Excited to have one day, two posts on coronary artery diseases😄
🫀Our research on genomics of CAD was published in @NatureComms: An integrated germline and somatic genomic model for coronary artery disease
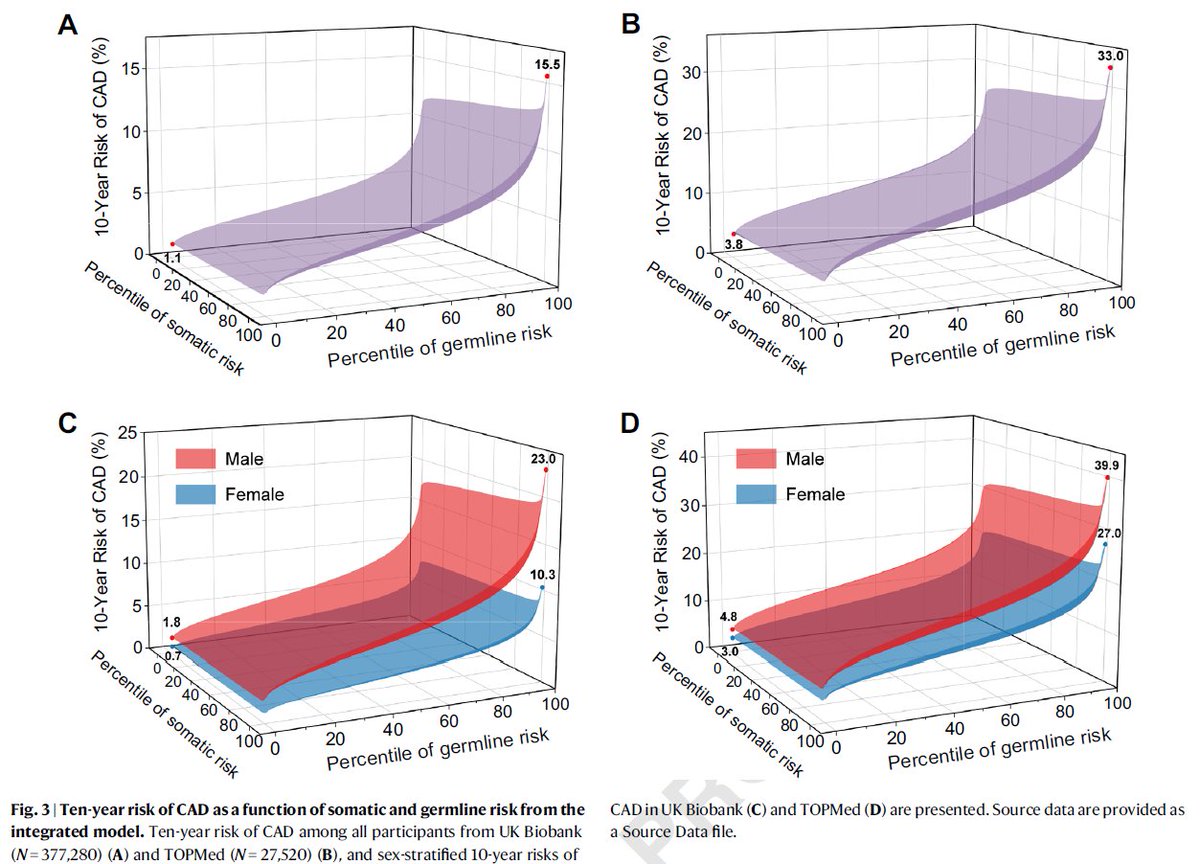
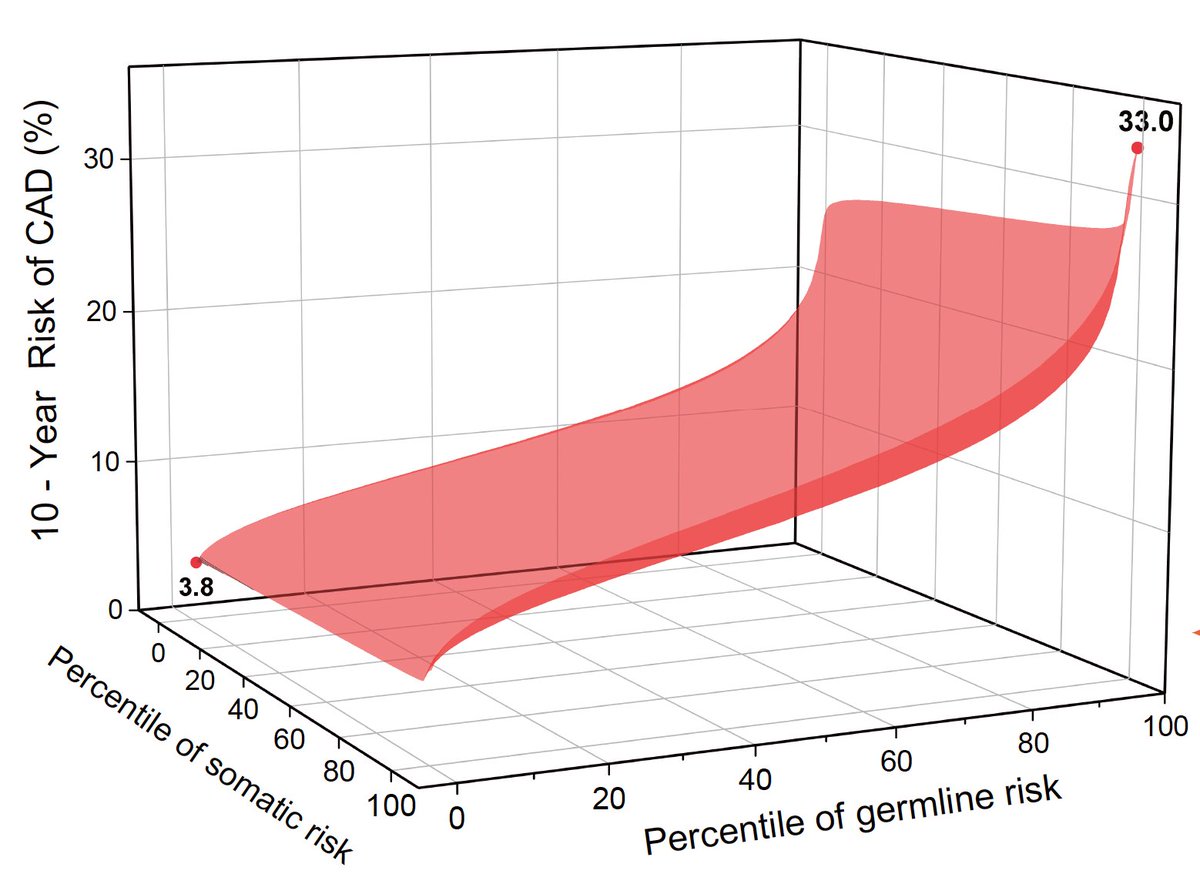
As genomic medicine moves closer to routine clinical use, mixed signals from different genetic tests risk confusing patients and clinicians alike. Our goal was to consolidate all available genomic information into a single, interpretable risk estimate, much like how clinical risk calculators integrate blood pressure, cholesterol, and diabetes into one clinically actionable estimate. We developed an integrated genomic model (IGM) that combines six germline and somatic genetic drivers of coronary artery disease (CAD) into a single risk estimate derived from one DNA sample.
Key takeaways:
1️⃣ With integrated genomic model, we identified about 13% of CAD high-risk individuals who would have been missed by polygenic risk score alone. These are people whose risk stems from combinations of familial hypercholesterolemia variants, clonal hematopoiesis, or shortened telomere length.
2️⃣ The IGM captures individuals at high risk who lack any single obvious high-risk genetic factor. Their elevated risk comes from the accumulation of multiple moderate genetic signals across different biological pathways. Conversely, some individuals carrying known high-risk variants (like FH variants) are protected by favorable profiles elsewhere in their genome.
3️⃣When combined with the clinical risk scores (PCE, the guideline-recommended clinical calculator), the IGM provided the strongest risk stratification, reclassifying individuals across every clinical risk category.
This work would not have been possible without the @broadinstitute, @MGBResearchNews, @MassGenBrigham , and the @CAS__Science. I am grateful to have co-led this project with Xiong Yang, guided by the exceptional mentorship of @pnatarajanmd, @MinxianWang, and @aklfahed. Special thanks to @hongheeW, @patrick_ellinor, @NakaoTetsushi, @somijemmacho, @skoyamamd (to mention few), and the entire NHLBI TOPMed Consortium for their contributions.
New from our group published in @NatureComms
https://t.co/RfGy7oWGty
What is the maximal information you can get from a single DNA sample to predict heart attack risk?
We developed an integrated genomic model that combines germline (polygenic risk scores, monogenic variants) and somatic (CHIP, LTL) information.
Risk is demonstrated as a gradient on a 2D envelope capturing germline and somatic risk.
We identify ~ 13% of high-risk individuals who would have been missed by polygenic risk score alone.
Wonderful collaboration co-led with @pnatarajanmd and @wallacemwang
Thread form postdoc extraordinaire and co-first author @MinSeoKim_MD in comments
@MGBResearchNews@broadinstitute
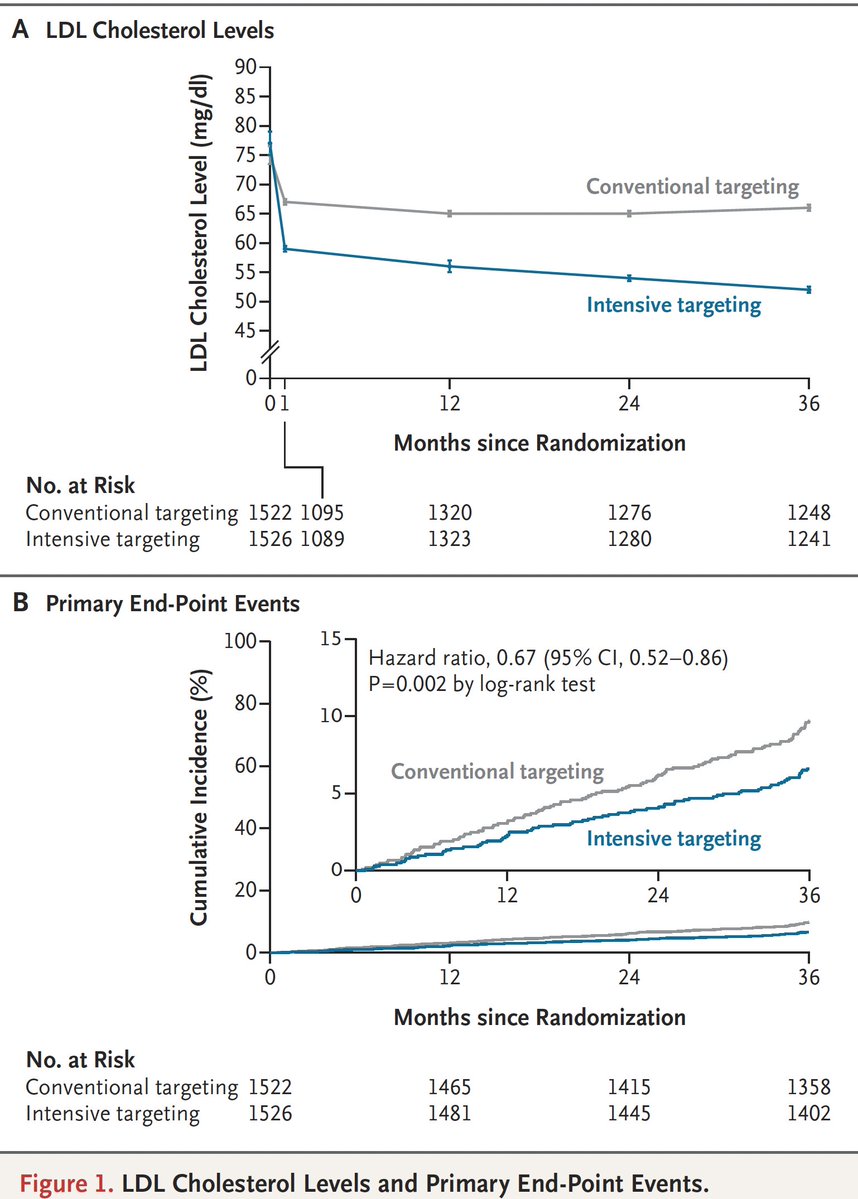
Validation of aggressive LDL lowering to reduce major adverse cardiovascular events, a randomized trial targeting LDL < 55 mg/dl. In participants with atherosclerotic cardiovascular disease (secondary prevention)
@NEJM #ACC26
https://t.co/oLnkqhawOd
HARP study is out at #ACC26 with simultaneous publication @CircAHA
OCT + Cardiac MRI identified diagnosis in 79% or MINOCA patients
Some examples from our participants below — intraplaque hemorrhage and plaque rupture that would otherwise be missed on coronary angiography
Congrats to Harmony Reynolds who led this effort over several years
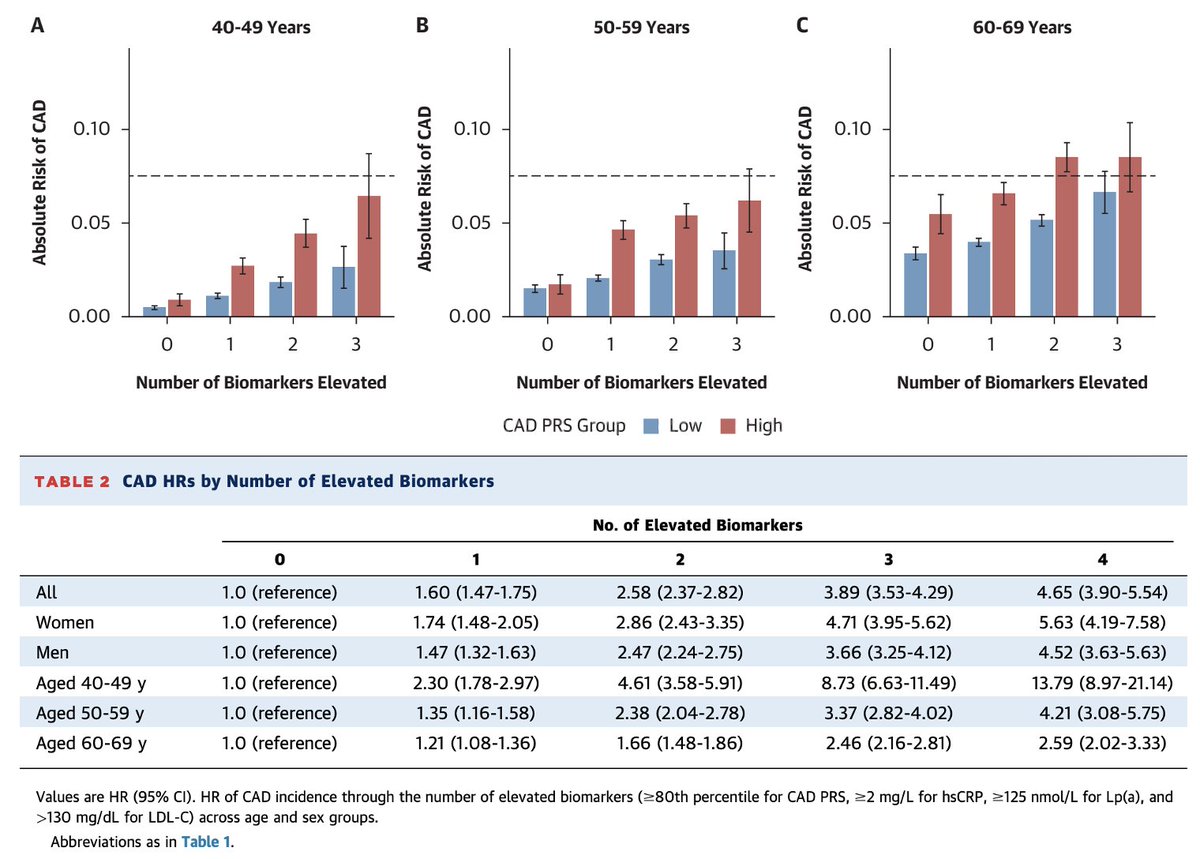
A combination of 4 biomarkers
👉polygenic risk score
👉LDL-C
👉Lp(a)
👉hsCRP
shows high predictive performance for incidence of coronary artery disease, especially in younger individuals.
Deep dive from @TCTMD_Caitlin about our recent paper and the concept of biomarker measurement to predict future cardiovascular disease, inform mechanisms that could be targeted, and potentially prioritize people for imaging.
Appreciate the insights also from @SumeetKhetarpal
Wonderful editorial from @iftikhar_kullo about our recent paper in @JACCJournals
From Risk Factors to Pathways: A New Framework for Coronary Heart Disease Prevention
"“Reducing the burden of CHD requires moving beyond risk prediction approaches developed more than 6 decades ago toward contemporary methods that leverage our understanding of disease biology.”
https://t.co/WMr24nrFxv
A one-time midlife assessment of four blood-based biomarkers—CAD polygenic risk score (PRS), hsCRP, LDL-C, and lipoprotein(a)—robustly predicts future coronary artery disease risk in both men and women aged 40 to 69 years.
A one-time midlife biomarker panel may unmask hidden future CAD risk long before conventional calculators do.
🔹 Pearl 1 — Four pathways, one practical panel
A single midlife assessment of CAD polygenic risk score (PRS), LDL-C, lipoprotein(a), and hsCRP captures genetic, lipid, and inflammatory risk, offering a more integrated view of future coronary artery disease risk.
🔹 Pearl 2 — Each biomarker independently predicts incident CAD
Over 12 years of follow-up, elevation of each biomarker was independently associated with higher CAD risk. The hazard ratios were 1.79 for CAD PRS, 1.60 for LDL-C, 1.20 for Lp(a), and 1.64 for hsCRP, confirming that all four add meaningful prognostic information.
🔹 Pearl 3 — Risk is multiplicative, not merely additive
Individuals with all four biomarkers elevated had a 4.65-fold higher risk of future CAD compared with those with no elevated biomarkers, highlighting the importance of cumulative burden across pathways.
🔹 Pearl 4 — Younger adults may benefit the most
All four biomarkers showed stronger associations at younger ages, suggesting that biomarker-based screening may be especially valuable in early midlife, when traditional clinical calculators often underestimate lifetime vascular risk.
🔹 Pearl 5 — Biomarkers can rival traditional risk calculators
The combined 4-biomarker model achieved a C-statistic of 0.753, which was slightly better than the pooled cohort equations at 0.740, indicating comparable or better discriminatory performance.
🔹 Pearl 6 — Better reclassification means fewer missed patients
Compared with pooled cohort equations, the 4-biomarker strategy produced a 32% continuous net reclassification improvement, suggesting it may identify at-risk individuals who would otherwise be missed by conventional clinical scoring.
🔹 Pearl 7 — CAD PRS appears particularly informative in men
The association of CAD PRS with incident CAD was stronger in men than in women, although the 4-biomarker model was predictive in both sexes.
🔹 Pearl 8 — Lp(a) still matters even when effect size is modest
Although the hazard ratio for Lp(a) was lower than for the other markers, it remained an independent predictor of CAD, reinforcing the value of at least once-in-a-lifetime Lp(a) testing in risk stratification.
🔹 Pearl 9 — hsCRP keeps inflammation in the CAD conversation
The strong association of hsCRP with future CAD supports the concept that residual inflammatory risk deserves attention alongside cholesterol and inherited risk.
🔹 Pearl 10 — Think beyond 10-year risk; think lifetime vascular exposure
This study supports interpreting CAD risk as a cumulative lifetime burden of inherited susceptibility, atherogenic lipids, and inflammation, which may help clinicians prioritize earlier and more targeted primary prevention.
Practical CME INDIA Take-Home Message
In adults aged 40–69 years, a one-time 4-marker panel of CAD PRS, LDL-C, Lp(a), and hsCRP may refine CAD risk assessment beyond traditional calculators, especially in younger individuals and those who appear low-risk by routine clinical scoring. This approach may help clinicians identify candidates for earlier lifestyle intensification, lipid lowering, closer follow-up, and personalized prevention strategies.
One-Line Conclusion
Midlife CAD prevention may become smarter when we measure inherited risk, cholesterol burden, lipoprotein(a), and inflammation together—not separately.
https://t.co/JQklhg9XeG
New from @rayshafarah in our group published in @JACCJournals
🔸 A single measurement of 4 blood-based biomarkers in midlife, namely CAD PRS, hsCRP, LDL-C, and Lp(a), is strongly predictive of future CAD incidence in both sexes and across the age spectrum from 40 to 69 years
🔸 A biomarker-based prediction model achieves comparable performance with clinical risk calculators and may identify populations who are not detected using a traditional clinical risk calculator, creating an opportunity for improved primary prevention, particularly in younger age groups, where the performance of biomarker-based screening is highest.
🔸 Interpreting risk as a cumulative burden of genetic, lipid, and inflammatory pathways provides a straightforward approach to prioritizing earlier, targeted primary prevention.
Article: https://t.co/uSeeARZNKh
Builds on prior work form Paul Ridker et al in @NEJM last year https://t.co/nHYgbxcBuC
going from 3 to 4 biomarkers by adding genetics
@MinSeoKim_MD@buutruong11@YangSui@somijemmacho@AniruddhPatelMD@pnatarajanmd@MGBResearchNews@broadinstitute
A single measurement of four biomarkers (CAD PRS, LDL-C, Lp(a), and hs-CRP) in middle age improves ASCVD risk prediction
Presented by @harvardmed student in the lab @rayshafarah#AHA25
https://t.co/76aiPpRYz2