After decades of work….when it really feels like a service, contribution to health of children, and not just a professional survival…when you can see the smiles 🙂🙂🙂on faces of children from the marginalised and underserved communities.
The "First Flow" project is such an act of service for the adolescent girls in underserved pre-urban communities.
Register Now:- https://t.co/AAIhIiVp8G
Accreditation is often seen as the benchmark of quality, but the true challenge lies in sustaining excellence, ensuring patient safety, driving continuous improvement, and building a culture of quality across healthcare organizations. Join us for an engaging discussion with distinguished healthcare leaders as they share practical insights, real-world experiences, and strategies to strengthen healthcare quality in India. Date: 25th June 2026 Time: 4:00 PM – 5:00 PM IST Meet Our Speakers Dr Mahtab Singh, Director Operations & Management (NHI) A Public Health & Quality Improvement Leader Dr. Kedar Sawleshwarkar, Director, Neonatal & Pediatric Center of Excellence, Mahaveer Hospital, Chh Sambhaji Nagar, Maharashtra Moderator: Dr. Manisha Khurana, Editor-in-Chief, Voice of Healthcare | Founder, Next Edge Precision Medicine Insights
Register Now:- https://t.co/AAIhIiVp8G
NIWARA HealthCare Improvement #BeyondAccreditation #HealthcareQuality #PatientSafety
To follow & execute the Quality Improvement learnings of more than a decade, Dr Kedar Sawleshwarkar, NHI's Director Research & Documentation, has started this world class evidence based facility in an under developed area of the country.
Dr Mahtab Singh, Director Operation & Management participated as 'Guest of Honour'. The facility is going to save a lot of lives in the area to help achieve the set indicators for the area and the country.
NHI with its team congratulates him and extend the best wishes. @kedarpriya1@NNF_india@HelenBevan@PeterLachman@NHSRC_India@IHF_FIH
The teams that deliver the most in periods of rapid change are those that experiment the most & learn the fastest: Part 2.
A summary of comments in response to my last post from across multiple social platforms. I pulled out five themes:
1) Purpose and the why: Penny Triantafillou argued that building “superteams” is an investment, not an intervention. People can cope with uncertainty if they understand the why: purpose creates connection, energy and resilience. Jonathan Sunkersing extended this beyond formal leadership: if anyone were willing to be curious, learn from failure and think carefully about giving feedback, society as a whole benefits.
2) Structural barriers to experimentation: Anthony Lawton noted that most of the habits I described require “discretionary capacity”: time, space, curiosity. NHS structures frequently consume that capacity before teams can use it. Assurance frameworks reward programme logic and penalise the iterative mess real improvement demands. Ish Ahmed, a surgeon, added that frontline experimentation often gets lost under governance layers, and meaningful innovation starts with small practical tests close to the work, not large centrally designed programmes. Richard Perry asked whether we need experimentation and learning rather than another competency framework.
3) Psychological safety as a prerequisite: Jamie Lackie observed that "what are you stuck on?" only works if the culture has made it safe to answer truthfully, and that teams have learned surfacing problems gets managed, not solved. Vik Chand stressed that teams learn faster when experiments feel safe, not career limiting. Binod Shankar added that many organisations do not have an innovation problem — they have a fear problem. They say they want experimentation while “punishing” mistakes, so people stop trying.
4) Curiosity is how knowledge is accessed: Cheryl Hoare highlighted the line: "In change work, the formal leader rarely holds the crucial knowledge. Curiosity is how we access it." Josh Sarkar noted that performance problems are frequently coordination problems, and the biggest gains come from redesigning how people work together. Bill Powell added that teams which adapt through change treat setbacks as data to interpret; those that simply endure it treat them as failure to hide
5) Collective learning means sharing failure AND success: Arokia Antonysamy argued that the highest-performing teams create environments where learning, experimentation, feedback and shared ownership are part of the culture. The NHS could leverage this at scale if teams shared what failed as well as what worked. Odiri Oteri noted how small and simple these changes are — catalysts that can transform an average team into a superteam with minimal effort. Maria Mentzer observed that innovation culture lives and dies with leader mindset and behaviour.
If I were to sum up the comments in a sentence, I��d say this: most teams have the potential to become "superteams" when we create the right conditions; e.g., a sense of purpose, curiosity, safety and time and space for shared learning.
Thanks to everyone who commented, These discussions are so rich and helpful.
La mesure de la qualité des soins dans les hôpitaux progresse mais reste lacunaire et pas suffisamment centrée sur les résultats effectifs, épingle la Cour des comptes. Malgré l'obligation légale, les accidents médicaux graves restent sous déclarés.
➡️ https://t.co/rW0O2roY3p
Ensuring accuracy, reliability, and excellence in laboratory practices is no longer optional—it’s essential.
Join this insightful webinar to explore how you can elevate lab safety standards and drive quality improvements that directly impact patient outcomes. Gain practical insights, expert perspectives, and actionable strategies to transform your lab from good to excellent.
Date: 6th May 2026
Time: 4:00 PM – 5:30 PM
Register for free here:
https://t.co/dnYicRpsUW
The Health outcome is directly proportionate to multiple of Utilization & Quality so if your quality is 0, the health outcome is also 0 automatically.
Meaningful access to healthcare services requires a commitment to quality to ensure that services are both reachable and effective. Providing access without ensuring quality is ineffective, wasteful, and unethical, as it fails to produce meaningful health outcomes.
Poor quality care causes 5 million deaths annually in low- and middle-income countries (LMICs), while 3.6 million deaths are due to insufficient access.
𝐍𝐮𝐫𝐬𝐞𝐬 𝐚𝐫𝐞 𝐜𝐞𝐧𝐭𝐫𝐚𝐥 𝐭𝐨 𝐭𝐡𝐞 𝐝𝐞𝐥𝐢𝐯𝐞𝐫𝐲 𝐨𝐟 𝐬𝐚𝐟𝐞 𝐚𝐧𝐝 𝐭𝐢𝐦𝐞𝐥𝐲 𝐜𝐚𝐫𝐞 𝐚𝐜𝐫𝐨𝐬𝐬 𝐚𝐥𝐥 𝐡𝐞𝐚𝐥𝐭𝐡 𝐬𝐲𝐬𝐭𝐞𝐦𝐬.
However, increasing pressure and limited support continue to affect their ability to respond effectively. Global workforce gaps further intensify this challenge, with a projected shortage of 𝟒.𝟓 𝐦𝐢𝐥𝐥𝐢𝐨𝐧 𝐧𝐮𝐫𝐬𝐞𝐬 𝐛𝐲 𝟐𝟎𝟑𝟎 (𝐖𝐨𝐫𝐥𝐝 𝐇𝐞𝐚𝐥𝐭𝐡 𝐎𝐫𝐠𝐚𝐧𝐢𝐳𝐚𝐭𝐢𝐨𝐧).
At the same time, sustained investment in the health workforce remains essential for strengthening health systems and ensuring reliable care delivery (Frontline Health Workers Coalition).
𝐹𝑟𝑜𝑚 𝑎 𝑝𝑎𝑡𝑖𝑒𝑛𝑡 𝑝𝑒𝑟𝑠𝑝𝑒𝑐𝑡𝑖𝑣𝑒, 𝑡ℎ𝑖𝑠 𝑖𝑠 𝑐𝑟𝑖𝑡𝑖𝑐𝑎𝑙.
When nurses are adequately supported, they are better positioned to deliver safe, consistent, and timely care. Evidence also shows that staffing pressures directly affect patient safety and quality of care (𝐈𝐧𝐭𝐞𝐫𝐧𝐚𝐭𝐢𝐨𝐧𝐚𝐥 𝐂𝐨𝐮𝐧𝐜𝐢𝐥 𝐨𝐟 𝐍𝐮𝐫𝐬𝐞𝐬).
Through its Heart of 𝐇𝐞𝐚𝐥𝐭𝐡𝐜𝐚𝐫𝐞: 𝐂𝐞𝐥𝐞𝐛𝐫𝐚𝐭𝐢𝐧𝐠 𝐎𝐮𝐫 𝐍𝐮𝐫𝐬𝐞𝐬 𝐜𝐚𝐦𝐩𝐚𝐢𝐠𝐧, the 𝐖𝐨𝐫𝐥𝐝 𝐏𝐚𝐭𝐢𝐞𝐧𝐭𝐬 𝐀𝐥𝐥𝐢𝐚𝐧𝐜𝐞 is advancing global awareness on the role of nurses in patient safety and calling for sustained investment in nursing workforce support.
Investing in nurses is not only a workforce priority. It is a patient safety imperative.
#HeartOfHealthcare #PatientSafety #SupportNurses #HealthSystems #NursingWorkforce
@WHOAFRO@WHO_Europe@UN@UNICEF@WorldBankGroup@OECD@SigmaNursing@ghc_global@IHF_FIH@ISQua@TheIHI@PLAN4ZERO@GlobalFund@NursingNow2020@HWAlliance2@PHealthupdate@HIMSS@ICNurses@HowardCatton@JHUNursing@NurseStandard@AAN_Nursing@YaleNursing@AmbCareNursing@DarlingtonUnion@ANANursingWorld@FHWCoalition
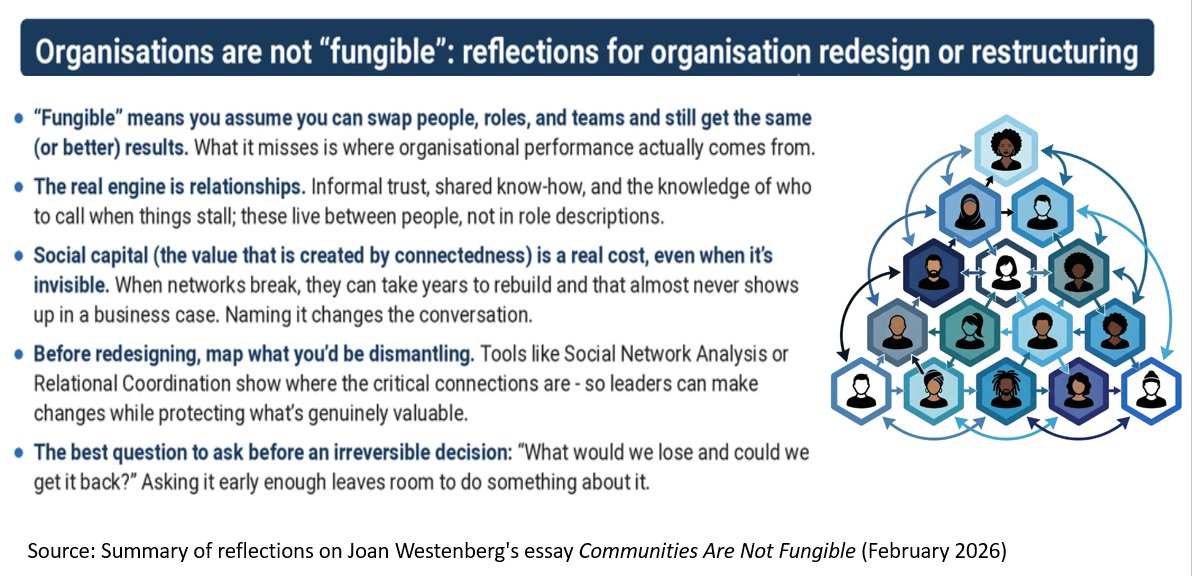
Organisations are not "fungible".
“Fungibility” is an assumption that if you redesign an organisation & replace one set of people with a different set, you will still get equivalent outputs. This mistaken belief underlies many organisational restructures: that you can redistribute roles, reporting lines & teams without meaningful loss.
I've been reading "Communities Are Not Fungible", a recent essay by @JoanWesten7568. She examines 1960s urban renewal, when planners believed demolishing old neighbourhoods & rehousing residents would allow communities to reform. They didn't. The residents moved. The community did not. A community is not a set of people: it is a historically produced web of relationships between them. Destroy the web, & you have strangers in a building. The parallel to organisational life is uncomfortable.
When we restructure, we may preserve many of the people but destroy the relational infrastructure that made them effective. The informal trust that lets someone ask for help. The shared knowledge of who to call when a process stalls. The accumulated understanding of each other's judgment. These live in relationships, not individuals. Redrawing an org chart doesn't transfer them.
Research backs this up. Tacit knowledge - the "knowing how" driving real-world performance - depends on trust to flow. Break those relationships & you block the transfer. Studies show informal networks persist along old lines long after formal structures change, creating tension between old loyalties & new mandates. Social capital is the value created by connectedness. It can be destroyed in restructuring & take years to rebuild — a cost that almost never appears in a business case.
What leaders can do to protect collective value:
1. Audit informal networks before redesigning formal structures. Use, eg., System Network Analysis or Relational Coordination. Breaking key network nodes causes capability losses no productivity model captures.
2. Treat relational capital as a real cost. Business cases for restructuring rarely account for social capital destruction. Making it visible leads to better decisions & stronger cases for change.
3. Design around high-value relationships. Identify relationships carrying the most trust & history & actively design the new structure to protect them while enabling necessary change.
4. Invest deliberately in building new relationships. Create conditions for them to form through shared work, peer learning & social connection.
5. Give explicit attention to belonging & psychological safety for everyone (not just those who lose or change roles): This creates conditions for the discretionary effort that makes new structures succeed.
6. Slow down at the point of irreversibility. Ask not only "what do we gain?" but "what do we lose - & can we recover it?"
The value of an organisation is not the sum of its people's individual capabilities. It is the web of relationships between them. That web is not fungible.
Link to Joan Westenberg's essay: https://t.co/GFZo1McA7V. Thanks to @charlie_psych who sent me the essay.
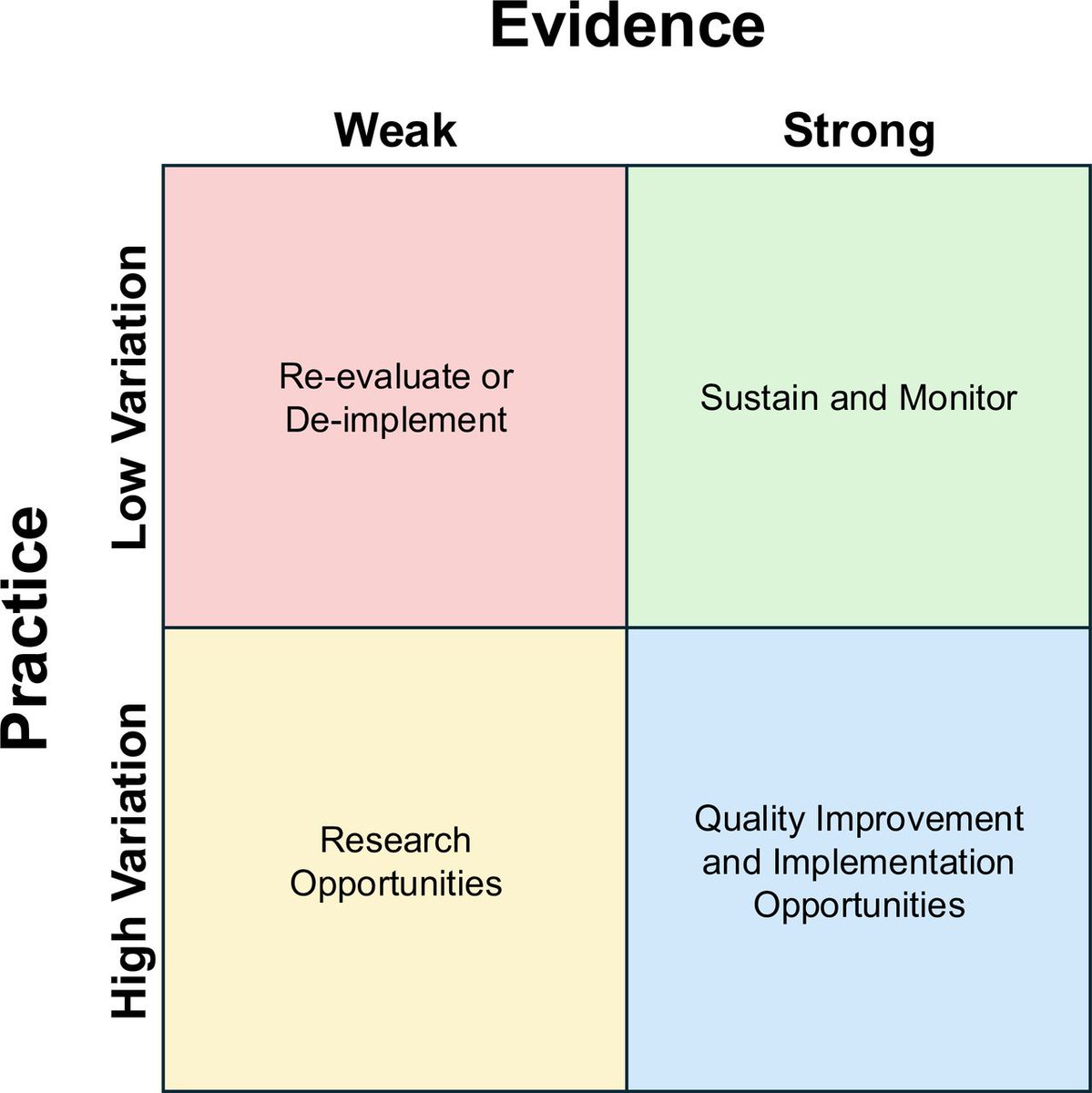
🎯 This Viewpoint argues that recognising specific association between the conduct of clinical practice and the quality of scientific evidence is a critical step to effectively improving healthcare quality.
A new framework maps clinical scenarios across 2 key dimensions: evidence strength (weak→strong) & practice variation (low→high) with each quadrant requiring a different improvement strategy
The message: match your improvement strategy to the specific evidence-practice relationship you're facing. Work smarter, not harder 💡
https://t.co/q7Y8X4eDsD
NABH at AI Bharat Expo 2026 | 𝗔𝗜 𝗥𝘅: 𝗥𝗲𝗶𝗺𝗮𝗴𝗶𝗻𝗶𝗻𝗴 𝗜𝗻𝗱𝗶𝗮'𝘀 𝗛𝗲𝗮𝗹𝘁𝗵𝗰𝗮𝗿𝗲 & 𝗣𝗵𝗮𝗿𝗺𝗮 𝗙𝘂𝘁𝘂𝗿𝗲
NABH marked its presence at AI Bharat Expo 2026, with Mr. Avinash Pandey, Group Leader – Digital Health, NABH, joining as a panel speaker on the evolving role of artificial intelligence in healthcare.
He emphasised the importance of NABH Digital Health Standards as a foundational framework for enabling safe, reliable, and trustworthy digital systems—critical for the responsible adoption of tech & AI in healthcare.
NABH continues to focus on three key pillars:
1. Data Quality – Accurate, standardised data
2. System Reliability & Validation – Consistent, validated system performance
3. Patient Safety & Accountability – Patient-centric care with clear accountability
As healthcare advances digitally, NABH is strengthening quality frameworks through its standards—not only for healthcare organisations, but also for the digital systems that support them. Building trust through robust standards, certification, and continuous monitoring remains essential for scaling AI in India.
#DigitalHealthStandards #AIinHealthcare #HealthTech #PatientSafety #QualityCare #AIBharatExpo #NABH
@jaxayshah l @rizwankoita l @ct_kannan@QualityCouncil
Does Confidence = Competence in Medicine? 🤔
We often assume a clinician’s certainty reflects diagnostic accuracy. It doesn’t.
A systematic review of 77 studies shows that confidence and accuracy are driven by different factors and miscalibration directly affects patient care.
🔴 Overconfidence → missed diagnoses, ignored cues, resistance to correction
🔵 Underconfidence → unnecessary tests, delayed treatment, reluctance to escalate
Diagnostic confidence is frequently misaligned with true accuracy, shaping decisions around testing, prescribing, and referrals.
🧠 What doesn’t predict accuracy:
- Time spent deciding
- Volume of information considered
- Clinician mood or personality
✅ What does help:
- Strong medical knowledge
- High-quality information gathering
- Feedback on diagnostic outcomes
The review proposes a 3-level model to support better calibration through education, cognitive tools, and targeted system-level interventions.
Read the full systematic review to learn how clinicians, educators & health systems can improve diagnostic confidence here: https://t.co/NObqAJZnwf
The truth is out, and it’s sobering. According to the 𝐖𝐇𝐎 𝐄𝐮𝐫𝐨𝐩𝐞: 𝐇𝐞𝐚𝐥𝐢𝐧𝐠 𝐇𝐚𝐧𝐝𝐬 – 𝐇𝐮𝐫𝐭𝐢𝐧𝐠 𝐌𝐢𝐧𝐝𝐬 (𝟐𝟎𝟐𝟓) 𝐫𝐞𝐩𝐨𝐫𝐭, the very people keeping our healthcare systems alive are at a breaking point.
Over 𝟓𝟎% 𝐨𝐟 𝐧𝐮𝐫𝐬𝐞𝐬 are reporting symptoms of anxiety and burnout. We aren’t just facing a "𝐬𝐭𝐚𝐟𝐟𝐢𝐧𝐠 𝐬𝐡𝐨𝐫𝐭𝐚𝐠𝐞", we are witnessing the rise of "𝐍𝐮𝐫𝐬𝐢𝐧𝐠 𝐃𝐞𝐬𝐞𝐫𝐭𝐬," where entire communities are losing access to the care they need to survive.
At the 𝐖𝐨𝐫𝐥𝐝 𝐏𝐚𝐭𝐢𝐞𝐧𝐭𝐬 𝐀𝐥𝐥𝐢𝐚𝐧𝐜𝐞, we know that you cannot have Patient Safety without Nurse Well-being. When the "𝐇𝐞𝐚𝐫𝐭 𝐨𝐟 𝐇𝐞𝐚𝐥𝐭𝐡𝐜𝐚𝐫𝐞" is hurting, the entire system is at risk.
It’s time to move beyond the applause.
𝑊𝑒 𝑛𝑒𝑒𝑑:
Safe staffing ratios that prevent exhaustion.
Fair, livable wages that reflect their expertise.
Real mental health support for frontline workers.
We are taking this data to the global stage, but we need your voice.
𝐒𝐇𝐀𝐑𝐄 𝐭𝐡𝐢𝐬 𝐩𝐨𝐬𝐭 𝐭𝐨 𝐛𝐫𝐞𝐚𝐤 𝐭𝐡𝐞 𝐬𝐢𝐥𝐞𝐧𝐜𝐞 𝐨𝐧 𝐭𝐡𝐞 𝐡𝐞𝐚𝐥𝐭𝐡𝐜𝐚𝐫𝐞 𝐜𝐫𝐢𝐬𝐢𝐬.
𝐓𝐀𝐆 𝐚 𝐡𝐞𝐚𝐥𝐭𝐡𝐜𝐚𝐫𝐞 𝐰𝐨���𝐤𝐞𝐫 who deserves more than just a "𝐭𝐡𝐚𝐧𝐤 𝐲𝐨𝐮" today.
𝐃𝐚𝐭𝐚 𝐒𝐨𝐮𝐫𝐜𝐞: 𝐖𝐇𝐎 𝐄𝐮𝐫𝐨𝐩𝐞 (𝟐𝟎𝟐𝟓). Healing hands – hurting minds: Survey on the mental health of health and care workers.
#WorldPatientsAlliance #HeartOfHealthcare #NurseBurnout
@WHOAFRO
@WHO_Europe
@UN
@UNICEF
@WorldBankGroup
@OECD
@SigmaNursing
@ghc_global
@IHF_FIH
@ISQua
@TheIHI
@PLAN4ZERO
@GlobalFund
@NursingNow2020
@HWALLIANCE
@mentalhealth
@PublicHealth
@HIMSS
@ICNurses
@HowardCatton
@JHUNursing
@NurseStandard
@AAN_Nursing
@YaleNursing
@AmbCareNursing
@DarlingtonUnion
@ANANursingWorld
@HelenBevan@SessionLab This si something people should consider while conducting chain of trainings or workshops without proper handholding mechanisms.
Thanks for sharing Helen.
Register to join us for our 'Tea-Time QI webinar' on 19th March 2026 to learn how to do process flow mapping in healthcare facilities.
Click the link below or scan the QR code:-
https://t.co/iPXIfWYXop