The price and cost of American health care and coverage is intolerable. Luckily a growing number of states are doing something bold—rewarding patients with “deductible credit” when they pay a cash price below what their insurance company pays.
Why does it matter? Because instead of blowing through your entire deductible over a $6,000.00 MRI fee (not even the full episode of care), you can now directly pay ~$300 to a provider and have that out-of-pocket spending count towards your in-network deductible. If you as a patient do a better job at finding a price below what your health plan pays normally you should be rewarded and not penalized.
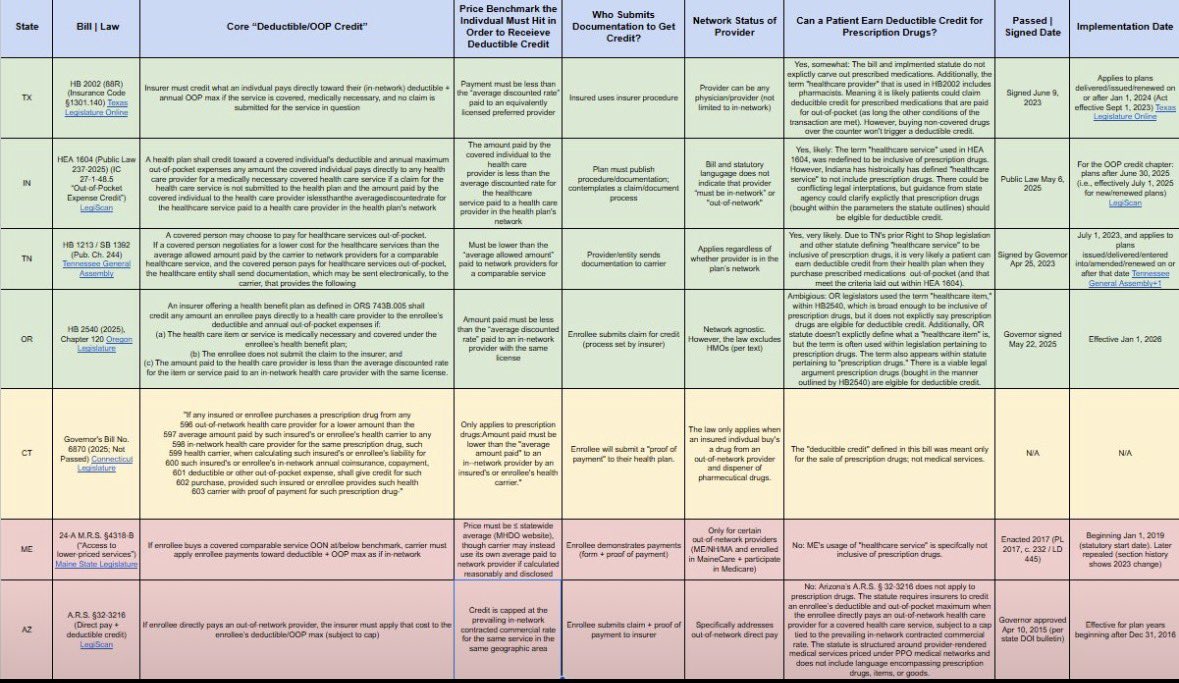
Attached is a table contrasting how states are going about implementing “deductible credit” laws. To date only 6 states have successfully implemented a variation of a deductible credit reform; however more state legislatures are getting poised to work on similar policy.
✅ = State has recently passed a law
🟡 = Attempted bill
🛑 = A proto version of deductible credit with limitations
https://t.co/GTHPRFz9Ej
Agreed… patients not knowing or caring how to utilize their health data isn’t a valid argument that justifies completely abolishing HIPPA.
Interoperability and actually making it possible for patients to use their protected health data according to their unique interest is a good North Star for reform.
Ya know @DrDiGiorgio, it’s disturbing that many healthcare-central-planning proponents’ arguments rely on the presuppositional belief that individual patients/physicians are incapable of producing a good health and financial outcomes for themselves…
Worst yet they then predispose the government will do a better job despite there being a long list of historical failures within the VA, IHS, Medicaid, Medicare, and ACA exchange…
Why is it so wrong to believe that a patient and good healthcare professional should be in the driver seat?
Probably not.
Extending 501(c)(3) status to an entity that can generate its own revenue and profit through the sale of goods and services it offers, is folly…
Unless you compel that entity to actually prove they offer some kind of valid and relevant community benefit that justifies the tax exemption (which the states nor the federal government does well)… you are essentially giving an unfair market advantage for consolidation to an entity that should be a for-profit but gets to avoid paying taxes. 8 out of the top 10 hospital systems in America are non-profits… Not surprising.
My evidence? Just look at Paragon’s graph showing hospital service rates in relation to inflation…
@HEALTHCOSTtruth Chargemaster rate application needs to be limited.
The fact hospitals can factor in their made-up chargemaster rates into cost-to-charge ratios for things like calculating Medicaid shortfall or medical debt sales (with third parties) is disgusting. Where is the accountability?
I agree.
The best community benefit that tax exempt hospitals can provide is affordable care and services.
If they can’t, they should not benefit from being tax exempt.
My dream for healthcare in Texas is this. Every time, every patient. Price transparency, HB2002, ensuring innovators like @Curative and @sidecarhealth have room to grow are done. But I am not finished yet, not until my dream is reality for all Texans. Stay tuned….
TRS/ERS need a cash pay based plan option. And we need to close the loophole that lets providers deny a cash price to someone with insurance and force them to use their insurance. Excellent work @JoinCrowdHealth!
“Physician-owned hospitals cherry-pick profitable cases.” The nonprofit across the street runs a hedge fund, owns a Gulfstream, and pays its CEO $8M. Sure, the surgeons owning their OR is what threatens the community.
VUMC made $270 million last year.
Paid $0 in federal income taxes.
Borrowed at municipal bond rates their for-profit competitors can’t touch.
They call it charitable mission.
The IRS calls it 501(c)(3).
Tennessee calls it the largest hospital in the state.
@DutchRojas They also charge their “discounted cash prices” for shoppable services, ~350% - ~850% more than any nearby ASC or independent provider (offering the same services).
Check the cash pricing map in this Forbes op-ed (a little dated, but still relevant): https://t.co/8qoAvj6Ubu
@mass_marion Posting prices was never going to drastically change patients’ behaviors—it was the first step.
It was a massive fight just to get prices out there. Now policy makers are incentivizing patients to use the emerging pricing information to their advantage: https://t.co/8qoAvj6Ubu
It is not run as a hospital primarily. It is an investment firm under the cover of a tax exempt status. The doctors are the minions giving credibility to the “hospital” label.
@DrDiGiorgio And worse yet, the same large health centers will send lobbyists to state capitols and Congress claiming they should be free of inventory tracking and transparency… this is foul and this type of abuse should be considered criminal.