Proud to share Appraiseye’s seminal publication in the Journal of Neurosurgery 🚀
Our AI vision stack quantified what happens between cases; itemizing OR turnover into discrete subprocesses.
Result: instrument burden is the main contributor to turnover duration ⏱️
Across 53 turnovers (cranial, spine, ENT):
• Setup time explained most variability
• Each additional tray added ~2.7 minutes
• Tray count—not individual surgeon nor assigned OR— best predicted turnover
Tray rationalization = faster turnover + lower costs
https://t.co/vnXpZvSFWd
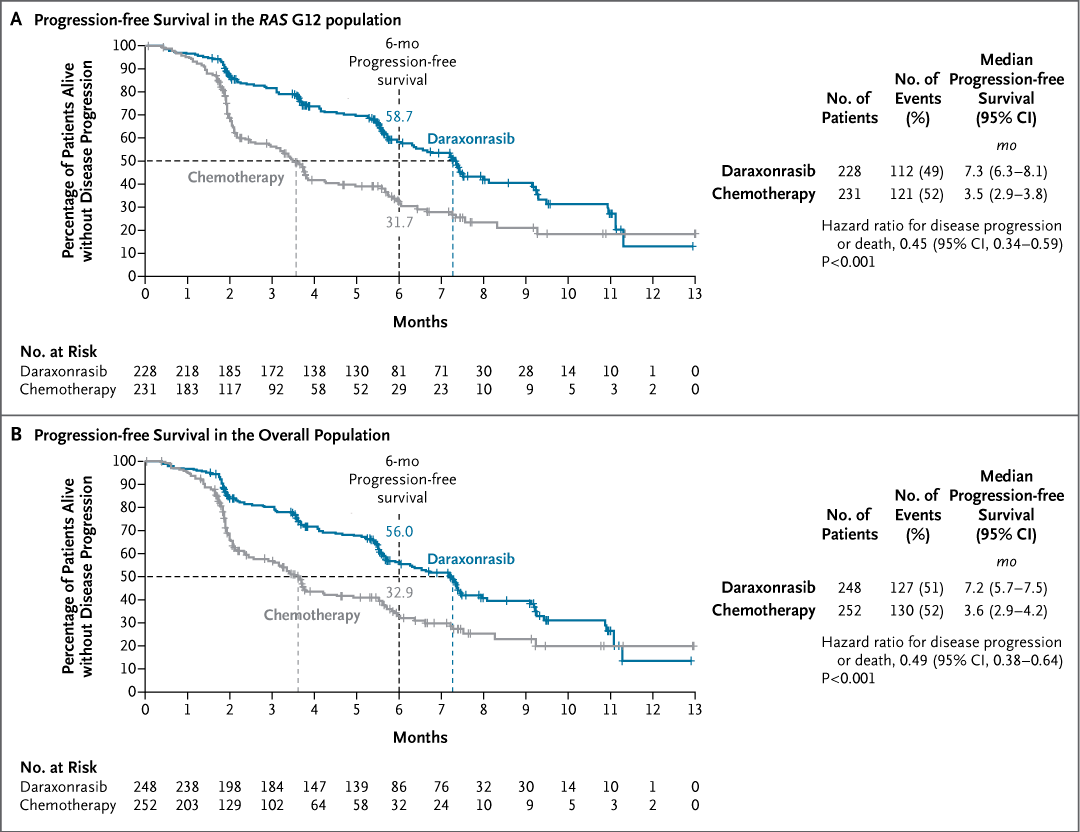
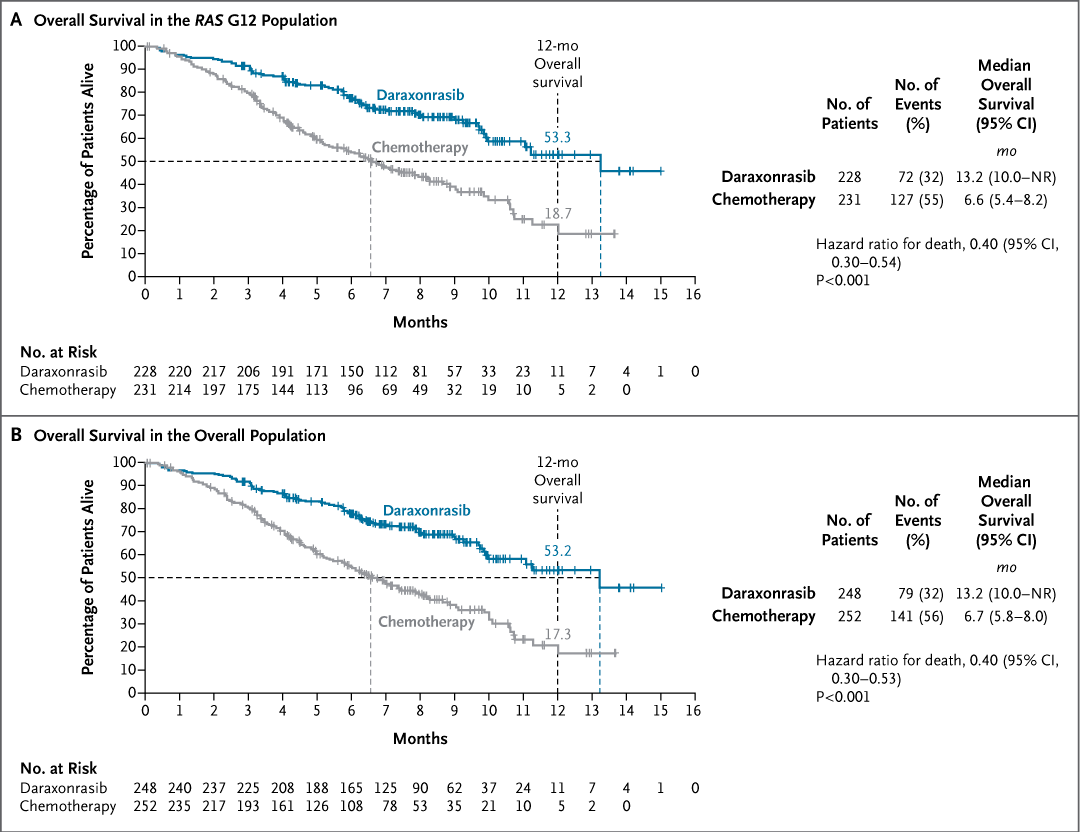
Original Article: Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer (phase 3 RASolute 302 trial) https://t.co/y4G27hfORg
#ASCO26 | @ASCO
Our new @NatureMedicine Perspective argues that uncritical use of #AI in early medical training may weaken independent clinical reasoning, and proposes a framework for integrating AI while protecting core competencies.
https://t.co/vAriiUhOk4
@NaturePortfolio@dukenus#DukeNUS
Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart.
Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient.
Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them.
Patient data is never stored after the clinical session or used for any other purpose.
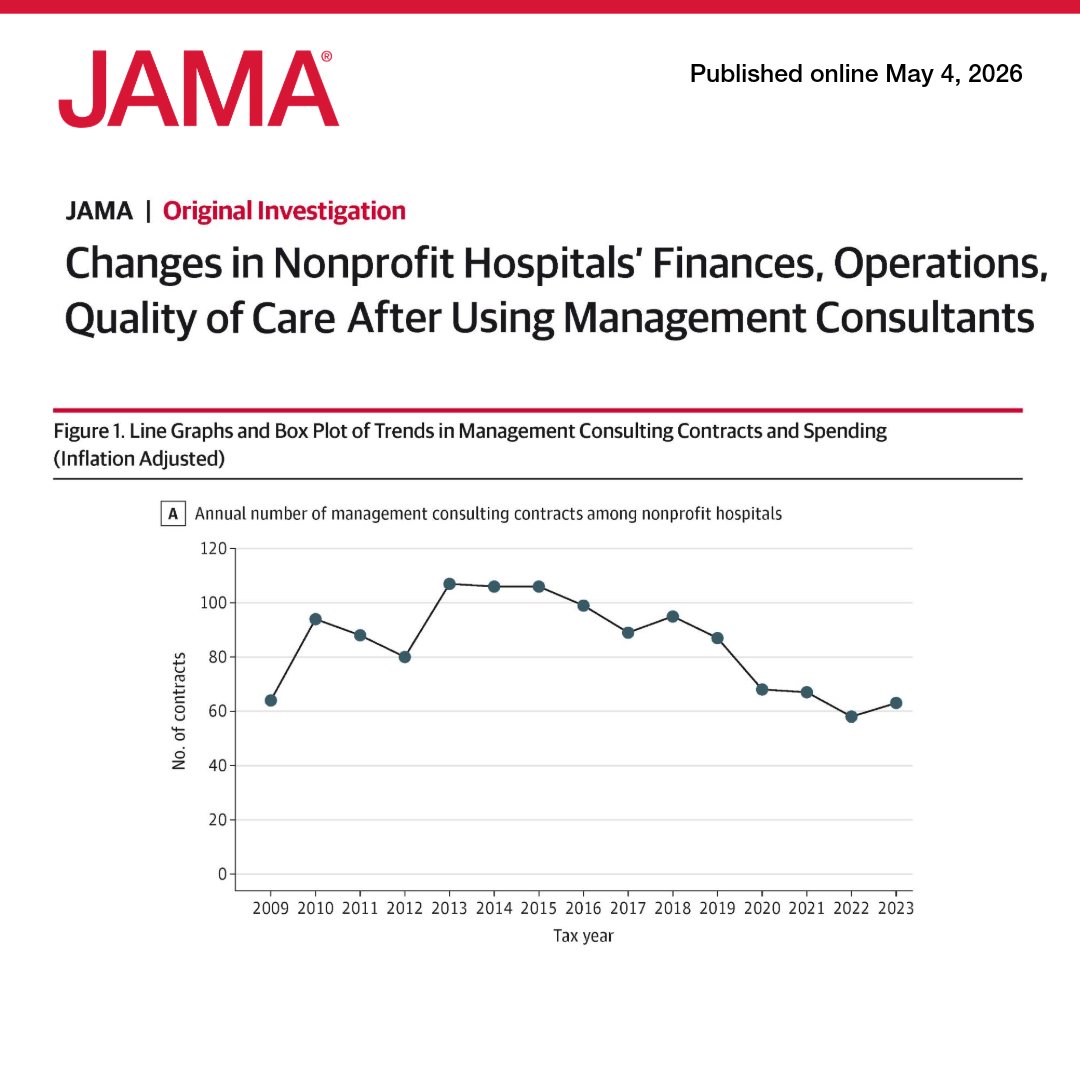
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
https://t.co/QQswMYxrG8
"Hospitals cost $1 to $2 million per bed to build. A single hospital can routinely exceed $1-2 billion. Their floor plans are rigid, fixed for decades. AI is about to make those floor plans obsolete."
Having now been on the front line of clinical care delivery, designing hospitals and building agentic AI infrastructure -- the collision is hard to ignore. We're spending $70B a year on hospitals with designs that may be obsolete before construction is done.
https://t.co/67i7YAspvP
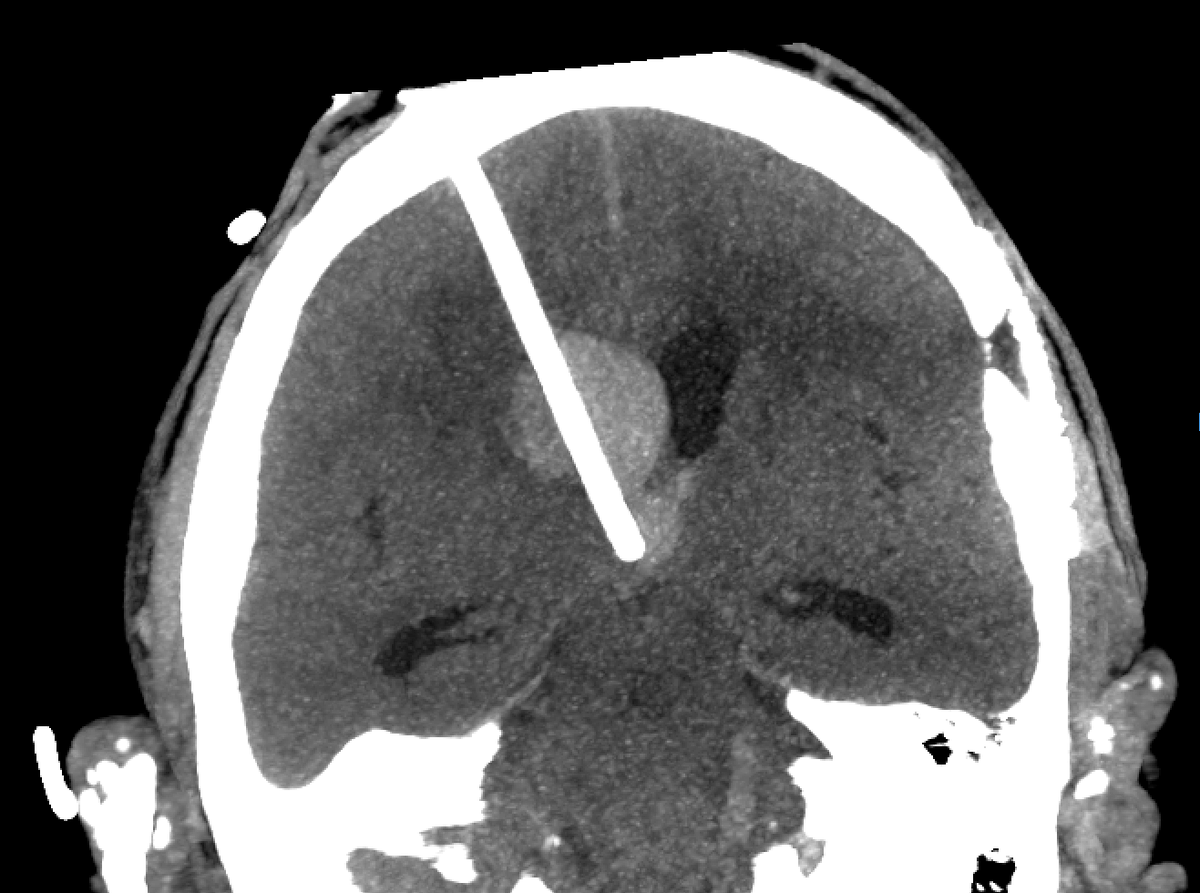
We're proud to announce a significant step forward in neurosurgical care. Dr. @RandyDAmico_MD has performed the first catheter placement navigated with Medivis' Cranial Navigation platform. It's a first that matters — intracerebral hemorrhage is one of the most time-sensitive and high-stakes conditions in neurosurgery, and precision is everything.
Post-op imaging confirmed accurate IRRAflow placement within the target hematoma, facilitating efficient clot evacuation.
Medivis' AR-guided platform delivers immersive, real-time anatomical visualization directly to the bedside and OR — giving surgeons the precision and confidence to navigate complex anatomy with clarity.
Dr. D'Amico's work exemplifies what's possible at the intersection of cutting-edge technology and surgical expertise.
Precision. Confidence. Better outcomes.
This is what the future of neurosurgery looks like. Congratulations to Dr. D’Amico and the entire team!
𝐒𝐥𝐨𝐩 𝐇𝐞𝐚𝐥𝐭𝐡𝐜𝐚𝐫𝐞 𝐈𝐬 𝐂𝐨𝐦𝐢𝐧𝐠
As a doctor/ tech start-up founder, I think I'm in a very good position to say the following:
- AI tools give true experts incredible leverage and turbocharges them.
- AI tools give novices incredible leverage and causes tremendous harm.
When my team and I at FutureClinic use AI coding tools, those who have enough expertise to correct the AI when it inevitably makes subtle or major mistakes are able to do work that would've taken them a year in 2 weeks.
But those who vibecode and don't have the expertise to NOTICE and CORRECT these mistakes produce huge volumes of dangerous code. Code that LOOKS plausible, but introduces security vulnerabilities that could end a company, or that introduces poor performance with cascading effects on the rest of the codebase.
When you apply that to healthcare, you start realizing how shallow and naive most of the analysis we see on the timelines is these days.
AI will make plausible-sounding healthcare advice abundantly available. Slop healthare. But when it comes to something as high stakes as the health of you and your family, is 'plausible-sounding' what you're looking for?
This is why tech companies are paying an absolute premium for TRUE experts as the 'guardians' of what AI-generated code actually gets merged into the codebase.
And why people will continue to rely on human doctors for anything beyond the lowest stakes 'health optimization' advice for years to come.
(FYI, I don't mind if your "AI Doctor" tells you to eat healthy and exercise, or helps the worried well analyze a few years of their Whoop data.)
Rory McIlroy commissioned this pencil drawing after last year's Masters Tournament.
The artist (@KeeganHall) provided context on Reddit:
• Spent 6+ months working on it
• Estimates 600-800+ total hours
• Worked on it 6-7 days each week
• Uses a Pentel Graphgear mechanical pencil
Hall says this piece was incredibly challenging because so much detail went into such a small area. For context, the original is smaller than 30x22, so each face in the crowd is essentially a quarter of the size of a fingernail.
This is the second piece he has done for Rory.
#AI scribe adoption across 5 academic centers was associated with modest reductions in EHR and documentation time, plus a slight increase in weekly visit volume, especially for primary care and female clinicians.
https://t.co/S2TNIOmhyO
@Rainmaker1973 CAR-T cells for solid tumors are coming. We need to make them scalable and identify the right target, but as in leukemias and lymphomas CAR-Ts can be a game changer. You gotta love the immune system!
Doctors in large centers don't realize what a life-changer fast operating room turnover times are.
For those that don't know, the turnover time in OR's varies widely between hospitals. That's the time it takes to clean the room and set up for the next case.
In efficient hospitals, especially those that are physician owned, it can be as quick as 20 minutes. In large academic hospitals, it can push 4 or even 5 hours.
Think of the difference that makes for quality of life, patient care, and revenue.
A doctor who has a large waitlist of patients might be at the hospital until 8pm and still only get two surgeries done because the turnover time is so long. That same doctor could get 3 or 4 surgeries done in a more efficient hospital, getting home in time to have dinner with his family.
A physician owned hospital would never tolerate a 4 hour turnover time. That's money being lit on fire. Yet hospitals tolerate this all the time because they don't face competition. There's no incentive to run efficient.
So the patients have to wait longer for their surgery, the doctors get frustrated, and everybody loses.
🚀 LabOS is now inside LabClaw! We embedded LabOS AI-XR co-scientist directly into LabClaw with OpenClaw —with unified skill layer for biomedical AI agents and world models. No more separate systems. One install. Full Wet-lab + Dry-lab execution with XR.
🔗 https://t.co/uWYgehXUxW
#LabClaw #Claw #LabOS #OpenClaw #AIforScience #Stanford #Princeton
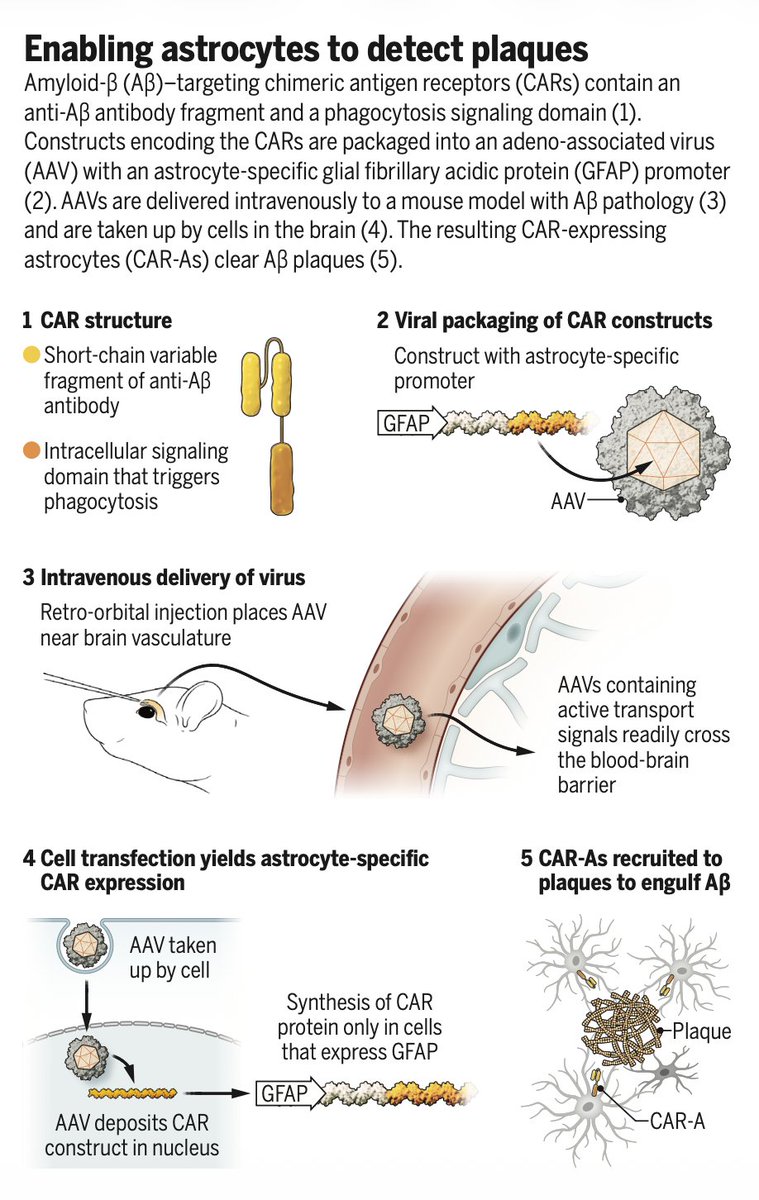
New @ScienceMagazine
Engineering the brain's astrocytes to clear amyloid plaque!
"CAR-A," in mouse model
https://t.co/u9zJGnCLUj
https://t.co/eIrrFx7iTg
Backed by Innovate UK, our CSO Huiling Ke met with Nikon HQ in Tokyo to explore a collaboration in next-generation vision and imaging technologies.
Inspired and looking forward to what we can build together.
Welcome to the Lab of the Future! 🧬🤖
Excited to share LUMI-lab, out today in @CellCellPress — a self-driving platform that pairs an AI foundation model with a robotic lab to autonomously discover ionizable lipids (LNPs) for mRNA delivery.
The core problem: Designing lipid nanoparticles (LNPs) is hard. The chemical space of ionizable lipids is vast, experimental cycles are slow, and — critically — historical LNP datasets are far too small to train a predictive model from scratch. Most AI approaches in this space hit a wall immediately: not enough data to learn from.
Our solution: lab-in-the-loop foundation model learning. Instead of training on LNP data alone, LUMI starts as a transformer-based foundation model pretrained across broad chemical space, building rich molecular representations before it ever sees a single LNP experiment. Then it enters a closed loop with a robotic synthesis platform: predict → synthesize → assay → update. Each round of real wet-lab experiments fine-tunes the model, which then proposes smarter candidates for the next round. The lab isn't just validating AI predictions — it's actively teaching the model, continuously.
What happened when we let it run: LUMI-lab autonomously synthesized and screened 1,700+ ionizable lipids in human bronchial epithelial cells. The top candidate — LUMI-6 — features a brominated lipid tail, a structural motif that had been largely overlooked in LNP design. LUMI found it without being told where to look. When formulated into LNPs and delivered intratracheally to mice, LUMI-6 achieved 20.3% gene editing efficiency in lung epithelial cells — a compelling result for one of the hardest-to-reach therapeutic targets, directly relevant to diseases like cystic fibrosis and alpha-1 antitrypsin deficiency.
Why this matters beyond LNPs: This is a proof of concept for a broader thesis — that foundation model pretraining + active learning + robotic experimentation can overcome the data scarcity bottleneck that plagues AI-driven discovery in biology. You don't need a massive domain-specific dataset to start. You need a model that can generalize, a lab that can generate the right data, and a loop that connects them.
Huge congratulations to first authors Yue Xu, @HAOTIANCUI1, and Kuan Pang, and to the entire @BowenLi_Lab team. Grateful to our collaborators at @UHN and @UofTPharmacy, and to Princess Margaret Cancer Centre Research @PMResearch_UHN.
📄 Paper: https://t.co/5tfD3dkSr7