Realizamos nefrectomía lumboscópica izquierda por caso de exclusión renal, una vía que nos permite evitar cavidad abdominal y abordaje inmediato para control vascular, en casos bien seleccionados siempre es bueno tenerlo dentro del arsenal quirúrgico urológico.
En este caso al ser institucional utilizamos balón de Gaur modificado (nelaton, dedo de guante y seda) para la sustitución de SpaceMaker, aunque sin la misma efectividad, válido para cuando no se cuenta con dicho recurso.
Come watch this #MiniPCNL from start to finish -from the simplified 0–90 access technique to the final witdrawal of the percutaneous access sheat-
Sorry for my English, I’m not as fluent as I’d like to be
Also U can watch it at https://t.co/FQ8lhXM7s7 in 4k resolution
@RomanCarvajal@urobraulio@Endo_Society@AmerUrological@smumexico #endourology
Introducing the South Central Section representatives at the AUA2026 Residents Bowl! 🟢 Wear green to cheer on ProState of the Union.
The attendee with the most Section spirit will win a special prize on the first day of competition! 🏆
#AUA26#Urology
It's time once again to vote for your favorite Residents Bowl team name! The winning name will be honored with a special button at AUA2027! Voting closes May 13.
Click here to vote now! ➡️ https://t.co/vbTJcUVS9X
Mi médico siempre llegaba 45 min tarde a cada cita.
Ni una disculpa, solo un "Siéntese".
La última vez esperé una 1h y 20 min y me fui.
Luego escribí una reseña en Google. No fui grosero, solo honesto: "Siempre llega tarde, trae un libro". 2 estrellas.
Esa noche me llamó ⬇️
Uropatia obstructiva (en donde el flujo de la orina del riñón a la vejiga se obstruye) secundario a cálculo ureteral obstructivo, una verdadera URGENCIA UROLÓGICA, en descripción gráfica 😍…
Créditos: @io_voka
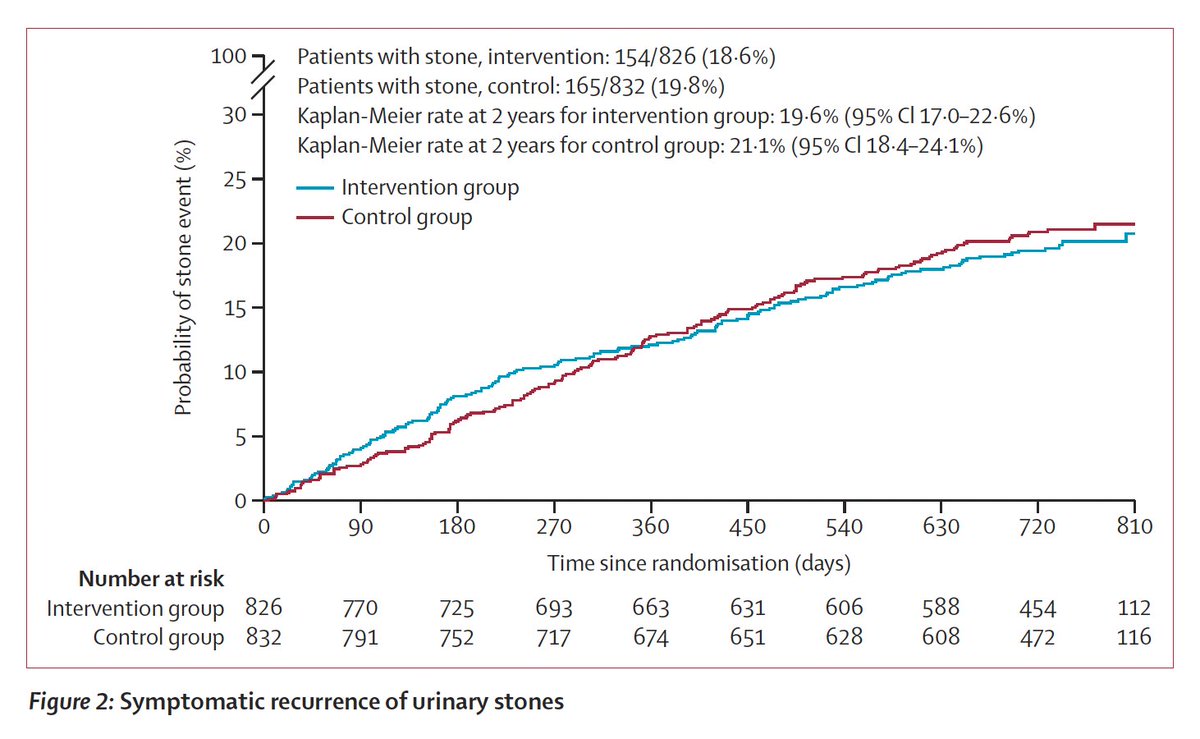
If you've had a kidney stone, you've been advised that the most important thing to prevent another bout is to increase hydration. Now a randomized trial of hydration in over 1600 participants showed no benefit, despite evidence of increase during volume. https://t.co/9ipUGlIsMz
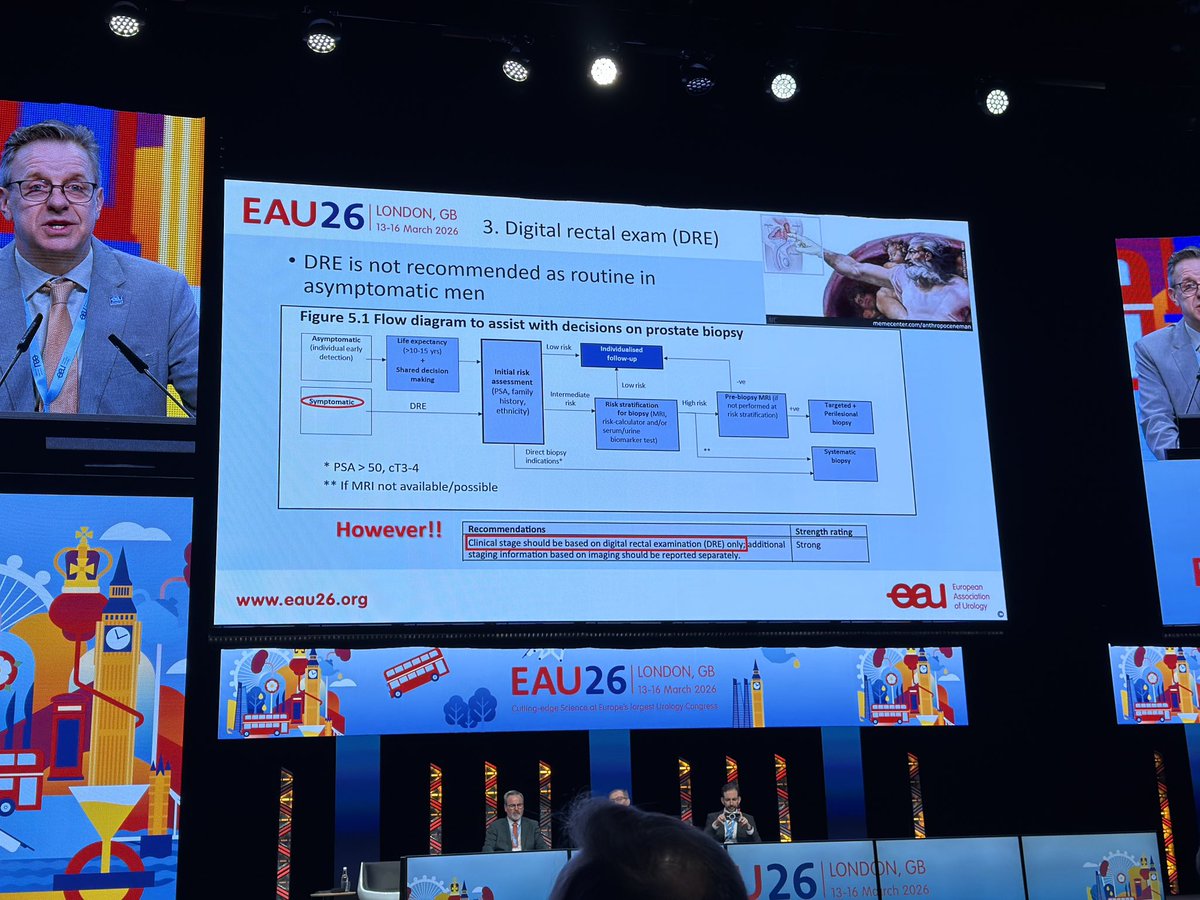
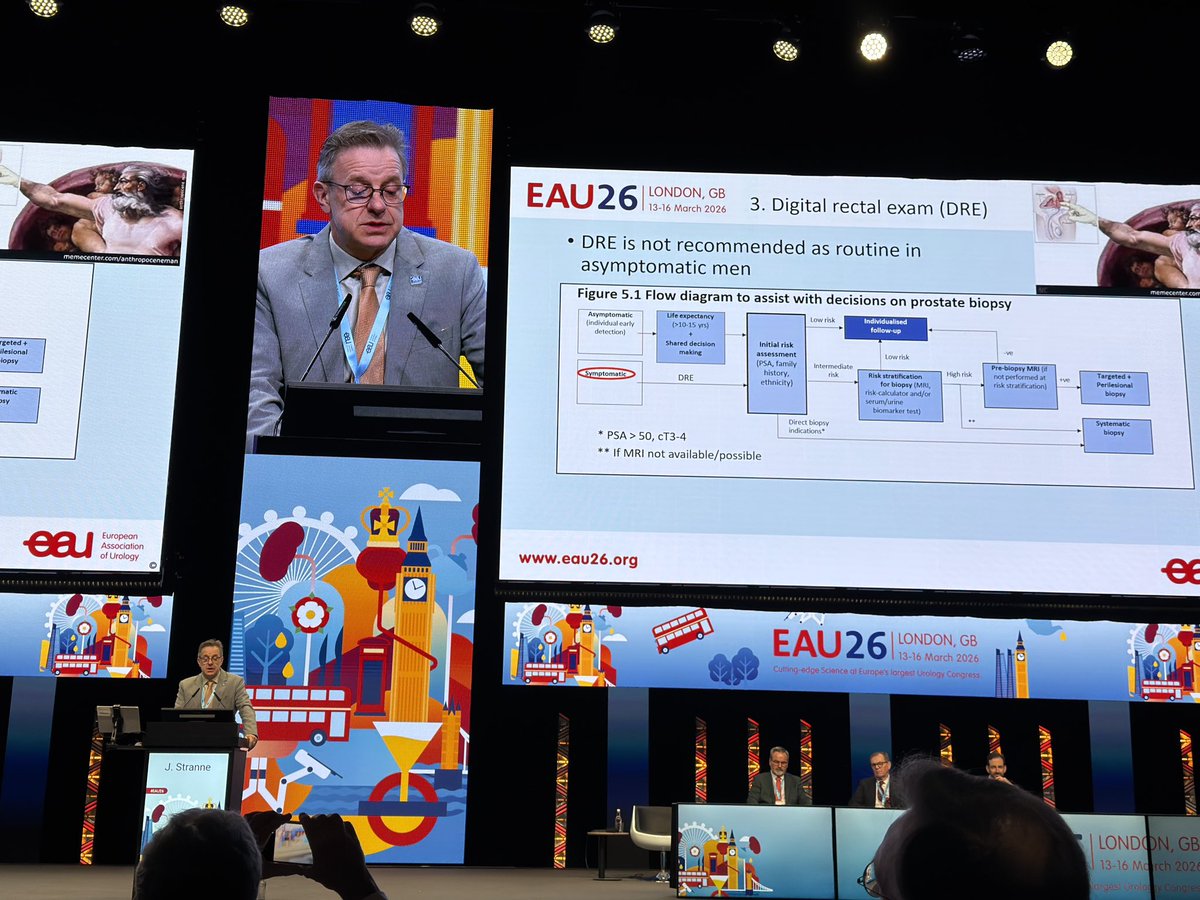
PRostate cancer guidelines 2026 update. Digital rectal exam NOW no more recommended for Asymptomatic men
SO NO MORE FOR Screening
Important for standing and for early diagnosis for SYMPTOMS only @Uroweb
Weighing risk and access: How to manage positive urinalysis in the #Urology clinic. Siobhán Hartigan, MD, URPS, FACS @HunterdonHealth joins @UroCancerMD@VUMCurology stressing the importance of separating asymptomatic bacteriuria from true UTI, especially for cystoscopy where inflammation can mimic cancer. She advocates risk‑stratifying by age, smoking history, and cancer risk, noting that almost half of patients whose cases are canceled never return. #WatchNow > https://t.co/IlYhHwbto3
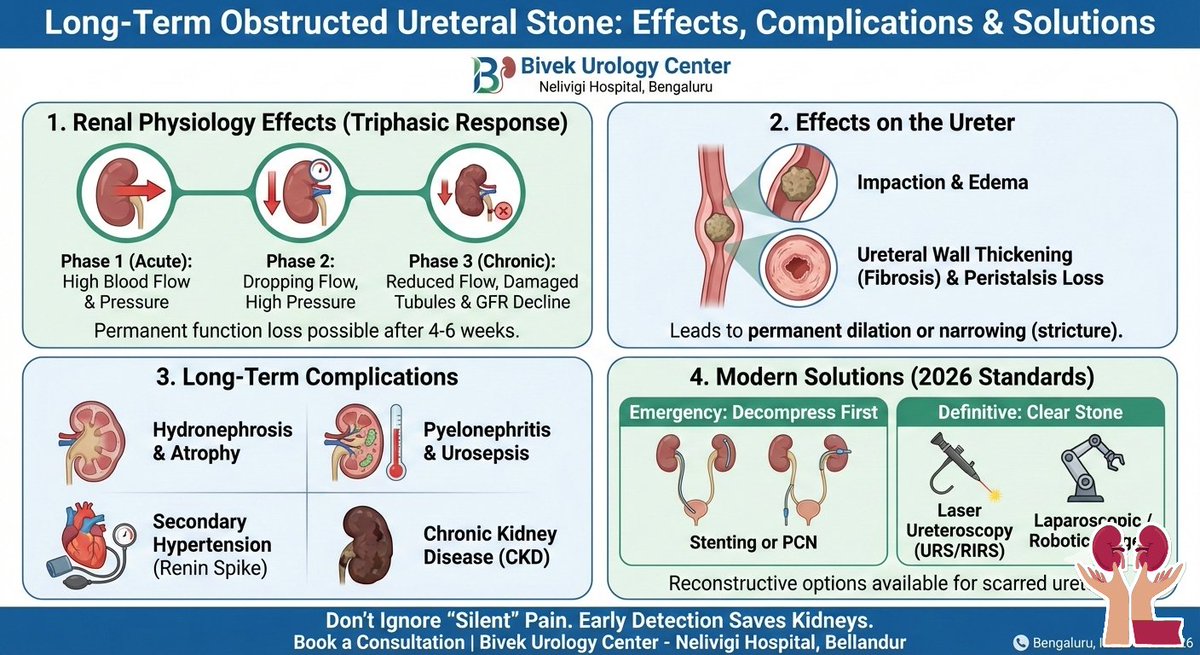
CHRONIC OBSTRUCTED URETER STONE
A long-term obstructed stone is often a "silent killer" of the kidney because once the initial sharp pain (renal colic) subsides, the patient may mistakenly believe the problem has resolved, while the kidney continues to deteriorate.
➡️Effects on Renal Physiology
When a stone blocks the ureter, the pressure behind it rises, triggering a "triphasic response" in the kidney:
🚩Phase 1 (Acute - First 1.5 hours): Renal blood flow increases as the body tries to "flush" the obstruction. Glomerular filtration pressure rises.
🚩Phase 2 (1.5–5 hours): Renal blood flow begins to drop while pressure in the renal pelvis stays high.
🚩Phase 3 (Chronic - After 5 hours): Renal blood flow significantly decreases. To protect the kidney from bursting, the body constricts the input of blood.
🚩Glomerular Filtration Rate (GFR) Collapse: Prolonged pressure causes the GFR to drop permanently. Even if the stone is removed later, the kidney may never return to 100\% function.
🚩Tubular Damage: The delicate tubules that concentrate urine begin to atrophy. This leads to an inability to balance electrolytes (sodium, potassium) and water.
➡️Effects on the Ureter
The ureter is not just a tube; it is a living, muscular organ. Long-term obstruction causes:
🎈Stone Impaction: The stone becomes "buried" in the ureteral wall as the surrounding tissue becomes inflamed and swollen (edema).
🎈Ureteral Wall Thickness (UWT): The muscle layer thickens to try and "pump" against the blockage, but eventually, this muscle is replaced by stiff scar tissue (fibrosis).
🎈Loss of Peristalsis: The rhythmic contractions that move urine are lost. This means even after the stone is gone, urine may not flow effectively, leading to "megaureter" or permanent dilation.
➡️Long-Term Complications
If the obstruction is left for more than 4–6 weeks, the damage often becomes irreversible:
🚩Hydronephrosis & Renal Atrophy: The kidney swells with trapped urine, thinning the actual functional tissue (the parenchyma) until the kidney becomes a useless "sac of fluid."
🚩Pyelonephritis & Urosepsis: Stagnant urine is a breeding ground for bacteria. This can lead to life-threatening blood infections.
🚩Secondary Hypertension: The damaged kidney releases excess renin, a hormone that spikes blood pressure, further damaging both kidneys and the heart.
🚩Chronic Kidney Disease (CKD): Permanent loss of nephrons leads to a lifelong decline in renal health.
➡️Modern Solutions (2026 Standards)
The approach today is twofold:
🎈Decompress first
🎈then Clear.
🚩Emergency ➡️Ureteral Stenting or PCN drain "pus or pressure" immediately.
🚩Definitive ➡️Laser Ureteroscopy (URS/RIRS) Using high-power lasers to "dust" the stone into sand.
🚩Complex ➡️Laparoscopic / Robotic Ureterolithotomy , For very large, old, or "impacted" stones that cannot be reached endoscopically.
🚩Reconstructive ➡️Ureteral Reimplantation / Boari Flap , If the ureter is too scarred or narrowed (stricture) from the long-term stone.
🍨Tip :
"If you had a stone pain that 'went away' without the stone actually passing, your kidney might be at risk.
A simple ultrasound or CT KUB can save your kidney function today."
Dr Bivek Kumar
Cisplatin-ineligible MIBC finally gets a perioperative breakthrough 🚨
This is not incremental. This is transformative.
KEYNOTE-905 / EV-303 | NEJM 2026 📘
Perioperative enfortumab vedotin + pembrolizumab around cystectomy vs surgery alone.
Study population 👥
Muscle-invasive bladder cancer
T2-T4a N0 or T1-T4a N1
Cisplatin-ineligible or declined cisplatin
ECOG 0-2
Older, frailer, real-world patients 🧓
Trial arms 🧪
🟦 Neoadjuvant EV + pembrolizumab (3 cycles) → cystectomy 🔪 → adjuvant EV + pembrolizumab
🟥 Radical cystectomy alone
Primary endpoint – Event-free survival 📉
2-yr EFS: 74.7% vs 39.4%
HR 0.40
P < 0.001
Overall survival 🌍
2-yr OS: 79.7% vs 63.1%
HR 0.50
P < 0.001
Pathological complete response 🧬
pCR: 57.1% vs 8.6%
Absolute gain ~48%
Safety signal ⚠️
Grade ≥3 AEs: 71% with EV-pembro
Expected EV toxicities dominate (skin, neuropathy) 🧴🦵
Surgery rates preserved. No compromise on cystectomy feasibility ✅
Clinical takeaway 🎯
For cisplatin-ineligible MIBC, perioperative EV + pembrolizumab sets a new benchmark
Survival gain ⬆️
Deep pathological responses 🔬
Practice-changing signal backed by OS 📊
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #BladderCancer #UroOnc
@myesmo@esmo_open@asco@OncoAlert