-short report turnaround time and closed-loop communication is necessary for relevance in hyperacute management of stroke
-delayed adoption of new technology that facilitates an emerging standard of care may create medicolegal exposure
@ShadiYaghi2 But it may not all be about neglect. Sounds like he was pretty certain about onset time and I would’ve thought benefit of doubt ought to have gone with the patient, especially with a plumb normal NCCT
In a systematic review and study-level meta-analysis, TNK improved excellent functional outcomes and recanalization in AIS patients treated within 4.5-24 hours, without increasing the risks of sICH or mortality. #stroke https://t.co/6m34Pm2pyJ
@PracticalNeuro@JAMANeuro@EVToday@American_Stroke@AANmember Good to bear in mind though that study participants were a mixed bag with: carotid or intracranial artery stenosis, noncardioembolic stroke, ischemic heart disease, or peripheral artery disease.
Congratulations @ShadiYaghi2 on the new classification system. Specifying the minimum diagnostic work up is an important advance, and one that’ll have important resource implications for Stroke services @BIASPstroke@HargrovesDavid
The stroke field had major developments since 1993 when the TOAST criteria were proposed. We need move on to a different system that incorporates new mechanisms/tools/testing and standardizes the minimum workup. Introducing ISPS25 #stroke#WSC25#meded https://t.co/Tv3xYXBznX
TNK improves excellent outcomes & recanalization in pts w/ acute stroke treated w/i 4.5-24h, w/o increasing symptomatic ICH or mortality, and provides greater additional benefits when EVT is inaccessible.🧠
https://t.co/ebaDGhZpzh
#SCCMNeuro#NeuroICU#NeuroTwitter#NeuroX
#STROKE: This special report by @AmolMehtaMD et al. critically appraises recent literature on endovascular thrombectomy for medium vessel occlusion stroke and offers consideration for practice. #AHAJournals https://t.co/BKDnRMukbo
Just when we thought TNK it is …
In patients with salvageable brain tissue identified by perfusion imaging who did not initially receive MT, alteplase given 4.5 to 24 hours after acute ischemic stroke onset improves outcomes https://t.co/bsy59hjgcZ
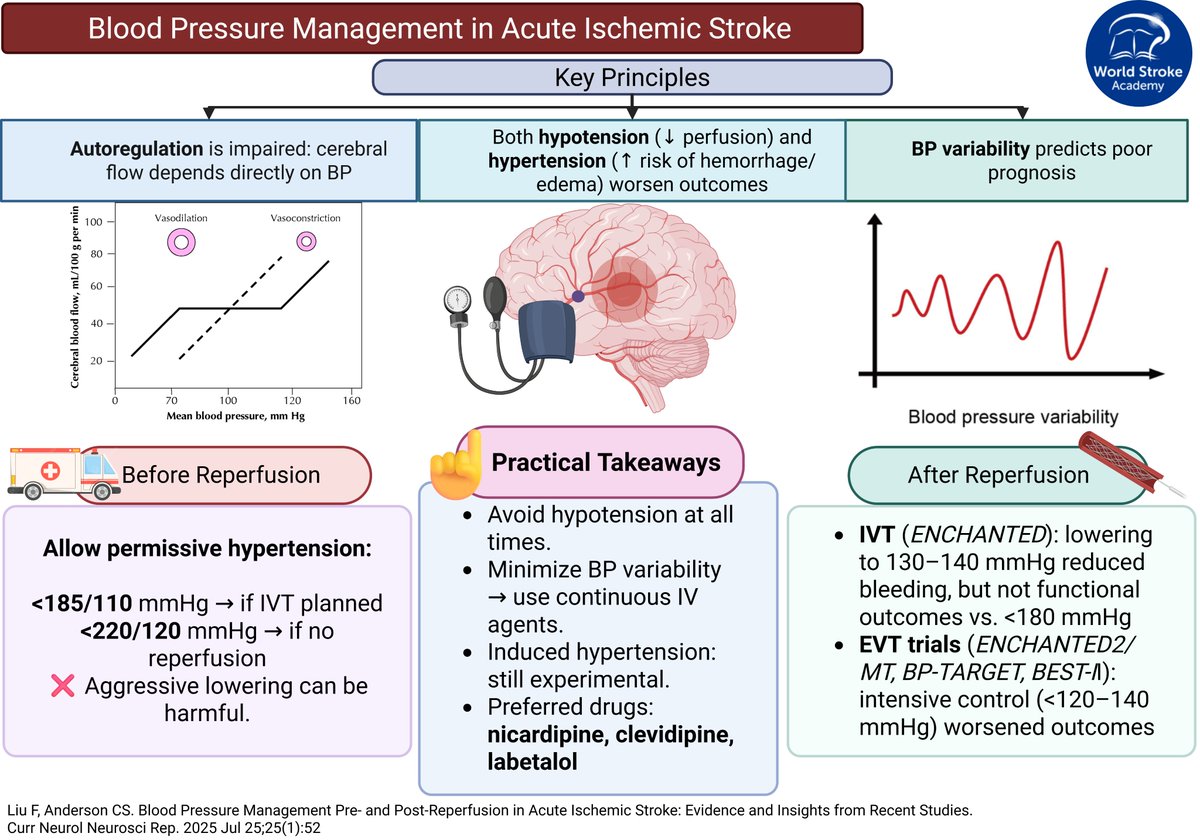
#MondayTip#BloodPressure management in Acute Ischemic Stroke
☝️Stability > aggressiveness
🚑Pre-reperfusion: #tolerate high BP (<185/110 if IVT, <220/120 if no reperfusion).
💉Post-reperfusion: #avoid intensive lowering, safer range is ~140–180 mmHg
🆓https://t.co/NxCWIWgiBQ
https://t.co/TmuWQKZQUr
Delighted the Thrombolysis in Acute Stroke Collaboration (TASC) tool kit is now available ☝️
18 hospitals with low IV lysis rates @NHSEngland demonstrated phenomenal agency, learning & improvement, averaging:
45% ⬆️rates & 20mins ⬇️DTN 👏
@NHSElect
The 2024 Lancet Commission stated that there are multiple preventable risk factors for #dementia. Addressing these factors may reduce future risk but there is a lack of interventional studies.
#MondayTip#DWI_negative AIS
📊Meta-analysis, 3,236pt➡️6.8% had clinical diagnosis of AIS w/DWI (-)
🔑Post. circulation is key: 5x greater odds of (-) DWI vs anterior strokes
⏰Timing & size matter
☝️While DWI is highly sensitive, it can still be falsely (-) in selected AIS cases
Great to see Radiology & Stroke clinicians come together to learn about CTP. We need this for #strokecare
Thanks to all speakers and a special shout out to @rayessastroke for coming down all the way from Hull! @HargrovesDavid
An underrated life lesson: Your energy creates your reality. Give your energy to stress, complaints, and negative people, they will grow. Give your energy to ambitions, gratitude, and positive people, they will grow. Your energy is your destiny. Choose wisely.