🫁 Chest tubes are far more than “just a drain.”
This review is an excellent reminder that successful pleural management depends on understanding physiology, imaging, drainage mechanics, and complications.
Several practical concepts stand out:
📡 Image guidance matters.
Ultrasound is now the standard for pleural drainage, improving success and reducing complications compared with blind insertion. CT guidance becomes essential for loculated, fissural, or complex collections.
📏 Bigger is not always better.
Small bore pigtail catheters are increasingly supported for many pleural effusions and pneumothoraces, often causing less pain and fewer complications. Large bore tubes still retain value in:
• hemothorax
• empyema
• persistent air leak
• mechanically ventilated pneumothorax
⚠️ One of the most misunderstood areas remains chest drainage systems.
The paper clearly explains: • tidaling
• bubbling interpretation
• water seal physiology
• suction management
• digital drainage systems
Importantly, continuous bubbling is not automatically “normal.” It may indicate a persistent air leak, tube malfunction, or incomplete pleural sealing.
Another excellent point: 🧠 excessive suction may sometimes prolong alveolar or bronchopleural fistula healing.
Finally, the review highlights serious complications clinicians must actively anticipate: • tube malposition
• arterial injury
• persistent air leak
• reexpansion pulmonary edema
Chest tube management is not a nursing afterthought. It is dynamic pleural physiology at the bedside.
📖 Ukeh I et al. Seminars in Interventional Radiology. 2022;39:234–247. https://t.co/fiVVLgt7CP
🍽️ ICU nutrition: we’ve been doing it wrong for years?
More calories
More protein
Earlier feeding
Sounds logical
But physiology disagrees
⚠️ The key update
High-quality RCTs now show:
❌ Early full-dose nutrition
→ NO benefit
→ Potential harm
Especially in:
• Shock
• Multiorgan failure
• High metabolic stress
👉 This is not neutral
👉 This is dangerous practice
🧠 Critical illness is not static
It evolves through metabolic phases:
1. Acute catabolic phase
2. Stabilization phase
3. Recovery phase
👉 Feeding must follow physiology
Not protocols
🔥 Phase 1: Acute catabolic
• High inflammation
• Insulin resistance
• Endogenous substrate mobilization
👉 The body is NOT ready for full nutrition
💡 Strategy:
✔️ Permissive underfeeding
✔️ Low protein
Why?
Because early overload leads to:
• Hyperglycemia
• Hepatic dysfunction
• Renal stress
• Impaired autophagy
👉 You are feeding dysfunction, not recovery
⚖️ Phase 2: Stabilization
• Inflammation decreasing
• Organ function improving
👉 Now metabolism starts to tolerate nutrition
💡 Strategy:
✔️ Slow escalation
✔️ Daily reassessment
⚠️ Red flags:
• Hypophosphatemia
• Hyperglycemia
→ Patient is NOT ready
💪 Phase 3: Recovery
• Anabolism returns
• Mobility improves
👉 NOW nutrition matters most
💡 Strategy:
✔️ Higher calories
✔️ Higher protein
✔️ Combine with rehab
👉 This is where you rebuild muscle and function
📊 The real takeaway
Nutrition is NOT:
❌ A fixed prescription
❌ A calorie target
It is:
✔️ A dynamic therapy
✔️ A metabolic intervention
🎯 The new principle
“Start low
Advance judiciously
Individualize throughout”
👉 Precision ICU nutrition
⚠️ Final thought
Overfeeding early harms
Underfeeding late harms
👉 Timing is everything
📚 Stoppe C et al. Curr Opin Clin Nutr Metab Care 2026
DOI: 10.1097/MCO.0000000000001186
@TJCoats@amirysh@RCEMevents It has a variable response as the t depends on if the FFP contains C1esterase inhibitors and kininase to breakdown bradykinins. But it is definitely worth a shot.
Team 2 u FFP and 1g TXA!
PAD reduzida no choque hemodinâmico é sempre sinônimo de vasoplegia? Nem sempre!
Entenda situações em que a PAD perde acurácia nessa associação.
Segue o fio 🧶
[1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
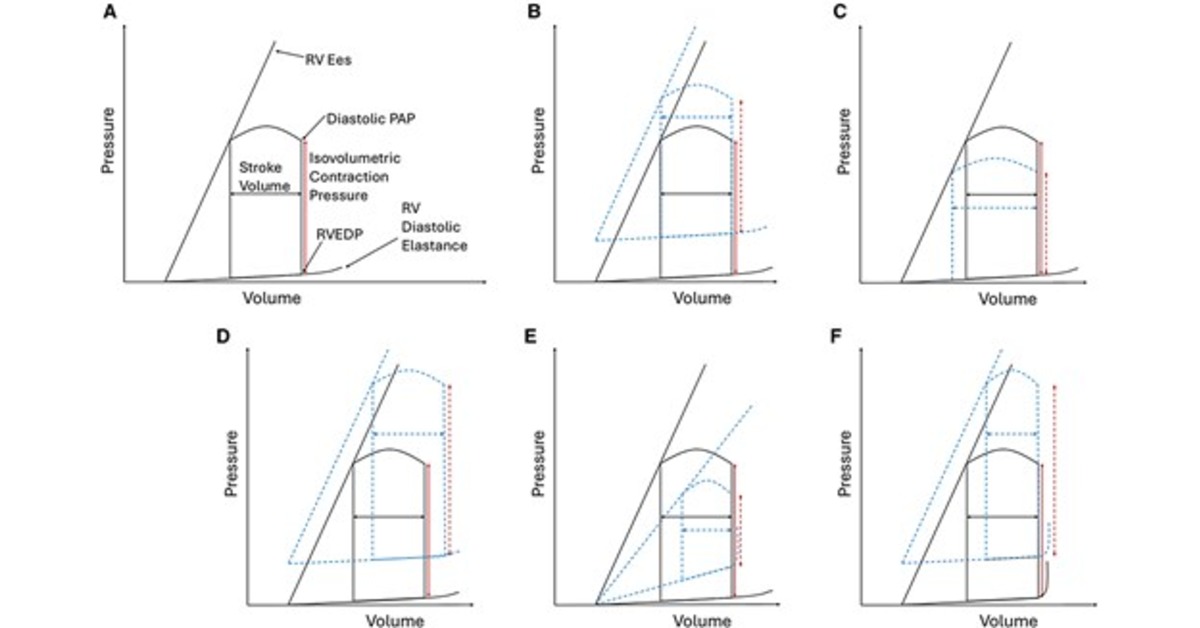
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 https://t.co/gri8ZaHHsI
Great schema!
But beware that *any* time you see a diagram like this, it assumes the patient has one disease process.
Our patients are increasingly multimorbid so:
⚠️May have >1 cause of hypoNa
⚠️Fixing one cause may cause dominant physiology to shift (playing wack-a-mol)
Peripheral vasopressor administration in critically ill adults was associated with a low incidence of adverse events—major events were rare using short peripheral intravenous catheters, and use avoided central venous catheter placement in 60% of cases.
https://t.co/wfpRZndlnl
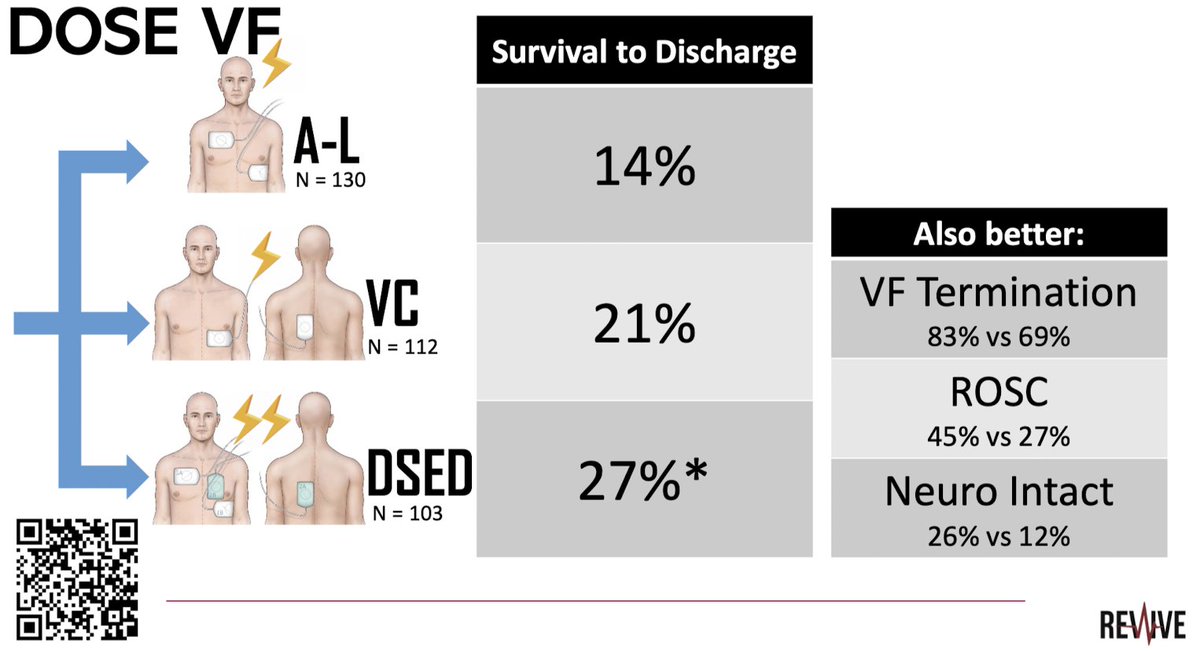
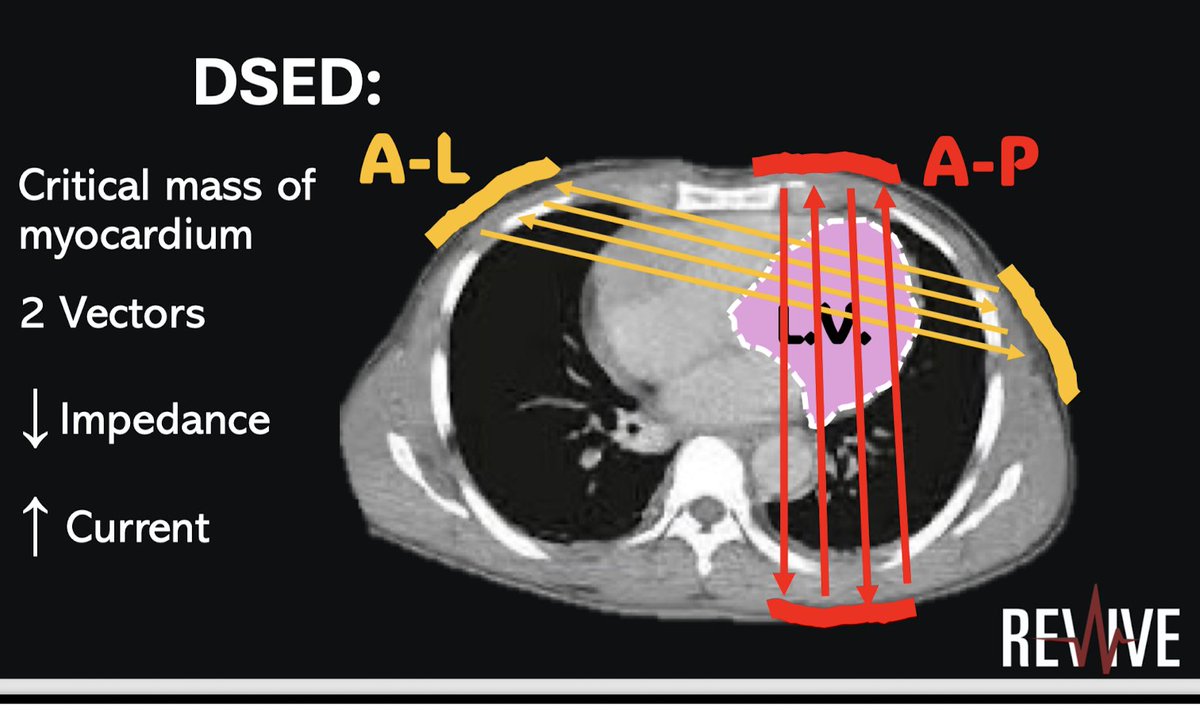
Defibrillation 2.0 by Dr. Corcoran #REVIVE2026
AP pad placement allows
🔺Better vector
🔺 Less impedence
Dual sequential external defibrillation (DSED)
AHA guidelines: Class 2b recom
ILCOR: DSED suggested strategy for VF refractory to shocks
@CardioNerds@OscarJMitchell
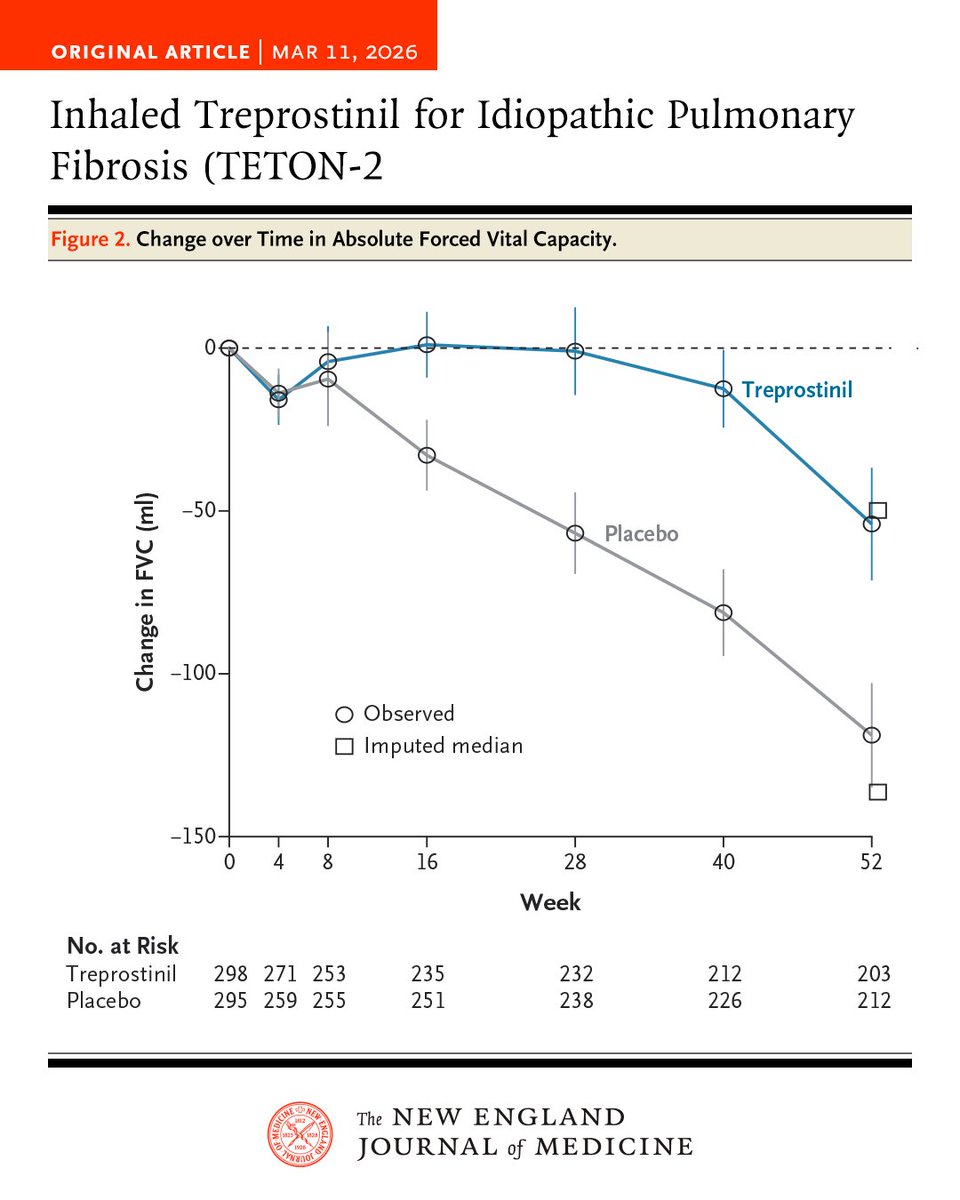
In the phase 3 TETON-2 trial involving patients with idiopathic pulmonary fibrosis, inhaled treprostinil was associated with a smaller decline in forced vital capacity and a lower risk of clinical worsening than placebo over 52 weeks. Full trial results: https://t.co/s2qlC2VAEd
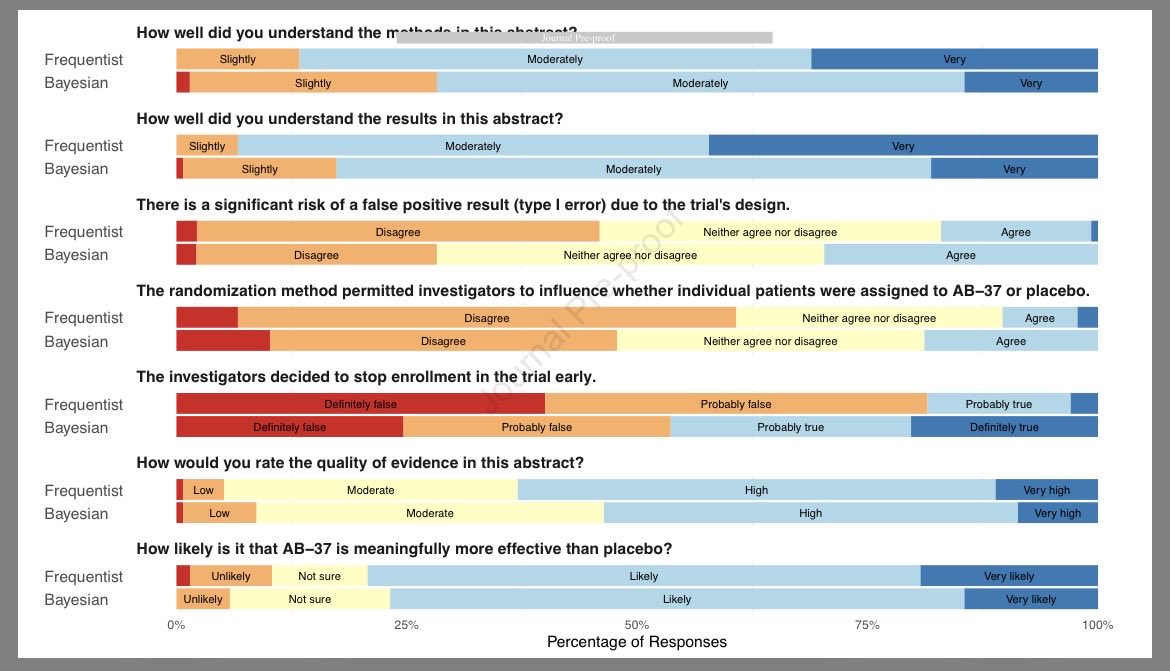
😵💫 Are you confused by Bayesian methods? Do you worry you’re alone? 🫢
Just in #journal_CHESTCritCare, B Malley et al eval how intensivists differently interpret results from Bayesian and frequentist trials…
https://t.co/nXpTmzJiKH
…I’m a bit unsettled by their findings 😉
Great to see this study in press where we show the utility of a sleep positioning device in managing GERD after lung transplant. Novel, safe and cost effective solution to a major problem in this population. Thankful to ACG for the research award! @ScottGabbardMD
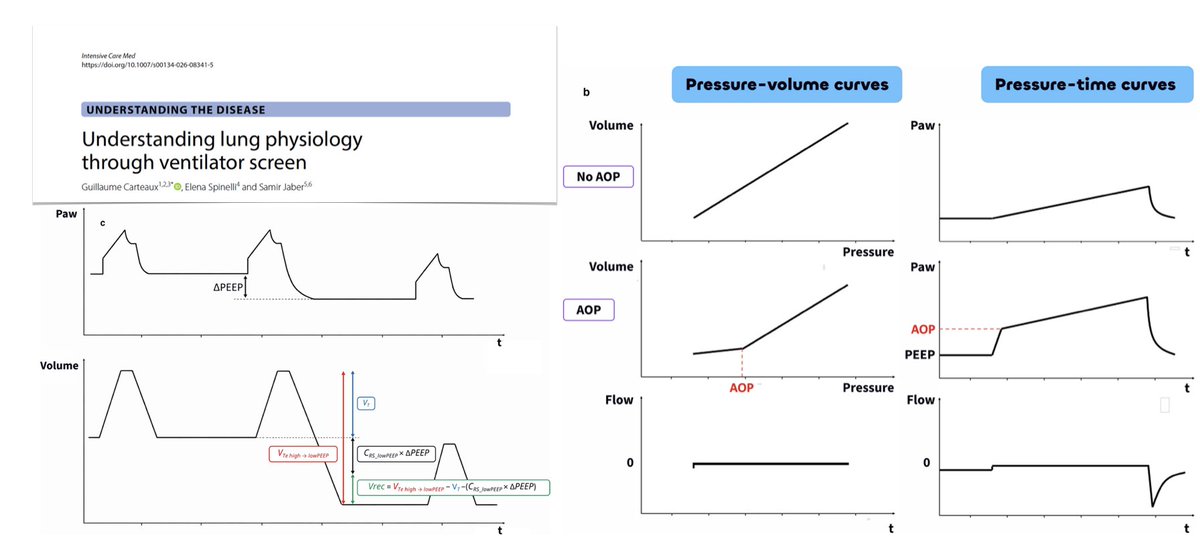
Understanding lung physiology through ventilator screen
🫁 airway pressure waveform at a glance: respiratory system equation of motion, conductive pressure, stress index, driving pressure
🌊 flow waveform during pressure-controlled ventilation
💨 expiratory flow and the time constant of the respiratory system
🛌 dynamic bedside maneuvers: airway opening pressure, recruitability & recruitment-to-inflation ratio
🚧 the way forward
#FOAMcc
🔓 https://t.co/TzWW9gtLOB
Right Ventricular Hemodynamics in Acute Respiratory Distress Syndrome: Monitoring and Implications for Clinical Management
@atscommunity
🔗 https://t.co/Pd3siasQuC
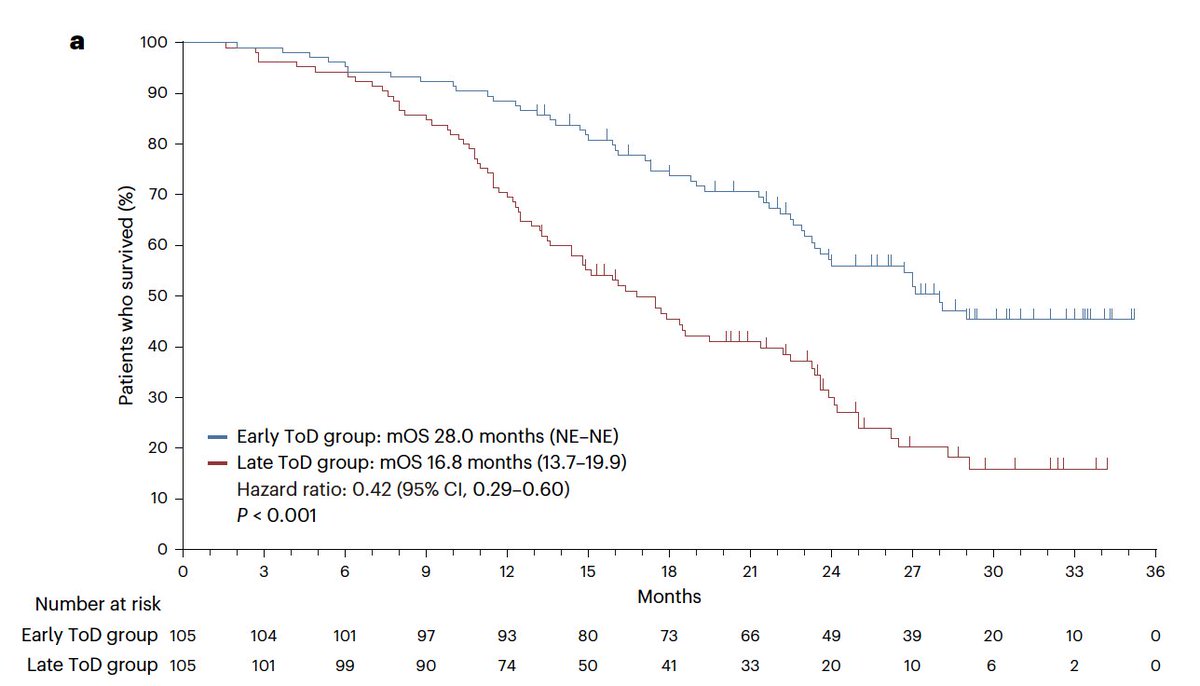
The time of day for cancer immunotherapy is associated with major outcomes. Early is better. Results from a randomized trial of lung cancer, backs up the importance of our circadian rhythm and immune system
https://t.co/bHqUZ3U83O
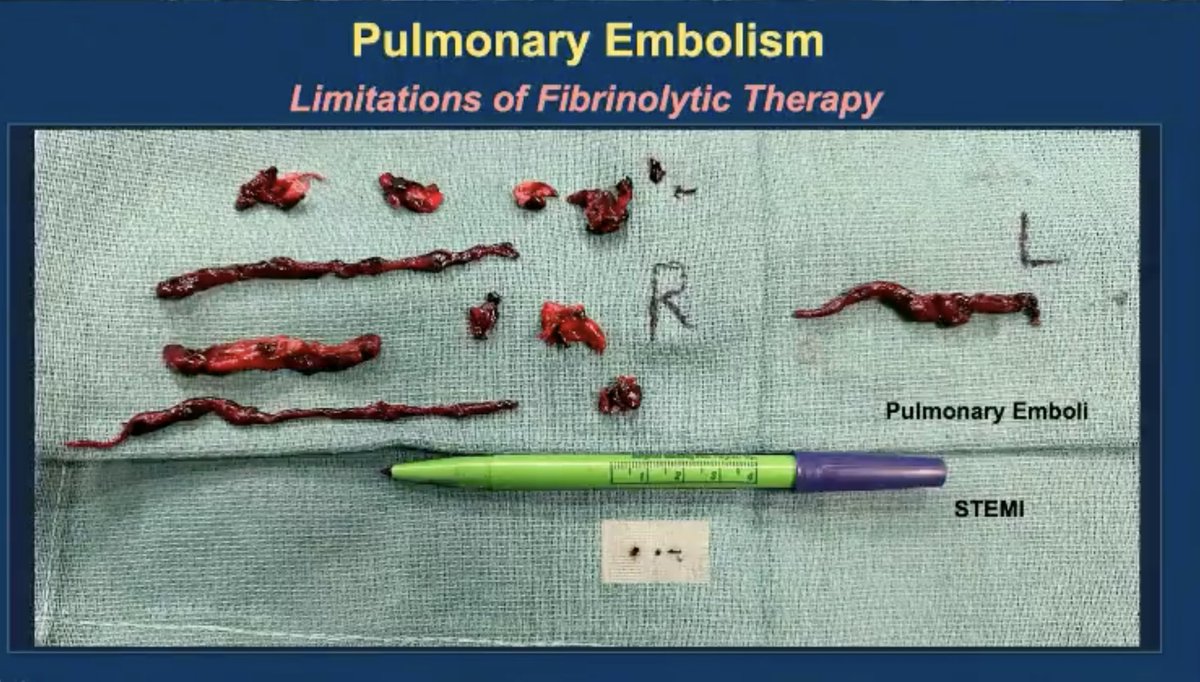
*Pulmonary embolism* versus *Acute myocardial infarction*:
Above and below the pen: the size of the clots in each scenario
I was looking for a picture like this and found it in a lecture by Dr Sripal Bangalore
#foamed#foamcc#meded#MedTwitter
Alveolar gas equation and its clinical implications
🧮 derivation & application of AGE
💨 fraction of inspired O2
💨 atmospheric pressure
🩸PaCO2 & respiratory exchange ratio
🫁 PAO2 & A–a gradient in the approach of hypoxemia & pulmonary shunt
#FOAMcc
🔓 https://t.co/LqmYQt1cht

































![FSotoMD's tweet photo. [1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24 https://t.co/uCviL2SL9n](https://pbs.twimg.com/media/Feq1bgWWYAEEcQs.jpg)