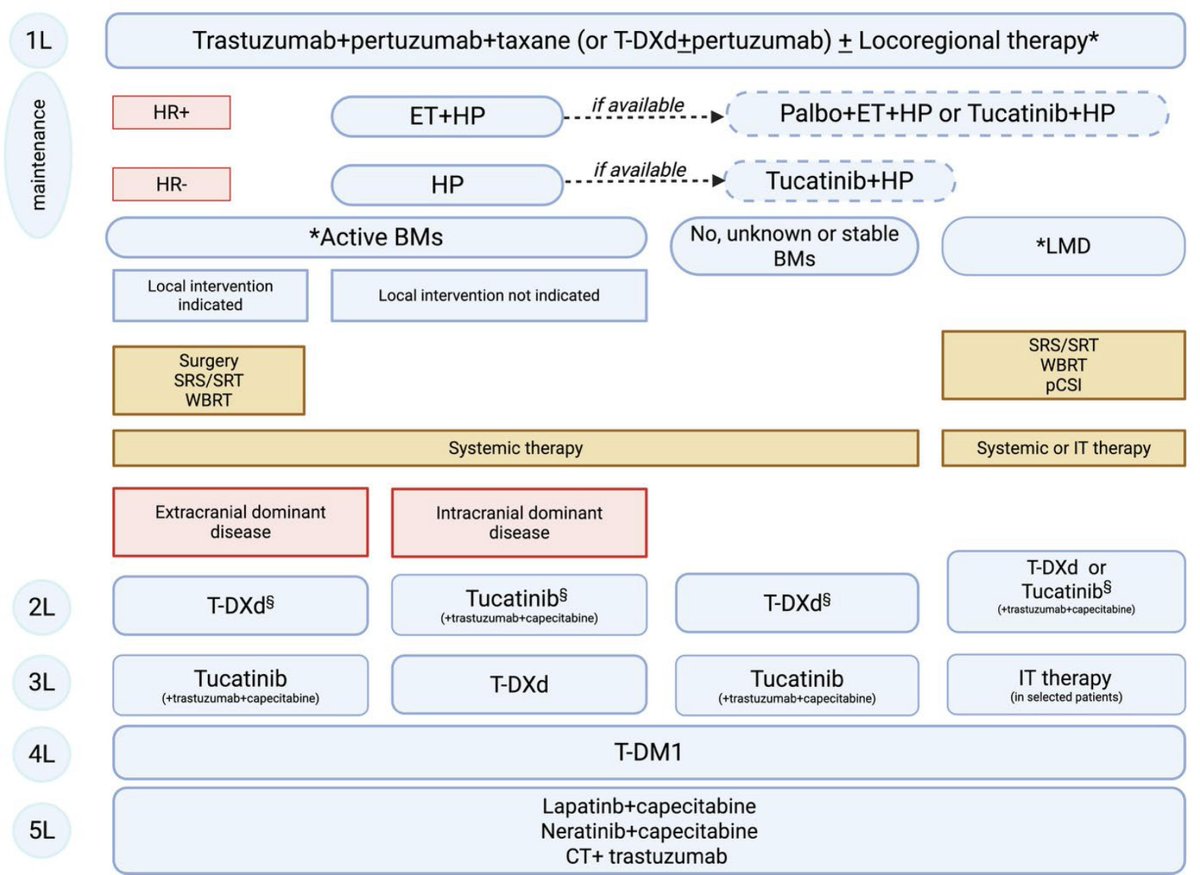
Central nervous system and leptomeningeal metastases in patients with HER2-positive breast cancer: A comprehensive review and therapeutic algorithm proposal
https://t.co/DhmTm5545R
🚨 AstraZeneca update in bladder cancer.
Phase III VOLGA trial met its primary endpoint:
Perioperative durvalumab (Imfinzi) + neoadjuvant enfortumab vedotin (EV) significantly improved EFS in cisplatin-ineligible or cisplatin-declining MIBC. 🔥
🧪 Trial arms:
1️⃣ Durvalumab + EV + tremelimumab
2️⃣ Durvalumab + EV
🆚
🏥 Radical cystectomy ± adjuvant therapy
📌 Key takeaways:
✅ Statistically significant & clinically meaningful EFS benefit
✅ Favorable OS trend
✅ Manageable safety profile
✅ Potential perioperative option for cisplatin-unfit patients
After NIAGARA and POTOMAC, VOLGA becomes another major positive perioperative bladder cancer readout for durvalumab.
The perioperative uro-oncology landscape is changing rapidly.
📖 Full release in comment ⬇️
#BladderCancer #uroonc #MedTwitter @OncoAlert@myesmo@esmo_open@asco@AstraZe
ESMO Breast 2026 — key trials at a glance
• HER2+ trials
• HR+/HER2− trials
• TNBC / ADC / Immunotherapy trials
Major studies, key results, and clinical take-home messages — all in one quick visual summary.
#ESMOBreast2026#BreastCancer#Oncology#MVOnco
هاتف عملة (قرص) والذي كان موجودا في شوارع المدن
ويعتبر هذا النوع من النوادر، لأن هاتف العملة (قرص) لم ينتشر كثيرا في السعودية، فكان استخدامه محدودا، ثم جاء بعده هاتف عملة (أزرار) واستمر مدة طويلة #stc
وبرفقه صورة قديمة ملتقطة في مدينة الرياض، ويبدو أن الصورة في سوق الخضار بعتيقة.
ER-Low Tumors (1-10%): Do They Really Need Adjuvant Endocrine Therapy?
ER-low tumors behave similar to ER-negative disease
Significantly worse survival than ER-high (>10%) tumors
Adjuvant Endocrine Therapy (AET) shows NO benefit in ER-low (1-10%) or ER-negative
Clear long-term benefit seen only in ER-high (>10%)
Practice-Changing Takeaway:
ER 1–10% → Treat as endocrine-insensitive (like ER-negative)
Study: 13,607 patients | 26-year follow-up
#MVOnco #BreastCancer #ERLow #Oncology #ESMOBreast2026 #PrecisionMedicine
https://t.co/SFzKbaclML
There will be people who agree & disagree with @US_FDA decision on #SERENA6#cami, but fantastic document by FDA 👏 educating & clearly outlining reasons for the decision and how PFS2 will be interpreted.
A must read for drug developers and pharma.
In the phase 3 ATOMIC trial in resected stage III mismatch repair–deficient colon cancer, adding atezolizumab to modified FOLFOX6 improved 3-year disease-free survival, with a higher incidence of grade 3 or 4 toxic effects, mainly fatigue. Full trial results: https://t.co/XASue2CCiE
Editorial: ATOMIC Energy — Biomarker-Bespoke Adjuvant Therapy for Colon Cancer https://t.co/mEj5Oqw68H
نحمد الله سبحانه وتعالى أن أكرمنا بإتمام صيام شهر رمضان المبارك وقيامه، ونسأل الله أن يديم علينا أمننا واستقرارنا، وأن يحفظ أبطالنا البواسل على الثغور والحدود في مختلف القطاعات العسكرية والمدنية.
وكل عام وأنتم بخير، وبلادنا في عز ورفعة.
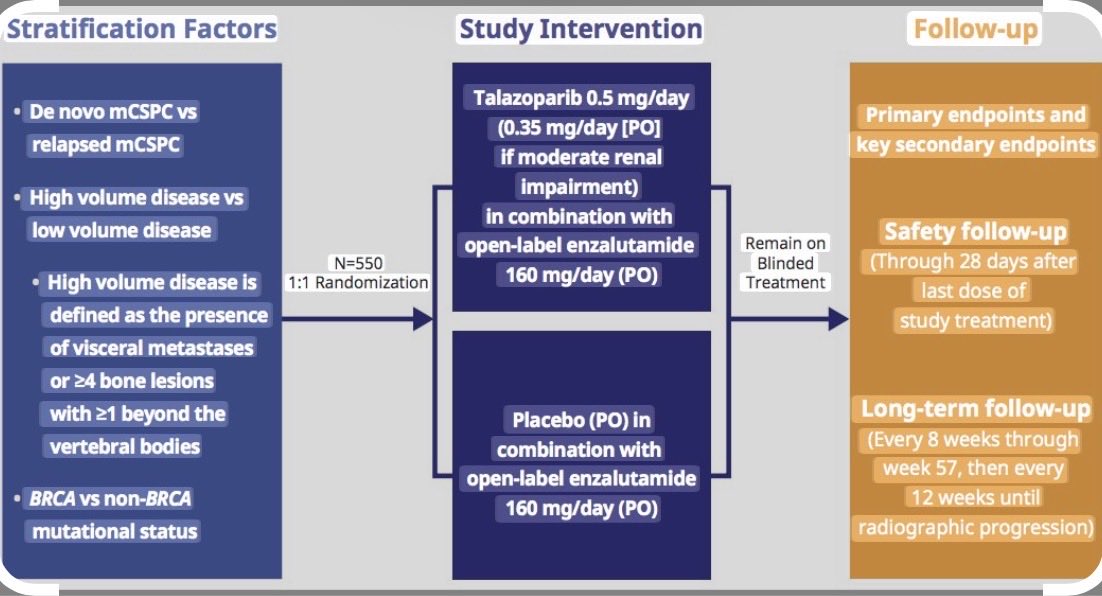
#EAU26 Dr. von Amsberg on when to introduce PARPi: mHSPC or should we wait until mCRPC?
🧬 BRCA1/2-mutated mHSPC behaves differently.
• Poorer prognosis
• Less benefit from ARPIs/docetaxel
• PARP inhibitor combinations show the strongest rPFS signal (emerging OS) in BRCA1/2
💡~1 in 4 men never receive another line of therapy → effective treatments may need to move earlier, not later.
@uroweb@UroToday
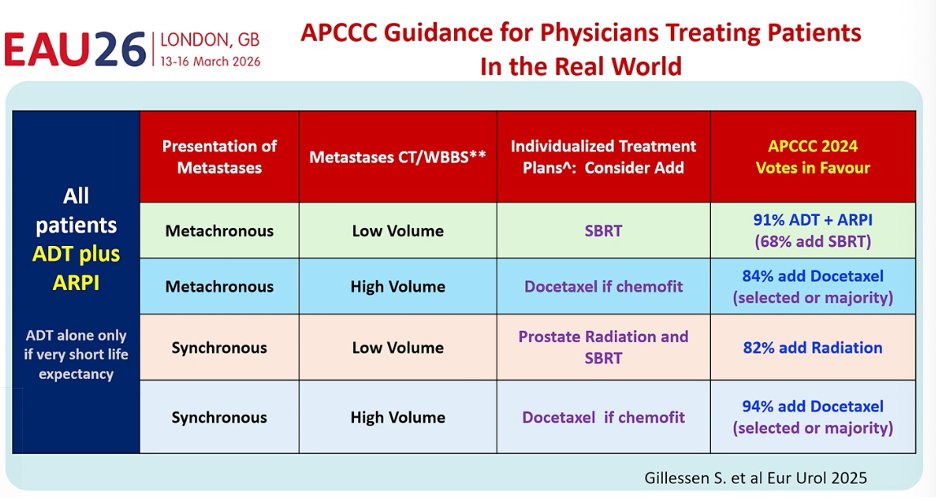
#EAU26@ChrisSweens1: the field is reaching a consensus in mHSPC.
ADT + ARPI for nearly all patients, then personalize intensification:
• SBRT for low-volume
• Prostate RT in synchronous disease
• Docetaxel if high-volume and chemofit
🕒 The hope for the future: biomarkers to guide therapy, global access, and drug prices coming down so evidence-based care becomes feasible worldwide.
@uroweb@UroToday
RECITE: In a phase 3 trial in patients with persistent chemotherapy-induced thrombocytopenia, 84% of those receiving romiplostim had no chemotherapy dose modifications, as compared with 36% of those receiving placebo (odds ratio, 10.16). Full trial results: https://t.co/5GoloaFC0A
Editorial: Thrombopoietin-Receptor Agonists in Chemotherapy-Induced Thrombocytopenia https://t.co/LdbOSSeGxt
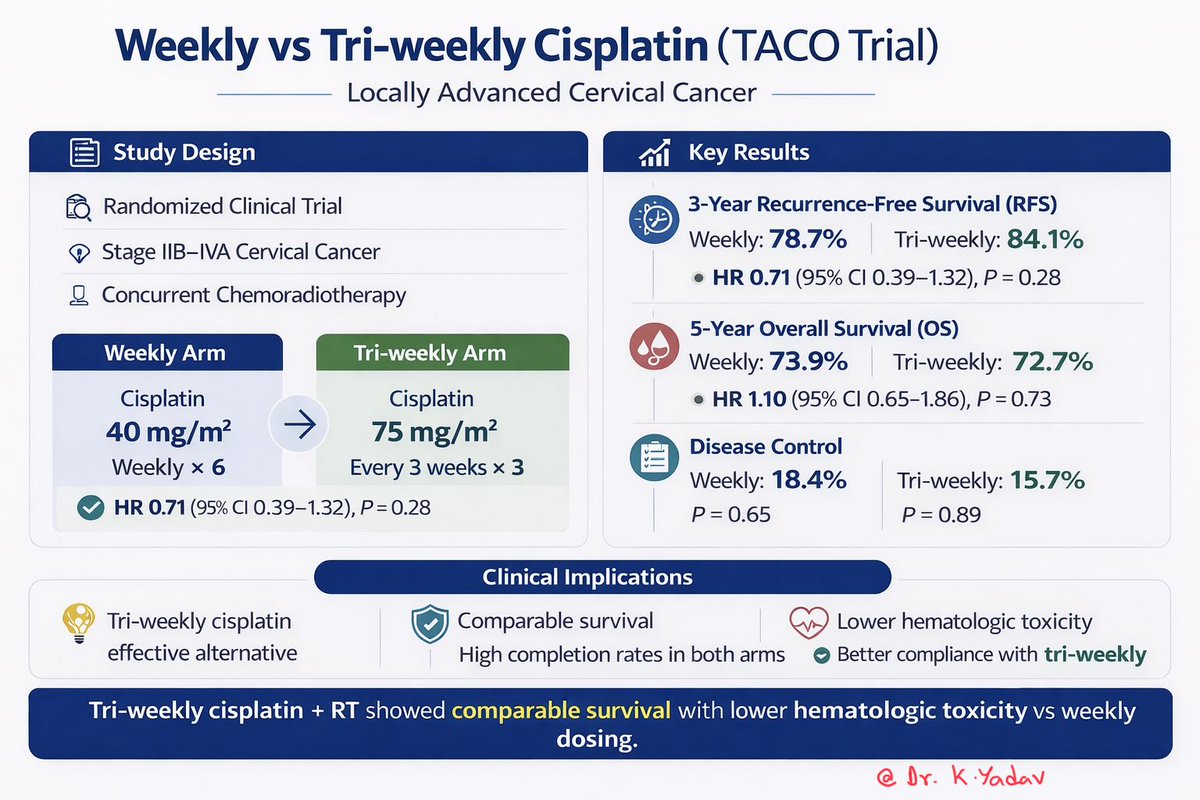
TACO Trial
Tri-weekly cisplatin (75 mg/m² q3w) vs weekly cisplatin (40 mg/m²) with concurrent RT in LACC.
Results:
• No difference in RFS or OS
• Similar recurrence patterns
• Lower hematologic toxicity with tri-weekly dosing
Clinical takeaway:
Tri-weekly cisplatin is a valid alternative regimen.
#CervicalCancer #OncologyResearch @OncoAlert@oncodaily@DrBarbiOnc@CCAENetwork@myESMO@ValenzaCarmine@stolaney1
نعم، تمتلك #السعودية أحد أكبر أساطيل المقاتلات الجوية في الشرق الأوسط ومن بين الأكبر عالميًا، لكنها في المقابل تؤكد أن عقيدتها العسكرية تقوم على حماية سيادتها وأمنها لا الانخراط في الحروب أو الاصطفاف في صراعات الآخرين…
السعودية 🇸🇦 تمتلك منظومة دفاع جوي متقدمة ومتعددة الطبقات أثبتت كفاءتها في التصدي للصواريخ والطائرات المسيّرة، وتحمي أجواءها باحترافية عالية، ما يعكس قوة الردع وقدرة المملكة على حماية أمنها واستقرارها دون الانجرار إلى حرب إقليمية.
#امنون_مطمئنون
gBRCA-Mutant Luminal Breast Cancer: CDK4/6 or PARP Inhibition?
CDK4/6 inhibitors combined with ET have become the central therapeutic backbone of HR+/HER2− BC. This paradigm has proven remarkably durable across both aBC and high-risk eBC. Yet gBRCA1/2 mutations introduce a biological context that may challenge the assumption that all luminal tumors behave similarly under CDK4/6 inhibition.
A recent clinicogenomic analysis published in Nature provides an important piece of this puzzle. In a cohort of more than 5,800 patients, gBRCA2 mutations were strongly associated with HR+/HER2− disease and with a genomic landscape enriched for alterations linked to CDK4/6 resistance, including RB1 loss-of-function, MYC amplification, and AURKA amplification. This constellation suggests that BRCA2-mutant luminal tumors may harbor a baseline vulnerability that facilitates escape from CDK4/6 inhibition. In clinical cohorts from the same study, pts with gBRCA2 mutations experienced significantly shorter PFS under CDK4/6i + ET compared with BRCA-wild-type patients.
This biological signal aligns with the clinical observation I reported in my recent meta-analysis presented at ESMO 2025. Across 5,002 evaluable patients with HR+/HER2− mBC receiving CDK4/6i + ET, gBRCA1/2 mutations were associated with significantly worse PFS and OS compared with wild-type tumors. Importantly, the adverse effect was most pronounced in the gBRCA2 subgroup, suggesting that this genotype may identify a population in which CDK4/6-based strategies are less durable.
Taken together, these data do not support abandoning CDK4/6i in BRCA-mutated BC. Rather, they suggest that gBRCA2-mutant HR+/HER2− BC may represent a biologically distinct luminal subtype in which resistance pathways are primed early. In practical terms, this distinction matters most when considering treatment sequencing.
In the metastatic setting, CDK4/6i + ET remain a reasonable first-line option in patients with endocrine-sensitive disease, long DFI, and low tumor burden. However, aggressive clinical features—short DFI, primary endocrine resistance, or high tumor burden—earlier use of PARPis may be biologically justified. The Nature analysis notably showed that PARP inhibition often produced longer disease control even when administered after CDK4/6 therapy, reinforcing the concept that HRD remains a therapeutically exploitable vulnerability.
The implications extend to early disease as well. Adjuvant olaparib has demonstrated a clear survival benefit in high-risk HER2-negative gBRCA-mutated BC, establishing PARP inhibition as a biologically targeted strategy in this population. At the same time, adjuvant CDK4/6is have shown meaningful benefit in high-risk HR+/HER2− eBC. Abemaciclib now has OS support in long-term F/U of the monarchE study, and ribociclib has demonstrated durable iDFS improvement in the NATALEE trial.
These advances raise a practical question in patients who meet criteria for both approaches—particularly those with gBRCA-mutant, node-positive HR+/HER2− early BC with substantial residual risk. In such cases, it may be overly simplistic to frame treatment as a choice between PARPi and CDK4/6i. Instead, these therapies target distinct biological layers: PARP inhibitors exploit HRD, whereas CDK4/6is suppress residual luminal proliferative signaling.
From this perspective, a sequential strategy—such as one year of adjuvant olaparib followed by CDK4/6i in selected very high-risk pts—can be considered a biologically rational approach, even though prospective evidence for this sequence is currently lacking. For patients with substantial nodal burden or RD after neoadjuvant treatment, integrating both mechanisms may be a reasonable risk-adapted strategy.
#X comment
Phase 3 LITESPARK-011: Belzutifan + Lenvatinib vs Cabozantinib in pretreated metastatic clear cell renal cancer #GU25 shows +ve PFS HR 0.75 , OS HR 0.85 (non-significant), ⬆️ RR 53% vs 40%, G3+ TRAEs 72% vs 66%. Cabozantinib is hard to beat making this a standard of care. Using the most active drugs first rather than sequencing is debatable, but not all patients can sequence. We still don’t have significant OS post in IO refractory RCC @OncoAlert