If you’re looking to take the PLAB exam or the MRC exam and are planning to train or work in the UK this episode of the @slidingscalepod is definitely for you!
Check it out!
Had the pleasure of talking to Dr Aakanksha about her journey to the UK and her experience within the NHS.
It’s not easy to leave your home country and relocate for training and work. And in a profession in which training maybe endless, this can be a daunting task.
Had a fantastic conversation with @docritsin, co founder of @rockethealthIN about entrepreneurship in the field of medicine.
The spirit, the passion and the resilience that embodies both medicine and the start up mentality— it’s all here. ⤵️
Had the opportunity to host @siddhant_k11 on our podcast.
Dr. Siddhant Kashyap, spoke about his journey as the founder of @humans_medicare , his work as an entrepreneur and the role that self belief has played in making him who he is today.
Check out the full episode here ⬇️
@AdiG1993 I’m an internist. And I feel this acutely every single day.
Even though I’m trained to handle emergencies with confidence, everyday my decisions and intentions are questioned.
No one says it. But they look like “you’re just an MD, what would you know.”
It sucks.
If you’re interested in neurology and the nuances of clinical examination, this is a great thread! Thank you @zach_london for making this so easy to understand!
Saw another patient with sensory neuronopathy who had been misdiagnosed with functional neurological disorder.
What is sensory neuronopathy, and why do we keep missing it? A #tweetorial.
1/
Hi #medtwitter !
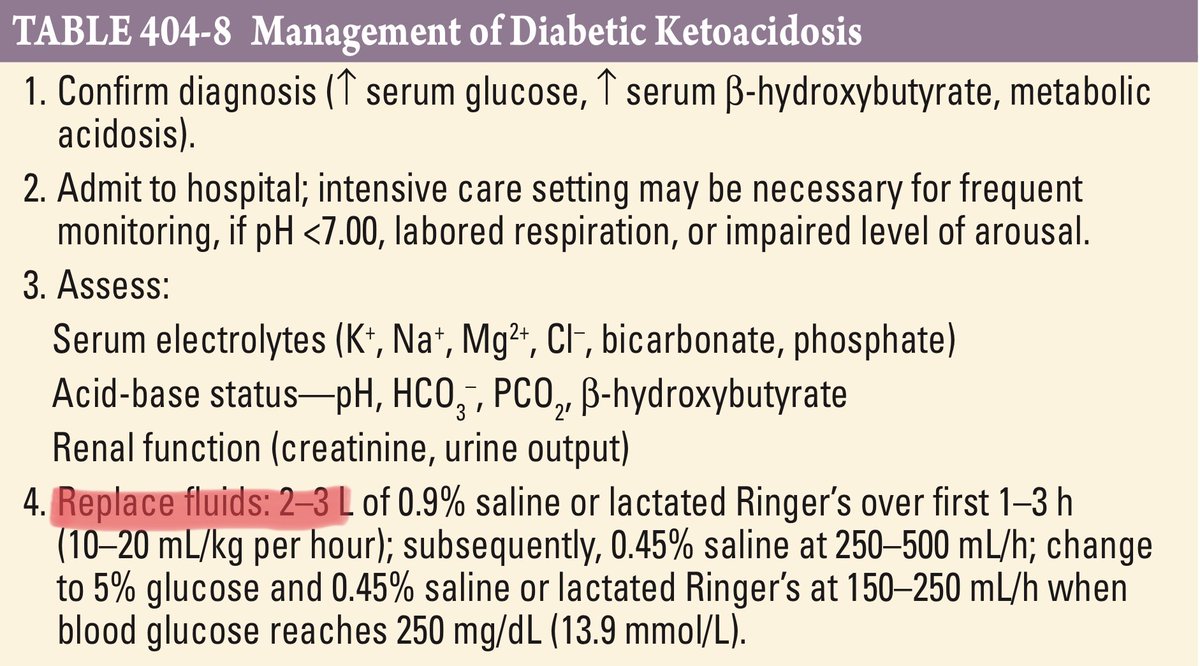
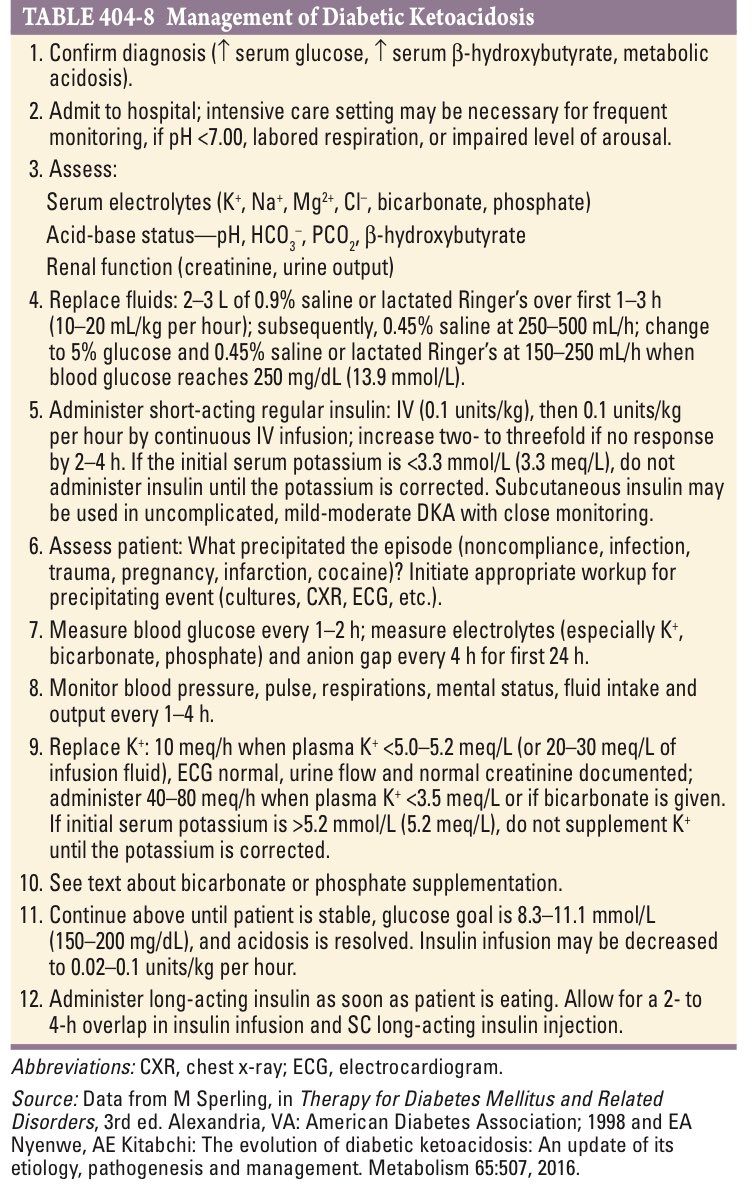
This is a screenshot from Harrison of the management of DKA.
I want you to look at just the fluid management part.
Why is it recommended that we give so many different types of fluids?
A short 🧵on why we do what we do!
Middle aged female in ICU with urosepsis
Norepinephrine (NE) ion is started in (ED) via peripheral IV.
On arrival to ICU, it was noted that peripheral IV was not functional, and there was a significant amount of NE extravasated in underlying tissues.
What is your next step?
@Country_fiedMD@ercowboy@ecgrhythms Glad I’m not alone! I’ll keep your advice about lyrics and nitro in mind if I’m faced with such a situation again! 😊👍🏻
Hey #cardiotwitter!
Had a 62/F came with chest pain intermittent for the past two days. Hypertensive, on treatment. ECG ⬇️.
BP 180-190/110mmHg.
I don’t work in a PCI Center, so I referred her. But acute inferior wall MI, with CHB do you treat the HTN?
If yes, with what?
I wish I could say kill them with kindness. But I’ve increasingly found that it doesn’t work in this field.
So yeah. Do your best to ignore bullies. If it’s not working so well, by all means out bully them.
Bullies understand only one language- strength. The only way to beat a bully is to outbully him/her. Take whichever branch you like - and if you meet a bully, rain hell on them. Show them actions have consequences.
All the best !
@Mycro_ftHolmes @The_Nanashi_O I thought so too. But I had to choose between lowering the BP with labetalol (not advised in CHB) or letting the BP stay high till the patient reached the PCI centre.
@ercowboy@ecgrhythms And I know that situation seems ridiculously theoretical. But in relatively resource poor settings, this was a very real situation.
@ercowboy@ecgrhythms Yeah for sure treating the MI is the priority. But I was in that interim period before shifting her to a PCI Center.
In a situation where I could either give her labetalol to reduce her BP or shift her without giving her anything. What do I do?