpMed
https://t.co/1bEMrzeNsP
COVID-19 can cause lasting frontal lobe damage, leading to brain fog, emotional dysregulation, and cognitive deficits.
Mechanisms include inflammation, strokes, and hypoxia; recovery is partial, with risks of long-term neurodegeneration.
https://t.co/WySX8m9KMR
@RWMaloneMD To treat the SPIKE protein /detox, I've heard about 3 solutions. 1) Follow Dr Peter McCullough regimen (first video below) 2) Also a new treatment called "Hemopurifier" that is a novel approach. 3) Lastly, the "EBO203 blood oil change" treatments (second video below). #covıd