Rethinking Surgical Trials in Esophagogastric Cancer
by Das B, Mitra AT, Bossuyt P and Hanna GB in Ann Surg Oncol
🪡 read our summary 👉 https://t.co/g4O6t4v9D4
📖 read the article: https://t.co/1JvCMqFZKD
Fantastic to see our pan-European GI robotic training survey of >1,000 responses in print! @EAES_eu@ERSC_Study@josiewalshaw1@my_ueg
@ALSGBandI
@IrcadFrance@bariatricBOMSS
https://t.co/5MqCzN47PF
Register your interest for our upcoming Delphi study:
https://t.co/Bbmy9Dg0Qi
Nice slide to show outcomes of perioperative chemo vs CTRT for all trials in GE junction and Stomach adenocarcinoma. Good for discussion with patient in clinic . @myESMO
Pleased to share our 5 yr outcomes of Bariatric surgery vs conventional weight loss for people living with anti-retro viral virus https://t.co/h6aJCgG74q @MatyasSurg@Bariatric_doc@JournalObesity@ChelwestFT
Development and validation of a virtual teaching method for minimally invasive surgery skills: a prospective cohort study @IJSurgery@MatyasSurg@Imperial_LGSSP
https://t.co/ANJ4rvGIlT
@ElliotServaisMD@DouglasAdlerMD@Daniela_Molena After initial enthusiasm for stents, we’ve largely moved away from them to palliate dysphagia unless as a last resort. Too many other symptoms as mentioned in the thread. Chemotherapy resolves most dysphagia by the 2nd cycle in locally advanced cases. https://t.co/dEGzaq5sXG
Read @young_bjs 'Acute threat to Life' series!
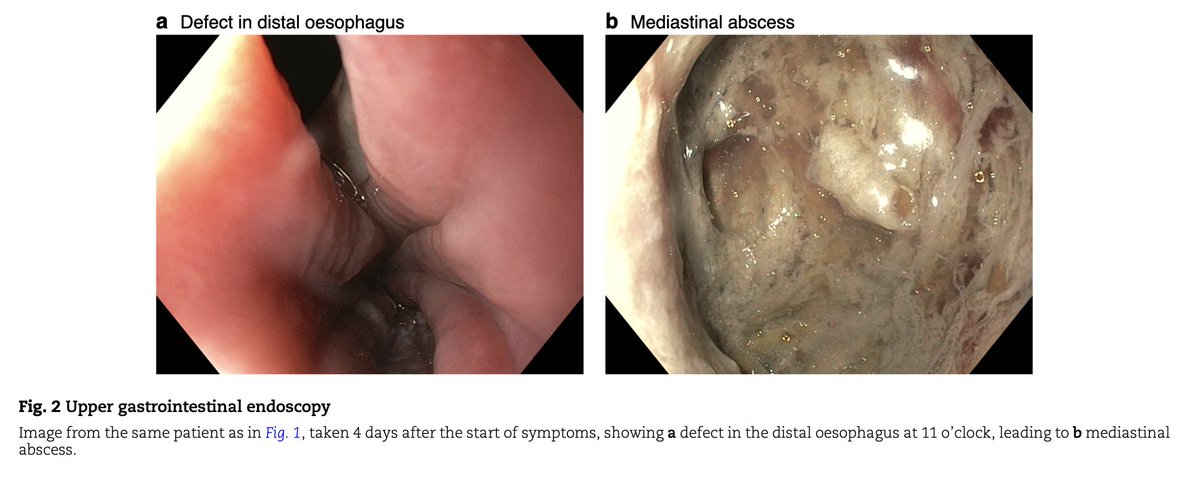
🔟Boerhaave syndrome
https://t.co/uoZ0c4NZVP
- It's a surgical emergency, defined as a spontaneous perforation of the oesophagus, typically located in the distal left posterolateral aspect
- The most common clinical presentation is vomitting followed by chest pain combined with signs of infection
- The initial diagnostic work-up consists of contrast-enhanced CT of the chest and upper abdomen
- The mainstay of treatment is endoscopic or surgical closure of the oesophageal defect and drainage of perioesophageal fluid collections ➡️depending on the treating centre’s individual experience and preference, with no guidelines currently available
Great work by Tobias Hauge, Aram Abu Hejleh, Magnus Nilsson, Wolfgang Schröder
#SoMe4Surgery #MedTwitter #SurgEd #Surgery
@RCPSGTrainees @aecirujanos@SEIQuirurgica@iss_sic #MedicalTechniques @BJSAcademy@young_bjs@BJSOpen@des_winter@evanscolorectal@robhinchliffe1@bplwijn@ksoreide@MalinASund@nfmkok@TejedorPat@paulo_sutt@PVaughanShaw@JJEarnshaw@juliomayol #SoMe4Trauma #emgensurg
@WSESurgery@NELANews #EmLap @ASGBI_MA
#some4peds
Effect of chemotherapy/targeted therapy alone vs. chemotherapy/targeted therapy followed by radical surgical resection on survival and quality of life in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction. https://t.co/UY2Pmj9xWx
Proud to share this major collaborative effort with everyone. I will share my thanks at the end of this thread.
But first, I want to share some key points to take away from this paper on #cancer risk due to #CDH1...
I am pleased to inform you that the primary result of JCOG1109 was published in the Lancet today. The neoadjuvant triplet chemotherapy would be the standard care for the locally advanced ESCC. Many thanks to everyone involved. https://t.co/YvNAwbLdUO
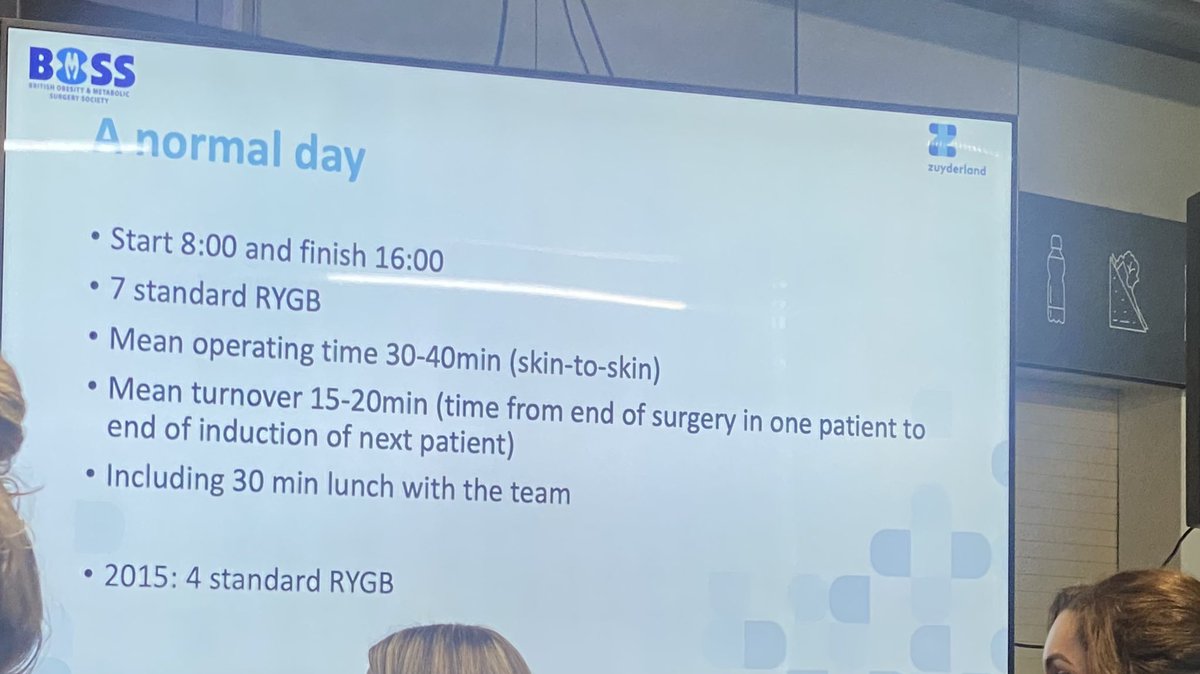
@mstotty88@LucyLucyHuppler@bariatricBOMSS Surgeon speed is a taboo in 🇬🇧 but must be addressed. The variation is massive & slow surgery is expensive & a waste of valuable resources
These rates of theatre efficiency from Pieter Broos, Zuyderland hospital in the Netherlands from @bariatricBOMSS. That’s an 8-4 day of operating many of us can only dream of. There’s so much work to do in the UK on so many levels to have any hope of matching this 😵💫