Know how some surgeons carry around a keychain trach just in case they need an emergent airway in public? I think I want to carry around calipers in case I see a crowd of people gathered around a tough rhythm strip.
All valid but counterpoints:
1. Lots of new AI-powered medical technology is going to be prototyped
2. It will all be vulnerable to criticism through traditional lenses like this
3. Some of it is going to work
4. Practicing medicine may provide little intuition about which things are going to work and which won’t (see coding/software engineering)
@drjohnm Rather than AC vs LAAC a better framing may be three axes of stroke risk reduction for those at elevated risk:(1) AC for nearly all (2) rhythm control when appropriate and (3) LAAC in cases of high residual risk or intolerance to AC.
Sure, you could use AI to summarize papers and explain them at a level anyone could understand... or you can turn the abstracts into music videos for no reason.
The tools are not perfect yet, but the disparate elements (consistent characters, lip syncing, etc.) are evolving fast
Physicians cannot bear the responsibility alone here. The risk has to be distributed among our vendors, institutions, and at some level even patients will have to “buy in” (assume some of the risk) too. There are models for this in other industries that automate critical functions (e.g., autopilot).
Healthcare is a very difficult space because the risks and benefits are both potentially very high and we are woefully under-resourced relative to other sectors that don’t have our systemic disadvantages (locked down data, human lives at stake).
And right now we don’t know whether these systems will show superhuman effectiveness across domains or have a much narrower range of applicability. We have to prepare for all scenarios. A lot of these balancing questions also transcend healthcare, alignment is not at all guaranteed. A lot of work to be done by people interested in it, and it’s our best hope at shaping what it all looks like.
Re-learning teaching in order to teach.
Superhumanization is opposite of self-acceptance.
AI[validated] needs to be a flashlight to illuminate and not our eyes or brain.Wisdom remains ground truth.
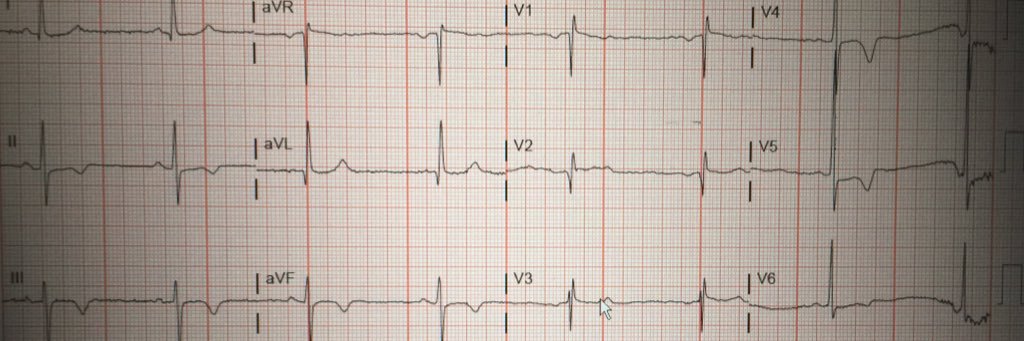
Calibrating AI Reliance—A Physician’s Superhuman Dilemma https://t.co/3CsJujCGlU
Congratulations to Dr. Colleen McIntosh who won first place in #qualityimprovement during the poster session at this year’s Hospital Medicine Conference #HowWeHospitalist
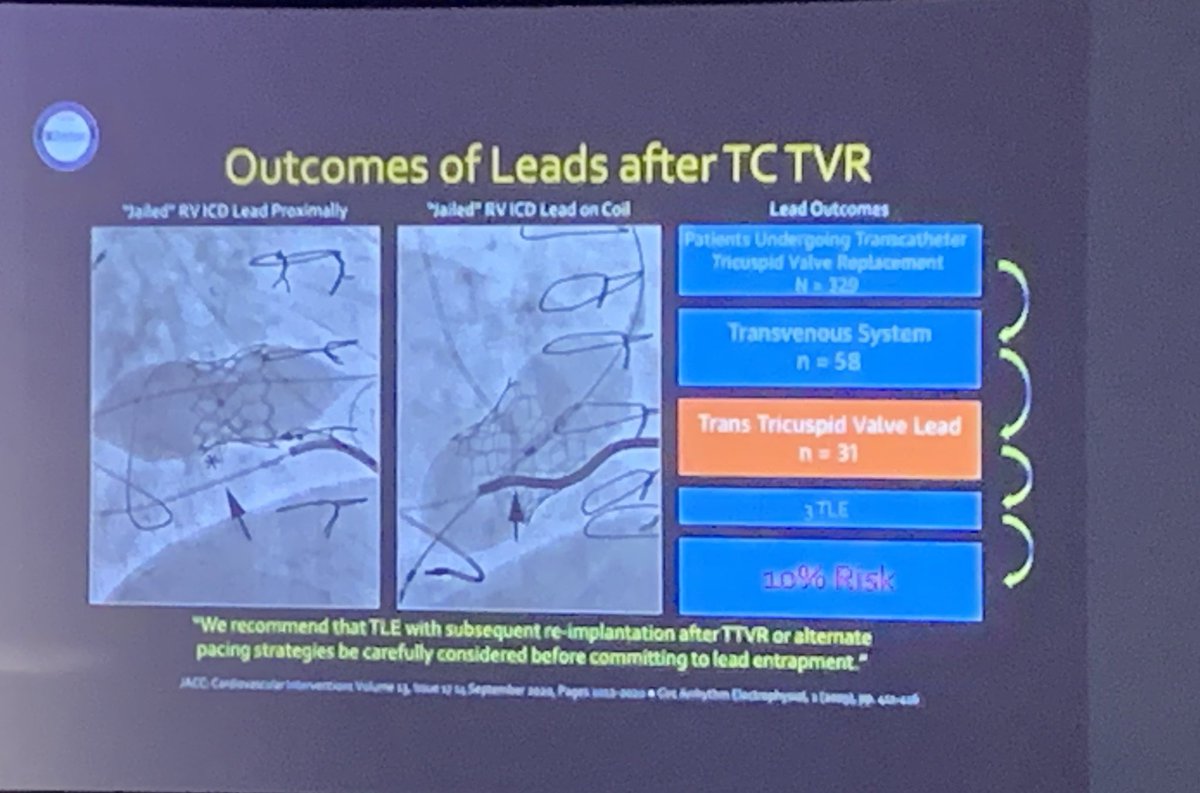
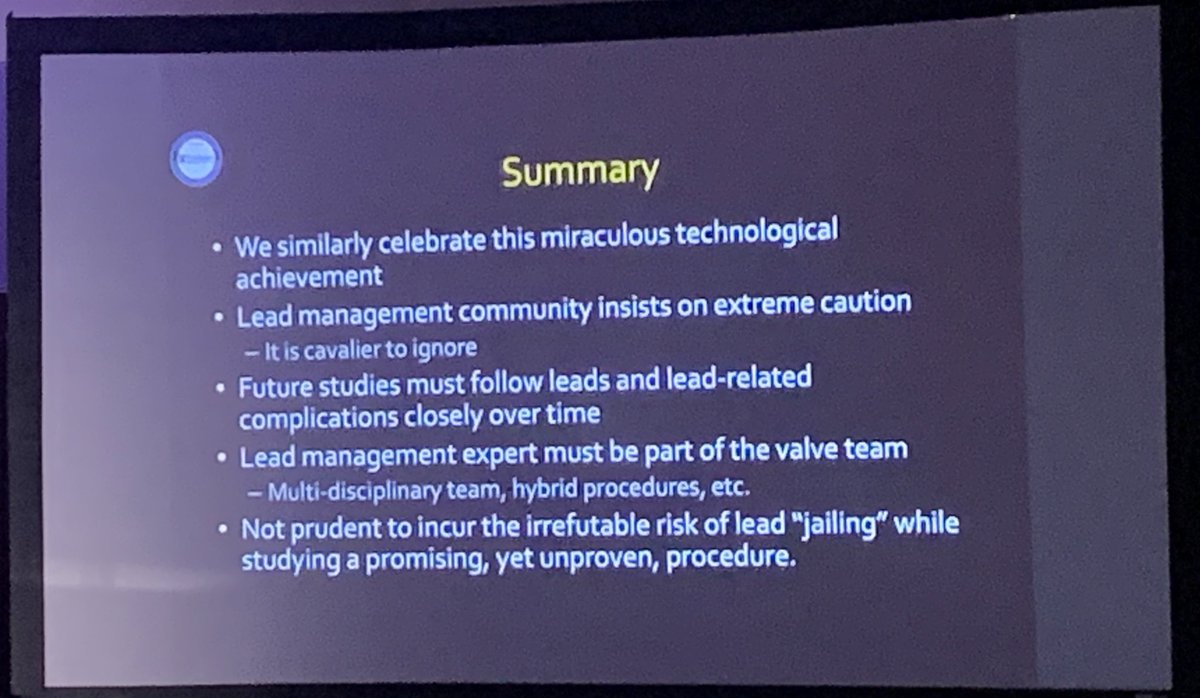
Transcatheter TV interventions
JAILING pacemaker/ICD leads - @rdschaller
⭐️ Get #EPeeps on the CV team *early*
Jailing is has risks!
🗑️ lead damage (esp pacer dependent pts)
🗑️ ⬆️⬆️difficulty & risk w/ later extraction - may be committing pts to surgical extraction
#ACC23
The first book of the UCLA- Amara Yad project-providing highest quality open access content for all! Thank you to @Cardiotext for partnering in this important project! Free download https://t.co/TZgOPGSX1i @dgsomucla@Ed_Gerst @clancyatheart @DrRoderickTung
Great VT-focused session this week with @AbbottNews, @MRobinsonEP, @Dr_Santangeli, and Frank Marchlinski in Austin, TX. The discussion of bevel orientation during epicardial access came in handy today when trying to obtain access to a “dry” Capri Sun!