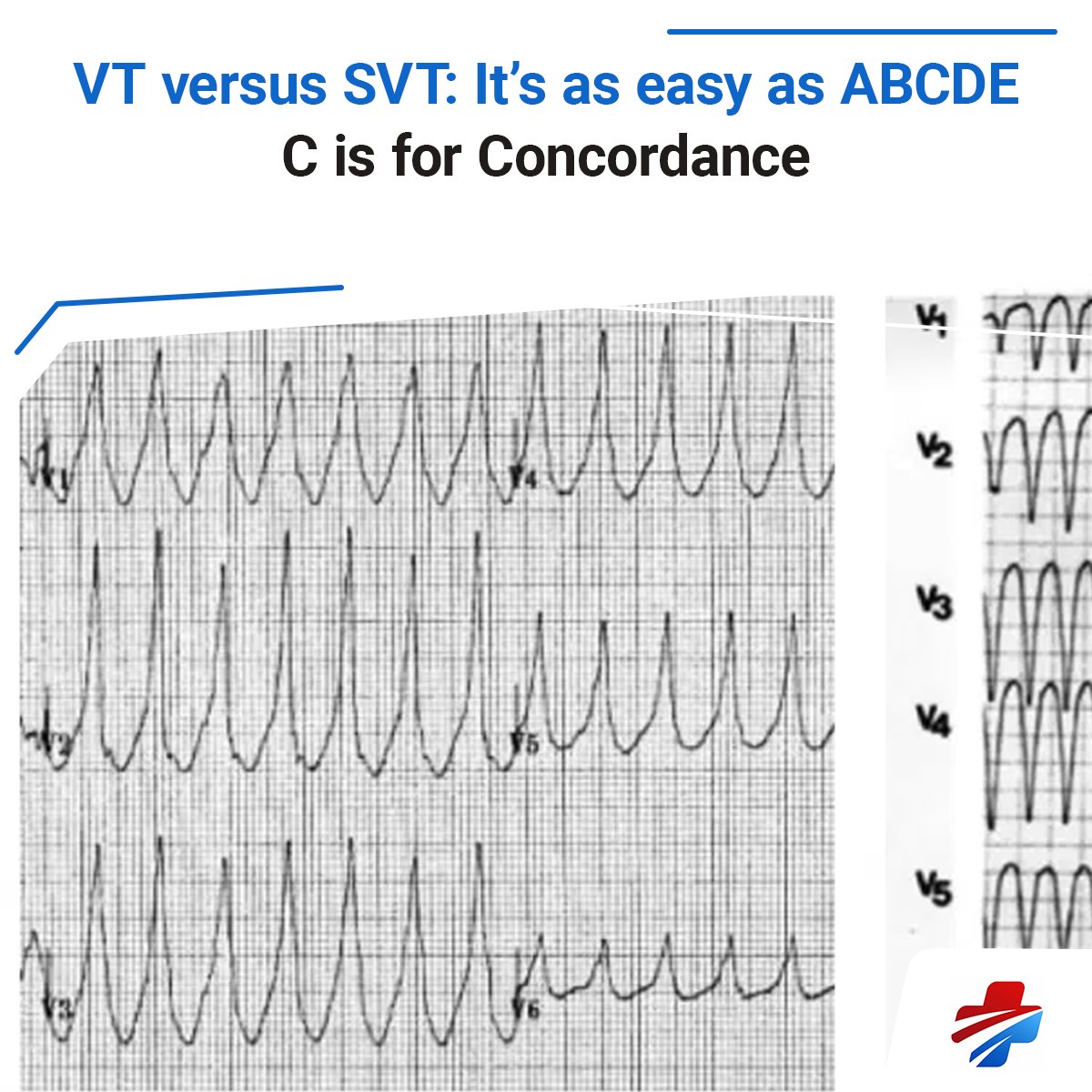
‘VT’ versus ‘SVT with aberrancy’.
The long list of VT "suggestive" ECG features is difficult to recall and apply in real time.
How can we simplify things?
Here is my ABCDE approach – five simple Qs to ask:
🧵👇
‘VT’ versus ‘SVT with aberrancy’.
The long list of VT "suggestive" ECG features is difficult to recall and apply in real time.
How can we simplify things?
Here is my ABCDE approach – five simple Qs to ask:
🧵👇
The ABCDE approach to VT v SVT
Came up with this last year when preparing an ECG talk for ICEM
Still my favourite piece of work giving a simplified, practical approach to a complex topic
https://t.co/5dBp3qPiWn
This is by far the best website for anything ECG. Whenever I read something that is new to me I just look it up on their website and read their straight-to-the-point articles. Check it our for anybody interested (they even have 150 ECG questions!)
Some great #pocus workshops still available - practical procedures with phantoms and live models, paediatrics and advanced US where you can learn high end US tips/advanced clinical integration from the experts. @broomedocs@rob_buttner @lukemphillips
1) Any patient who is a representation or failed discharge from the emergency department
2) When I am asked to “quickly send someone home" from the waiting room or triage
3) When an experienced clinician asks for advice on a patient
Knowing how to switch between system 1 and 2 thinking is one of the most important skills of an Emergency Clinician.
When do you choose to employ a System 2 approach?
Here are three situations for me. Comment with your own so we can improve our approach 👇🧵
@abuabdo2 I actually just wrote a walk and added
#6: F is for fragmentation of S wave in V1-2 (Josephson sign)
This is highly specific for VT and thought to be due to fibrosis from previous MI
By popular demand, the ABCDE approach is now an established part of the @LITFLblog ECG Library.
I've also added an optional F -- check out the post to learn more.
https://t.co/AowKI1SWfU
‘VT’ versus ‘SVT with aberrancy’.
The long list of VT "suggestive" ECG features is difficult to recall and apply in real time.
How can we simplify things?
Here is my ABCDE approach – five simple Qs to ask:
🧵👇
Differentiating regular narrow and wide complex tachycardias can be a challenge.
Can't see any P waves?
Here are three handy tricks to make things easier
🧵👇