🧬 Pre-Engraftment Syndrome (pre-ES) after Auto-HSCT: is prior PD-1 exposure a red flag? 🚨
🆕 2026 single-center study in R/R Hodgkin lymphoma
👥 64 adults undergoing BEAM auto-HSCT
💉 Prior PD-1 inhibitor exposure: 8/64 (12.5%)
• Pembrolizumab n=6
• Nivolumab n=2
⏱️ Median last PD-1 → ASCT: 41 days
🔍 Classical engraftment syndrome
❌ Spitzer ES: 0 cases
📌 Maiolino ES: 3/64 (4.7%)
➡️ None required steroids
🔥 But before neutrophil engraftment…
📈 Maiolino-compatible pre-ES: 34/64 (53.1%)
💊 Severe/steroid-requiring pre-ES: 3/64 (4.7%)
⚠️ All 3 also fulfilled Spitzer features outside the conventional timing window
🎯 Key signal
💥 All steroid-requiring cases occurred in patients previously exposed to PD-1 inhibitors
📊 Severe pre-ES among PD-1 exposed: 3/8 (37.5%)
🆚 non-exposed: 0/56
📉 Association: p = 0.0007
⏰ Timing matters
🔥 Median symptom onset: Day +4
🌱 Median neutrophil engraftment: Day +9
➡️ Clinically important inflammation may clearly precede ANC recovery
🧪 CRP clue
📈 Higher CRP already at Day 0: p = 0.036
📈 Persistently higher at Days +6–8: p = 0.019
🩺 Clinical pearl
Post-auto-HSCT fever ± rash/diarrhea/pulmonary infiltrates/capillary leak before engraftment should not automatically be labeled infection alone—especially after recent PD-1 blockade.
⚠️ Exclude infection aggressively first. If persistent/progressive inflammatory syndrome despite appropriate antimicrobials, consider pre-ES and timely corticosteroids.
🧠 Important caveat: “pre-ES” remains a descriptive, non-validated entity. This was a retrospective single-center cohort with only 3 severe events—hypothesis-generating, not practice-defining.
📚 Tóthfalusi D, et al. Medicina. 2026;62:738. DOI: 10.3390/medicina62040738. medicina-62-00738.pdf
#HSCT #AutoHSCT #HodgkinLymphoma #EngraftmentSyndrome #PD1 #Pembrolizumab #Nivolumab #BMT #KFSHRC #KSA #SOHO #ASH
📊 Variant Allele Frequency (VAF): One of the most misunderstood numbers in an NGS report!
A mutation being present is only part of the story. VAF tells you how frequently that mutation appears among all sequencing reads, helping clinicians interpret tumor biology, treatment response, emerging resistance, and even minimal residual disease (MRD).
🔑 Key points:
• VAF = Variant reads ÷ Total reads × 100
• VAF is NOT the percentage of tumor cells carrying the mutation
• Higher VAF does not always mean a more aggressive tumor
• Interpretation always depends on tumor purity, copy number changes, LOH, sequencing depth, and sample type
• Serial VAF measurements in liquid biopsy can help monitor response and detect resistance early
Understanding VAF transforms an NGS report from a list of mutations into meaningful clinical information.
What other NGS concepts would you like explained next?
#MedicalOncology #Oncology #NGS #VariantAlleleFrequency #VAF #PrecisionOncology #MolecularOncology #CancerGenomics #LiquidBiopsy #ctDNA #MRD #Biomarkers #TargetedTherapy #Pathology #Genomics #CancerEducation #FOAMed #MedEd #CancerConceptsExplained
NGS Report Interpretation Series – Part 2
A negative NGS report is not always truly negative.
Before interpreting any mutation—or the absence of one—always ask:
“Can I trust the technical quality of this test?”
Tumor cellularity, sequencing depth, coverage uniformity, DNA/RNA quality, limit of detection (LOD), mapping rate, duplicate reads, and overall QC determine whether genomic findings are reliable.
Remember: A mutation is only as trustworthy as the quality of the sequencing that detected it.
This infographic provides a practical framework for oncology fellows, DrNB candidates, pathologists, and practicing oncologists to systematically assess the analytical quality of every NGS report before making clinical decisions.
What QC parameter do you check first while reviewing an NGS report?
#NGS #PrecisionOncology #MolecularOncology #CancerGenomics #GenomicTesting #MolecularPathology #MedicalOncology #Oncology #LiquidBiopsy #Biomarkers #TargetedTherapy #PrecisionMedicine #DrNB #FOAMed #MedEd #CancerConceptsExplained
Scientists summarize the biological roles of p53, examine how TP53 gene alterations drive therapeutic resistance in #myeloid neoplasms, and compare contemporary classification frameworks.
🔗 https://t.co/ib8kJOgeNI
"Olutasidenib as maintenance therapy after treatment response in acute myeloid leukemia with persistent IDH1 mutation" read the full article in Blood Neoplasia: https://t.co/uSPZtQ61dK #AML#BloodNeoplasia
Venetoclax plus Idarubicin and cytarabine as frontline induction for newly diagnosed acute myeloid leukemia in young, fit adults: a real-world study | Annals of Hematology | Springer Nature Link https://t.co/xL6djaIiVK
New in @ActaHaematol: DLI after alloHSCT for myeloid malignancies — our 62-pt, 2001-2022 retrospective cohort.
📊 CR/CRi in 29% of therapeutic DLI recipients
📈 Responders: median OS 51 mo vs 4 mo for non-responders (P=0.008), seen across both acute and chronic myeloid subtypes.
⚠️ Complex karyotype, del5/7/17p, TP53/RAS/RUNX1/JAK2 mutations = worse outcomes
DLI remains a powerful GVL lever post-relapse, but genetics matter. https://t.co/Y4kvGUZ4ev
@MayoCancerCare@MayoTransplant #leukemia
Revumenib, DEC-C & Venetoclax combo in R/R AML looks good in KMT2Ar and NUP98 subsets...TBD in NPM1c 🤔 @JCO_ASCO#AML#Hematology#Leukemia#HemOnc https://t.co/bTelM4fgv9
🧬 EHA2026 | Precision Hematology
🎤 Speaker: Sören Lehmann
🧪 Topic: Treatment strategies in TP53-mutated AML/MDS
🚨 TP53-mutated AML/MDS remains a major therapeutic challenge
💊 VEN + HMA has become a common standard approach in TP53-mutated AML
📌 Reported with VEN/HMA:
CR rates ≈ 43–67%
EFS ≈ 6–7 months
OS ≈ 5–7 months
⚠️ VIALE-A signal:
VEN/AZA improved response in TP53-mutated AML vs AZA alone
But OS remained short and similar ≈ 6 months
🧠 Key message:
VEN/HMA increases remission rate
But remissions are often short
And survival remains poor
💉 HMA monotherapy in TP53-mutated disease:
AZA CR ≈ 20–40%
Decitabine CR ≈ 30%
Median OS often ≈ 7 months
📌 In MDS:
Lower TP53 VAF = better survival
Platelets >50 ×10⁹/L = better OS
🔥 Intensive chemotherapy in TP53-mutated MN is limited
3+7 chemotherapy:
CR ≈ 20–48%
Median OS ≈ 4–9 months
3-year survival ≈ 1–8%
⚠️ CPX-351 does not appear to overcome TP53-mutated chemoresistance
📊 Meta-analysis message:
IC, HMA, and VEN/HMA may produce CR/CRi
But OS remains clustered around very short medians
🧪 Metronomic VEN/AZA is emerging in TP53-mutated AML/HR-MDS
📌 Presented regimen:
Azacitidine 0.2 mg/kg SC weekly
Venetoclax 400 mg PO days 1, 8, 15, 22
28-day cycles
📊 Cohort: VEN/AZA-naïve HR-MDS n=26 + AML n=14
Median age ≈ 76.5 years
82% had biallelic TP53 mutations
✅ Outcomes:
AML OS ≈ 11.6 months
HR-MDS OS ≈ 9.9 months
48% of responders became MRD negative
Low toxicity reported
⚠️ Neutropenic fever ≈ 15%
No therapy-related fatalities
100-day mortality ≈ 7.5%
🎯 Clinical takeaway:
For TP53-mutated AML/MDS, higher response does not always mean durable survival
💡 Precision treatment must focus on:
depth of response 🧬
MRD negativity 🔍
toxicity balance ⚖️
bridging to transplant when feasible 🧫
novel TP53-directed combinations 🚀
#EHA2026 #PrecisionHematology #TP53 #AML #MDS #HRMDS #Venetoclax #Azacitidine #HMA #MyeloidMalignancies #Hematology #KFSHRC #ESH
A must read for all hematopathologists and heme molecular pathologists congratulations to @DrChrisHourigan and team on this very important publication
@BloodPortfolio
https://t.co/Slbi8to8um
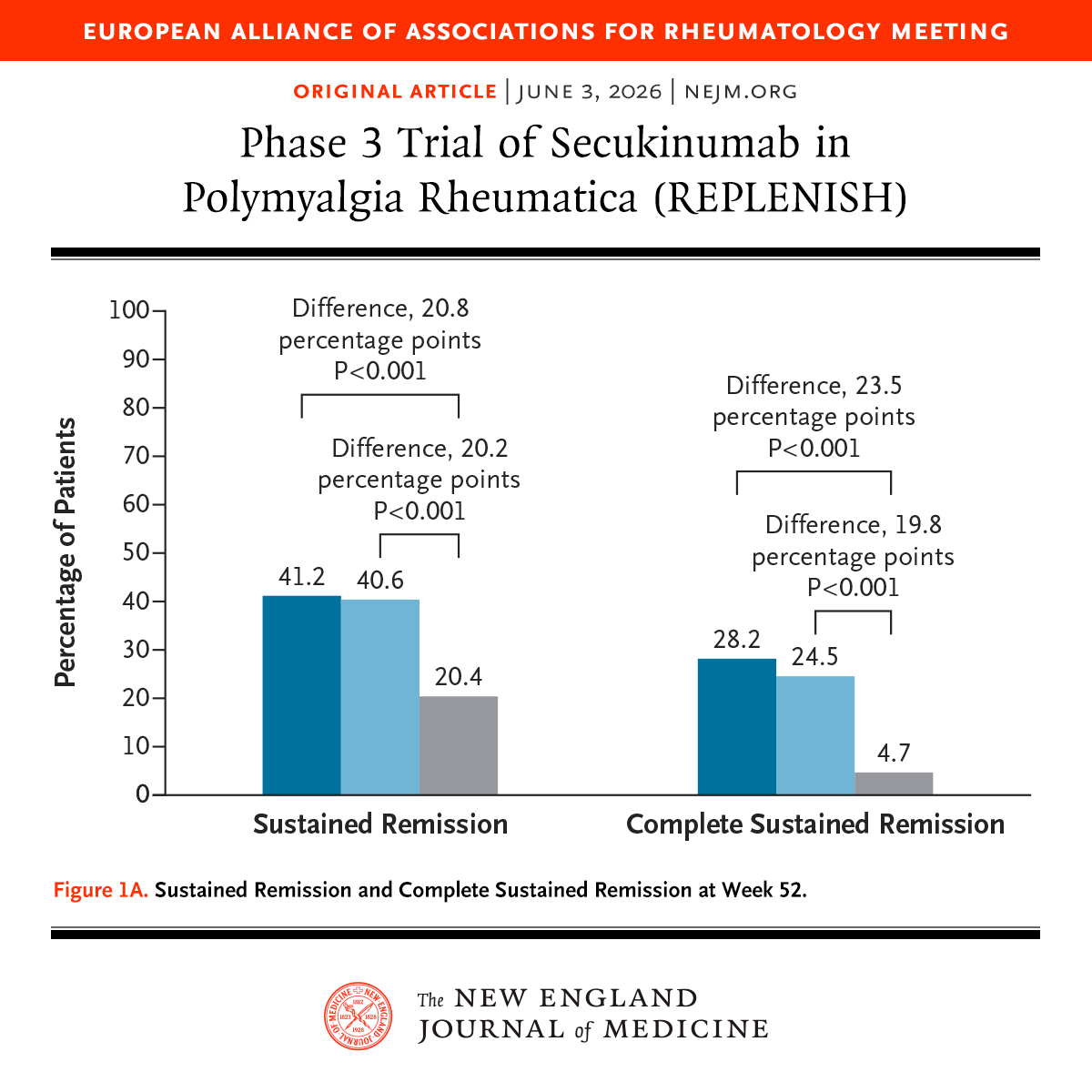
Presented at #EULAR2026:
Among patients with relapsed polymyalgia rheumatica, treatment with secukinumab plus a 24-week glucocorticoid taper resulted in a higher percentage of patients with remission than a glucocorticoid taper alone. Full phase 3 REPLENISH trial results: https://t.co/w1oD5ug1kJ
Editorial: Emerging Era for Polymyalgia Rheumatica and GCA — Interleukin-17A Targeting https://t.co/I13JtK01EA
Original Article in @NEJMEvidence: Secukinumab for Giant Cell Arteritis (phase 3 GCAptAIN trial) https://t.co/0dWjwDaEHs
@eular_org
Oral AML therapy just got real.
ASCERTAIN-V in NEJM tested all-oral decitabine-cedazuridine + venetoclax in newly diagnosed AML unfit for intensive chemo.
🩸 Phase 1-2, single-arm
👥 Phase 2b: n=101
🎯 CR: 47%
🎯 CR/CRi: 63%
⏱️ Median OS: 15.5 mo
✅ No PK drug-drug interaction
But this is not “easy venetoclax.”
Grade ≥3 AEs remained myelosuppression-heavy:
anemia 30%, neutropenia 26%, febrile neutropenia 25%.
The real message:
Convenience is oral.
The toxicity is still AML.
Early marrow assessment, venetoclax shortening, antifungal dose adjustment, G-CSF, and close monitoring are the treatment.
All-oral does not mean low-touch.
#OncoTwitter #MedTwitter #Leukemia #AML @OncoAlert@NEJM@esmo_open
This review article highlights how regulatory T cells can suppress acute and chronic #GVHD while preserving graft-versus-leukemia effects after #alloHCT. Early clinical studies demonstrate promising GVHD control low relapse rates and favorable survival. https://t.co/jd3taskfW5
#ASCO26#AML#leusm
Does venetoclax duration matter in frontline HMA+Ven for AML?
Poster: In a @MayoCancerCare analysis of 540 newly diagnosed AML patients, outcomes were driven primarily by disease biology, not venetoclax duration. Led by Dr. Naseema Gangat 👏👏👏
🔹 Similar OS across 7-, 14-, 21-, and 28-day schedules
🔹 Comparable outcomes within ELN 2024 and Mayo genetic risk groups
🔹 Higher early mortality with shorter durations likely reflected selection of frailer patients
🔹 In ELN high-risk AML, 14-day venetoclax was associated with inferior survival compared with 21- and 28-day schedules
Take-home: Venetoclax duration should be individualized based on genetics, response, cytopenias, and patient fitness rather than a one-size-fits-all approach.