Gasman, intensivist, resuscitationists, retired golfer, helping critically ill. Passionate about medicine. Slightly less serious than the rest :-) DESA #FOAM
Our reaction to any new study is either “I don’t believe it” or “I knew it”...
A NEJM trial in ICU pts w acute resp failure found that mucolytics (carbocisteine & hypertonic saline) don’t help. My ICU rounds line “mucolytics are useless” may need an update: “and possibly harmful”
Organ donation after #ECPR, narrative review aimed to examine associated clinical & ethical challenges, with particular attention to transition from resuscitative intent to donation-oriented care
⚠️ patient autonomy
📋 consent
⛔️ conflicts of interest
⚖️ equity of access in adults & peds
@Crit_Care
🔓 https://t.co/wyhWwqu3zf
First POCUS International Course in Warsaw 🇵🇱
Three days of intensive, hands-on training in TCCD, lung/abdominal/vessel ultrasound and echocardiography — delivered in English by an international faculty.
📅 11–13 Sept 2026
🔗 https://t.co/gD83vykjBQ
🌿 LIVE from Warsaw | Intensive Spring Conference 2026 🌿
We're thrilled to be part of #iSpring2026 – one of the most dynamic gatherings in critical care medicine, bringing together world-class intensivists from across the globe in the heart of Warsaw! 🇵🇱
🎤 Incredible panel discussions, thought-provoking lectures, and lively debates are already in full swing. Today's highlights include cutting-edge insights on:
💧 Fluid management in critically ill patients – When do you give a fluid bolus? Preload responsiveness, vasopressors, and the nuances of hemodynamic optimization are front and center.
🌍 Sustainability in the ICU – A timely session exploring the carbon footprint of intensive care, from Scope 1 to Scope 3 emissions, and what ICU teams can do to drive change.
📚 Proud to present our Springer open-access book "Rational Use of Intravenous Fluids in Critically Ill Patients" (Malbrain, Wong, Nasa & Ghosh) — available at the conference! 🎁
A huge thank you to our international faculty for sharing their expertise, and to all attendees who make this event such an energizing experience. The conversations happening here will shape critical care practice for years to come. 💡
📍 Warsaw, Poland | 14–16 May 2026
🏥 Supported by: Löwenstein Medical, Mindray, BD, Fisher & Paykel, GE, CIRRO & more
👉 Stay tuned for more updates throughout the conference!
#IntensiveSpringConference #iSpring2026 #CriticalCare #ICU #IntensiveCare #FluidManagement #Hemodynamics #Sustainability #MedEd #Warsaw #OpenAccess #IFAD #Springer #ManuMalbrain
Airway Management at a Crossroads: Why Global Adoption of Structured Airway Triage Could Transform Patient Safety
Johannes Huitink, MD PhD FEAMS
Airway management remains one of the most critical - and unforgiving - domains in acute care medicine. Despite decades of technological advancement, new devices, and refined guidelines, airway-related morbidity and mortality persist at an unacceptably high level. The paradox is striking: clinicians today have more tools than ever, yet adverse events continue to occur in operating rooms, emergency departments, and intensive care units worldwide.
The problem is not primarily a lack of knowledge or equipment. It is a failure of decision-making under pressure. Specifically, it is the inability to consistently match the right strategy to the right patient at the right time.
This is where the concept of structured airway triage - operationalized through an airway triage app methodology - has the potential to redefine global standards of care.
A 🧵 1/4
The Core Problem: Variability in Human Decision-Making
#airwaytriage #airwayassessment
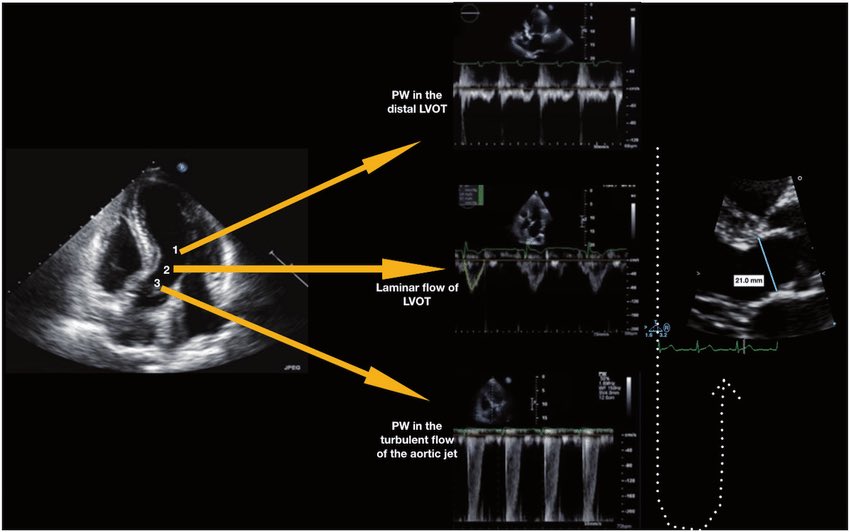
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → https://t.co/oCXGNgWsPF
👉 Pasipoularides et al. Am J Physiol 1984 → https://t.co/cfvNMpEgzG
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → https://t.co/lRVjLuYMEs
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → https://t.co/rf7l2FQUs4
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → https://t.co/avke1qOy4x
👉 Zoghbi et al. Circulation 1986 → https://t.co/KFiChfBNuc
👉 Oh et al. JACC 1988 → https://t.co/1C8sHRSMPq
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → https://t.co/U3hXFns4jx
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → https://t.co/iu07xBTwQS
👉 Hahn & Pibarot. JASE 2017 → https://t.co/uqgcv8kzO7
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni@JaeKOh2@ottoecho@WilliamZoghbi@ASE360@EACVIPresident@NephroP@iamritu@PPibarot@hahn_rt@MAecocardio@SISIACOficial@SONECOM_AC@VazyurVasquez@Cardiotweets83@HEARTof_echo@echobasics
🩺 Arterial line ≠ just a number on the monitor
If you’re only looking at MAP…
you’re missing most of the physiology.
🧠 Invasive BP is a real-time hemodynamic language
Every component tells a different story:
▪️ MAP → organ perfusion
▪️ DAP → vascular tone
▪️ SAP → LV afterload
▪️ Pulse Pressure (PP) → stroke volume surrogate
➡️ It’s not one number.
It’s a dynamic physiological system
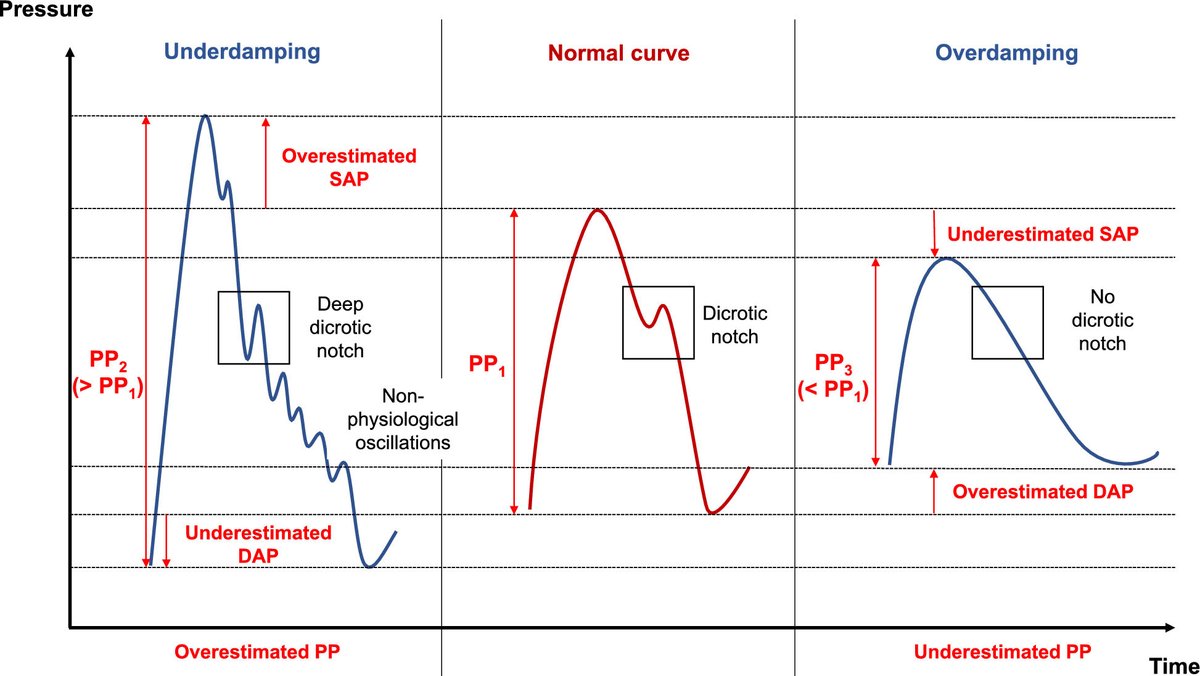
⚠️ First rule, often ignored:
👉 If the waveform is wrong → everything is wrong
Before interpreting:
✔️ Check damping
✔️ Perform fast flush test
✔️ Look for:
Rapid upstroke
Dicrotic notch
Smooth diastolic decay
➡️ Bad waveform = bad decisions
📉 MAP alone is NOT enough
We target MAP ≥65 mmHg…
but:
▪️ Duration of hypotension matters
▪️ Individual physiology matters
▪️ CVP matters
👉 Think instead:
🎯 Perfusion pressure = MAP − CVP (MPP)
➡️ A “normal MAP” can still mean hypoperfusion
🔥 DAP = your vasopressor trigger
Low DAP = low vascular tone
▪️ Septic shock → ↓ DAP
▪️ Early signal before MAP collapses
👉 Use it to:
✔️ Start norepinephrine earlier
✔️ Avoid delayed vasopressor therapy
➡️ It’s one of the most underused variables in ICU
⚡ Pulse Pressure = hidden CO monitor
PP reflects:
▪️ Stroke volume
▪️ Arterial stiffness
👉 Dynamic changes = key:
✔️ PLR
✔️ Fluid challenge
✔️ Ventilator cycles (PPV)
➡️ You can track CO trends without a CO monitor
🧬 Next-level physiology (very underrated):
New indices:
▪️ DSI = HR / DAP
→ identifies vasoplegia early
▪️ VNERi = DAP / (HR × NE dose)
→ detects norepinephrine resistance
👉 These may define who needs vasopressin early
💡 Mindset shift
Don’t ask:
❌ “What’s the MAP?”
Ask:
✔️ “What is the physiology behind this waveform?”
🧠 Take-home
Arterial line monitoring is not passive.
It’s:
▪️ Diagnostic
▪️ Therapeutic
▪️ Predictive
➡️ If you read it correctly…
it becomes a precision resuscitation tool
📚 Bertrand M et al. (2025)Annals of Intensive Care
DOI: 10.1186/s13613-025-01608-y
In a multinational cohort of ARDS patients, PaO2/FIO2 ratio was not associated with mortality and had poor prognostic utility, while driving pressure (ΔP) and the 4ΔP+RR index outperformed other variables in predicting mortality https://t.co/dafM1Xof06
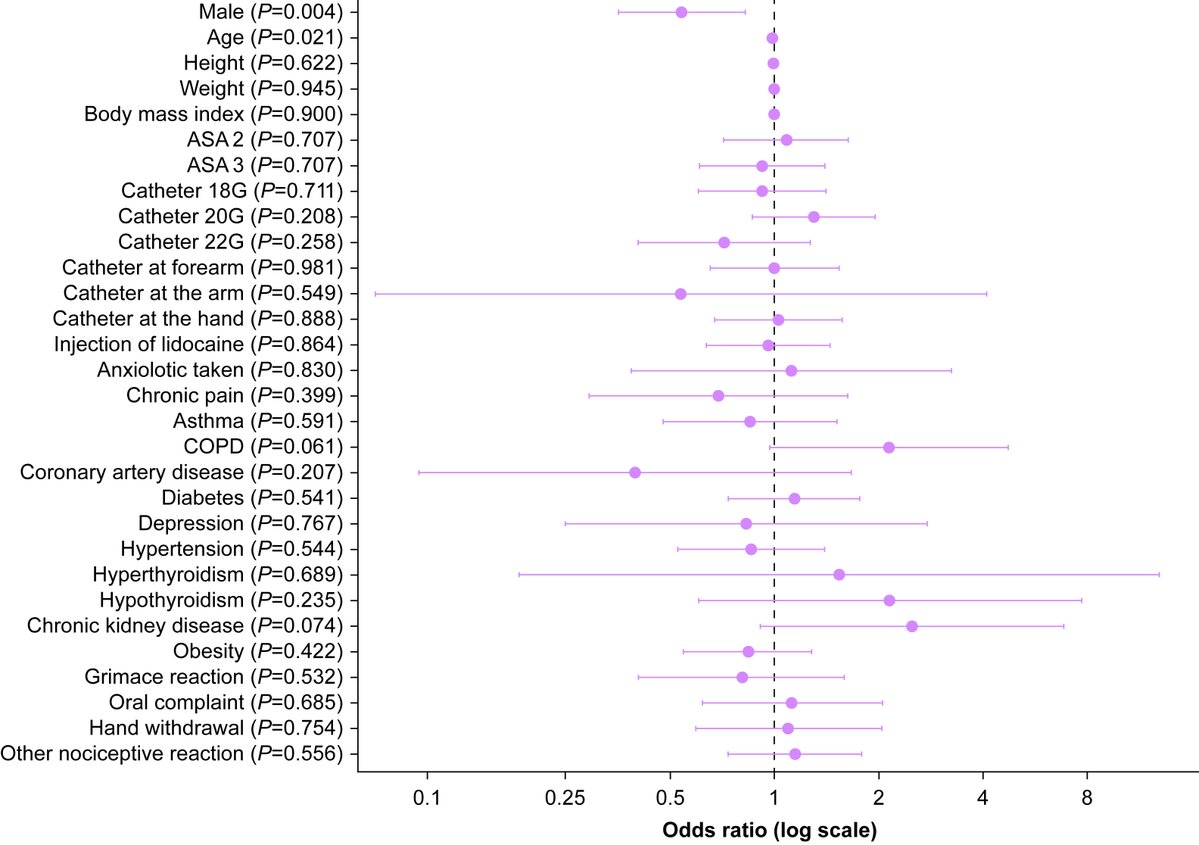
Is pain on #propofol injection at IV induction remembered by patients? After non-cardiac surgery, female sex was associated with pain recall but catheter characteristics, lidocaine use and observed nociceptive reactions were not #OpenAccess
https://t.co/XiZOPOO5eT
"Intensywnie o krwotokach" podczas #FIT2026
👉 trend ku bardziej restrykcyjnej polityce przetoczeń preparatów krwiopochodnych
👉 zwrócenie uwagi na różnorodne zaburzenia hemostazy
👉 rosnąca rola testów wiskoelastycznych u krytycznie chorych
👉 racjonalizacja podawania albumin
"Intensywnie o krwotokach" i nie tylko podczas #FIT2026
👉 wąskie wskazania do wodorowęglanów na OIT
👉 ważna optymalizacja "opieki okołoendoskopowej" w krwawieniach z GOPP
Today's Paper of the Day is:
Applied physiology at the bedside: using invasive blood pressure as a true monitoring tool
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
Nephrologist wanted to remove fluid with rrt. I said no, instead, gave some fluids. Can anyone guess why? I believe that EVERY nephro should incorporate POCUS in the assessment of AKI in ICU…
[1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24
🫀Hemodynamic monitoring. Are we measuring pressure or understanding physiology?
A recent review in Turkish Journal of Anaesthesiology and Reanimation revisits the fundamental elements of hemodynamics and exposes a persistent gap between monitoring and true physiological interpretation.
We measure more but, do we understand better?
-Blood pressure is not perfusion
Blood pressure is the most monitored variable in clinical practice
Yet it is only the product of flow and resistance
A patient may have normal pressure with low cardiac output
Or adequate flow with abnormal pressure
🫀 Clinical implication
Normal MAP does not exclude shock
Always question flow behind pressure
-Cardiac output is not enough
Cardiac output reflects macrocirculation
But tissue survival depends on microcirculation
The article reinforces that oxygen delivery depends on both flow and arterial oxygen content
🫀 Clinical implication
A normal cardiac output does not guarantee adequate oxygen delivery
Hemoglobin, saturation, and extraction must be integrated
-Oxygen delivery defines outcome
DO2 is the real currency of resuscitation
When oxygen delivery falls below a critical threshold
Oxygen consumption becomes delivery dependent
And cellular hypoxia begins
Lactate rises late
Extraction increases early
🫀 Clinical implication
Do not wait for lactate
Look at the trajectory of ScvO2, Pv aCO2 gap, and clinical perfusion
-Macro vs microcirculation mismatch
One of the most important concepts
You can normalize global hemodynamics
While microcirculation remains impaired
This explains why patients deteriorate despite “optimal” numbers
🫀 Clinical implication
If the patient is not improving
Reassess perfusion, not pressure
-Right ventricle. The forgotten determinant
The right ventricle is highly sensitive to afterload
And rapidly fails under pulmonary hypertension
Yet it is often overlooked in perioperative and ICU settings
🫀 Clinical implication
Always evaluate RV function in shock
Especially when response to therapy is unexpected
-Monitoring is evolving. Thinking must evolve faster
The review highlights future integration of macro and microcirculatory monitoring
But technology alone will not improve outcomes
Interpretation will
-Final reflection
We have learned how to measure hemodynamics
Now we must learn how to understand perfusion
📚 Demir ZA et al. Turk J Anaesthesiol Reanim. 2025. DOI: 10.4274/TJAR.2025.251925





































![FSotoMD's tweet photo. [1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24 https://t.co/uCviL2SL9n](https://pbs.twimg.com/media/Feq1bgWWYAEEcQs.jpg)































