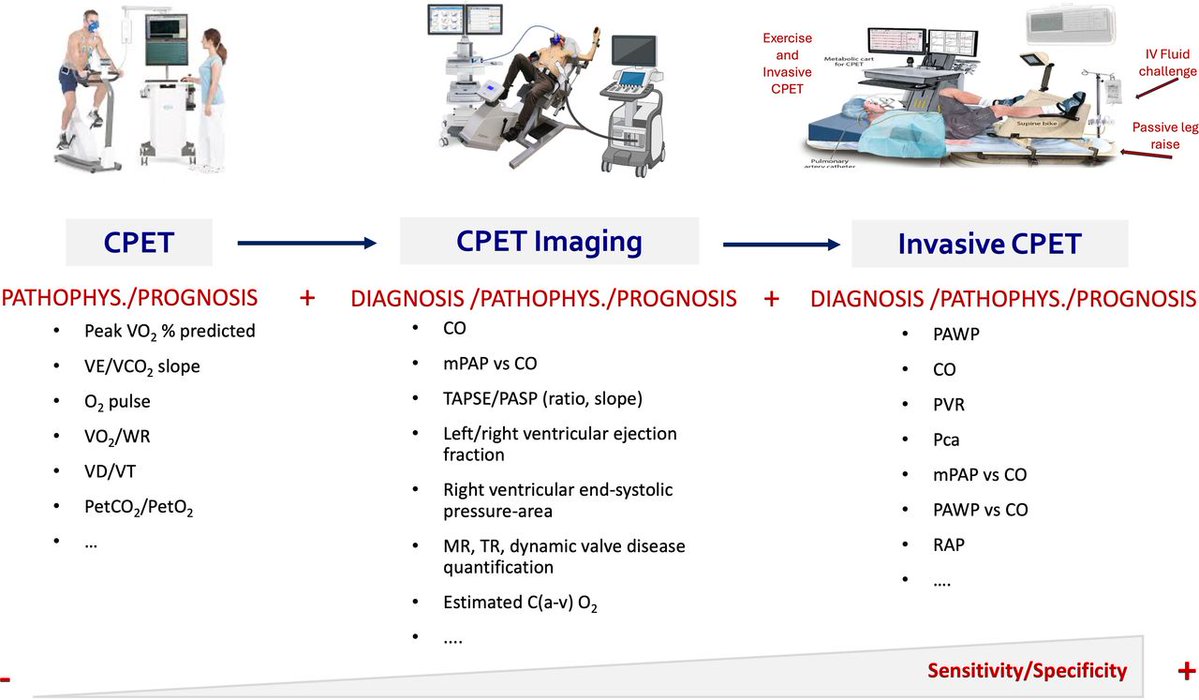
How do you differentiate the athlete's heart from underlying cardiovascular disease? 🫀🏃
New EAPC/EACVI Clinical Consensus Statement provides practical guidance on exercise imaging from stress echocardiography to advanced multimodality imaging—to improve diagnosis, risk stratification, sports eligibility, and exercise prescription in athletes.
Read more: https://t.co/hvlueCObzc
#SportsCardiology #CardiovascularImaging #ExerciseImaging
@EJPCEiC@AboyansV@SilCastelletti@PTBuketAkinci@PeroneFrancesco@SMosteoru@TimKambic #EJPC
In 773 pts from the PARADIGM registry, higher epicardial adipose tissue on #yesCCT was independently linked to coronary plaque progression and worse 10-yr #MACE-free survival, pointing to EAT as a potential marker for risk stratification. https://t.co/fVbEasYHU4 #JACCIMG
Many pts with #HFpEF who first present with EILAH transition to RELAH, thus suggesting that EILAH may represent an earlier stage of HFpEF. A history of #AFib, impaired LA compliance, & reduced PA compliance are associated with progression to RELAH. https://t.co/1ivBOYEccA #JACCHF
@Tartismalar Por favor, mira con detenimiento el video. Se trata de un vuelo privado. En todos lo aeropuertos del mundo siempre hay una inspección de seguridad, antes de montarse a un avión, sea vuelo nacional o internacional.
Lo hacen en la pista porque allí mismo se ve que esta su avión.
🚨 Can serial CMR redefine risk stratification in HCM?
A new study suggests that it may not be the amount of fibrosis alone that matters—but how quickly fibrosis progresses over time.
Researchers followed 313 patients with hypertrophic cardiomyopathy (HCM) who underwent two CMR scans approximately 4 years apart, assessing changes in late gadolinium enhancement (LGE), a marker of myocardial fibrosis.
🔍 Key findings
📈 Myocardial fibrosis increased substantially over time:
Median LGE mass increased from 2.9 g to 8.3 g
LGE prevalence rose from 72% to 91%
Extensive fibrosis (LGE ≥15%) doubled from 7% to 15% of patients.
⚠️ Nearly 70% of patients without LGE at baseline developed fibrosis on follow-up CMR.
💡 The most important finding was the rate of fibrosis progression:
ΔLGE >1.5 g/year independently predicted adverse clinical outcomes
Patients with rapid fibrosis progression had more than a twofold increased risk of death, transplant, HF hospitalization, stroke, or aborted sudden cardiac death
Adding ΔLGE/year to conventional risk models significantly improved risk prediction and reclassification.
❤️ For hard endpoints (death, transplant, aborted SCD), a fibrosis progression rate of >3.75 g/year identified particularly high-risk patients.
🎯 Clinical implications
Current guidelines already recommend repeat CMR every 3–5 years in HCM. This study provides strong support for that recommendation and suggests that:
✅ Serial CMR should be viewed as a dynamic monitoring tool rather than a one-time assessment
✅ Fibrosis progression may identify high-risk patients who appear low-risk according to conventional risk scores
✅ Imaging intervals could potentially be personalised based on fibrosis progression rates.
📚 One particularly striking observation: patients considered "low risk" by traditional ESC or AHA/ACC criteria but showing rapid LGE progression often had worse outcomes than some patients classified as high risk with stable fibrosis.
🧬 The future of HCM risk stratification may therefore move beyond a static fibrosis threshold toward a dynamic assessment of myocardial fibrosis progression.
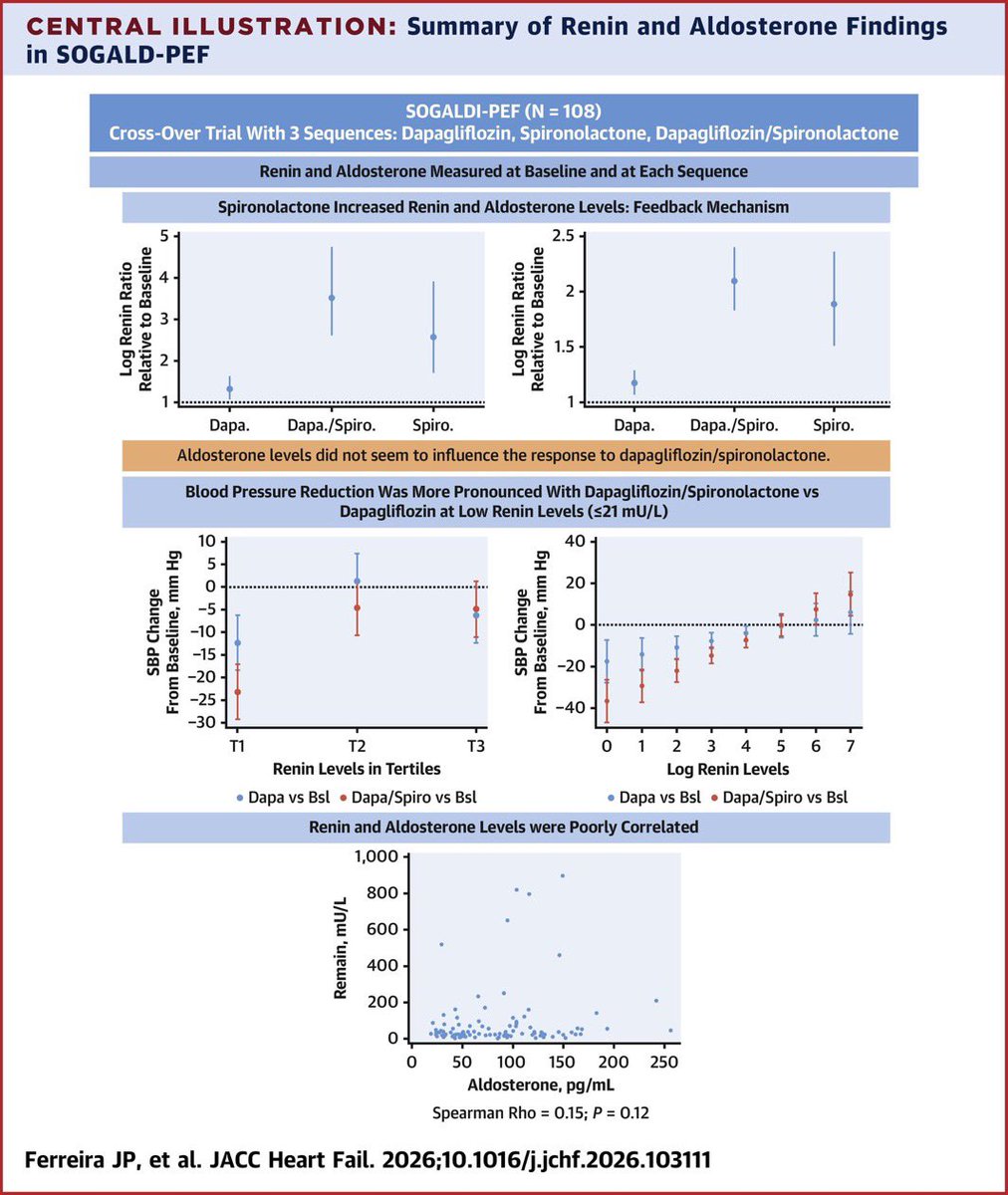
In HFpEF, measure renin before choosing between SGLT2i alone vs SGLT2i + spironolactone combination. Low renin patients benefit most from combo.
Spironolactone activates RAAS feedback loop
Low renin better response to the combination
Renin and aldosterone are poorly correlated
Ejercicio & prueba de esfuerzo en el Sx de Brugada. 🏃♂️🫀⚡️
🔹 El momento clave no es el ejercicio, sino la recuperación. Solo ~1% de los pacientes desarrolla patrón tipo 1 durante el esfuerzo, mientras que hasta 25.5% lo manifiesta en la fase de recuperación, cuando ocurre el rebote vagal tras el retiro del estímulo simpático. 🤔🏃♂️⏱️
🔹 La recuperación temprana (primeros 2-3 minutos) es la ventana más importante. Es aquí donde pueden aparecer el patrón tipo 1 de Brugada, elevación del ST/J-point, extrasístoles ventriculares, TV o FV en pacientes de alto riesgo. 🧐⚠️⚡️
🔹 Se asociaron con mayor riesgo de eventos arrítmicos: Aumento del ST durante la recuperación, extrasístoles ventriculares entre 1.5 y 3 minutos de recuperación, recuperación rápida de la FC (marcador de hiperactividad vagal), prolongación de la pendiente ascendente de la onda S en ejercicio máximo. 👨⚕️📝
��🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 👌🏻💯
https://t.co/pKL8FJz2HZ
https://t.co/4PnV0aMMfn
Bempedoic acid just got a new unexpected benefit — less blood clots?
Could bempedoic acid have a role beyond LDL lowering?
Possible mechanisms:
🔸 Anti-inflammatory effects (↓ hsCRP)
🔸 Lipid-inflammation-coagulation axis?
🔸 Off-target pleiotropic effects?
We know that aspirin can often be safely discontinued after PCI, provided it is not stopped too early. But how early is too early?
In this meta-analysis of 11 RCTs including 37,443 PCI patients—now incorporating the recent NEOMINDSET and TARGET-FIRST trials—we found that aspirin discontinuation at either ≤3 months or ≤1 month, followed by P2Y12 inhibitor monotherapy, reduced bleeding without increasing MACE compared with 12-month DAPT.
The key finding is that while discontinuation within the first month may provide an additional bleeding benefit, it appears to come at the cost of increased stent thrombosis, particularly in patients at higher ischaemic risk.
https://t.co/83VoBaFuiS
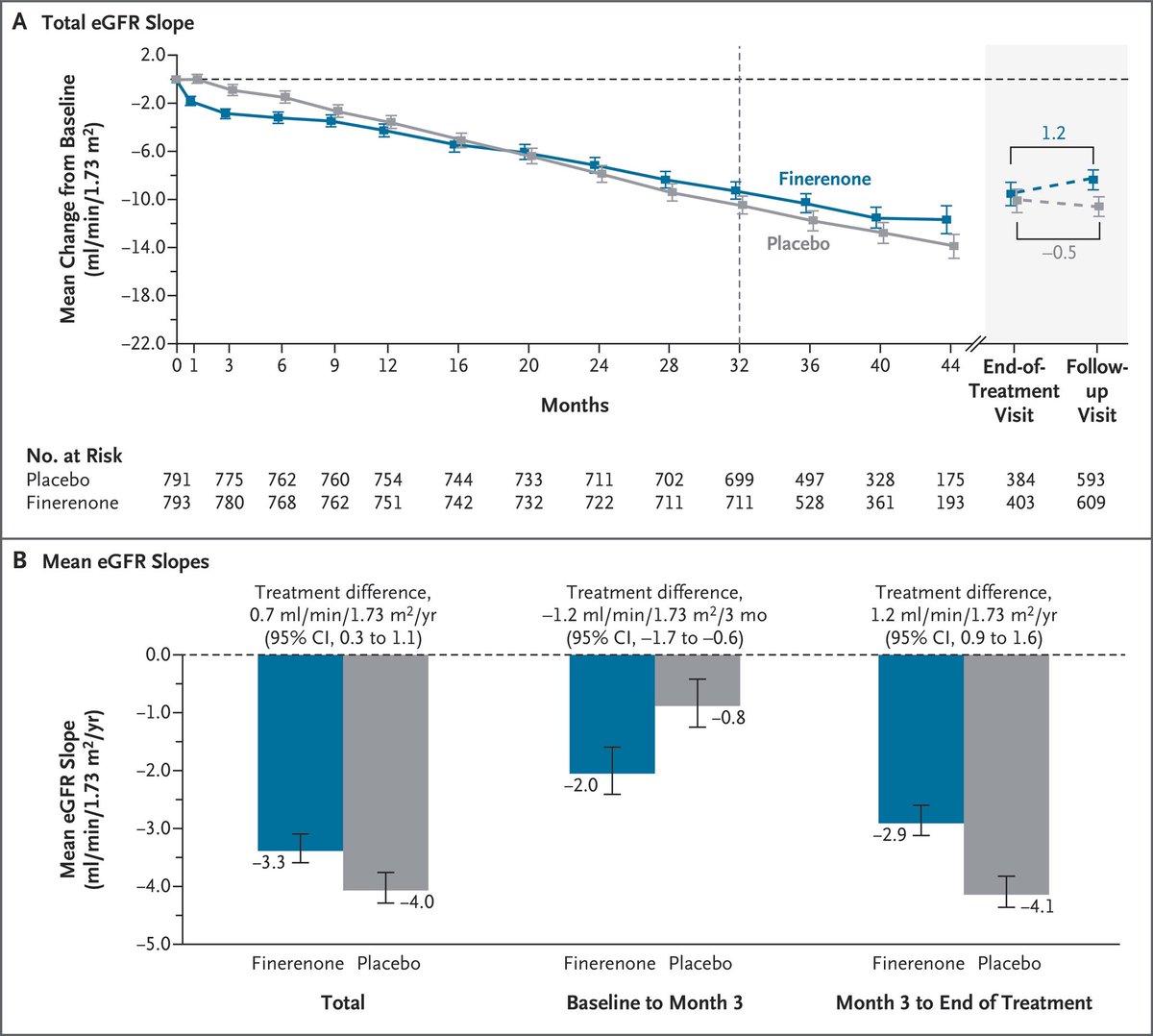
🔵 FIND-CKD Trial Results are out in @NEJM!
Finerenone vs placebo in non-diabetic #CKD:
A new era for non-diabetic #CKD treatment?
⚠️ Acute dip at month 1 (hemodynamic effect) — then sustained preservation
https://t.co/JF0jn71EV3
Terapia antitrombótica después de la cirugía de revascularización coronaria (CABG). 💊💥🫀
💊Aspirina: la piedra angular. La aspirina reduce la oclusión de injertos y los eventos CV sin incrementar significativamente el sangrado postoperatorio.
✅Mantener aspirina perioperatorio.
✅Reiniciarla dentro de las primeras 24 horas tras cirugía (idealmente antes de las 6 horas).
✅Continuar de forma indefinida a dosis bajas (75-100 mg/día).
💊💊¿TAP Dual? En pacientes con alto riesgo isquémico y bajo riesgo hemorrágico, puede considerarse aspirina + ticagrelor o clopidogrel durante 12 meses (indicación mas fuerte en SICA que en SCC) para mejorar la permeabilidad de los puentes venosos (reducen MACE pero aumentan 🩸).
✅Reiniciar TAPD tan pronto como el riesgo de sangrado esté controlado.
✅Mantenerla durante 12 meses.
✅Ticagrelor o prasugrel son preferibles a clopidogrel por su mayor reducción de eventos isquémicos y mortalidad.
📄🆓️⤵️ @ESC_Journals 💯
https://t.co/IcdxvQsTD9
https://t.co/SeTF6YUsXm
💊 Perioperative antiplatelet management is not “stop aspirin 7 days before surgery.”
It is a balance between surgical bleeding and catastrophic arterial thrombosis.
Recent PubMed indexed guidance is clear: in non cardiac surgery, the highest risk patient is not the one taking aspirin. It is the patient with a recent coronary stent, recent ACS, recent stroke, or high thrombotic burden in whom interruption of antiplatelet therapy may trigger myocardial infarction, stent thrombosis, or stroke (Thompson et al., 2024; Douketis & Spyropoulos, 2023).
For elective surgery, timing matters. After PCI, elective non cardiac surgery should ideally be delayed until the minimum recommended DAPT period is completed. If surgery cannot wait, aspirin should usually be continued when bleeding risk is acceptable, especially in patients with coronary stents. P2Y12 interruption, when necessary, should be as short as possible: clopidogrel usually 5 days, ticagrelor 3 to 5 days, and prasugrel 7 days before surgery (Thompson et al., 2024; Swan et al., 2024).
Emergency surgery is different. The decision becomes procedural urgency, bleeding site compressibility, last dose, platelet function recovery, and whether the antiplatelet effect can be tolerated. Platelet transfusion may partially reverse irreversible agents such as aspirin and clopidogrel, but it is much less reliable for ticagrelor because circulating drug can inhibit transfused platelets (Swan et al., 2024).
Recent evidence also challenges dogma. In stable patients with previous drug eluting stents undergoing low to intermediate risk non cardiac surgery, aspirin continuation did not clearly reduce ischemic events compared with temporary interruption, although minor bleeding increased (Kang et al., 2024). This does not mean “stop aspirin in everyone.” It means individualize.
The practical question is not:
“Should antiplatelets be stopped?”
It is:
What is more dangerous for this patient: bleeding today, or thrombosis tomorrow?
#Anesthesiology #PerioperativeMedicine #Cardiology #AntiplateletTherapy #Aspirin #Clopidogrel #Ticagrelor #Prasugrel #NonCardiacSurgery #PatientSafety
References 📚
Douketis, J. D. NEJM Evidence, 2(6). https://t.co/zms5Bz8MAE
Kang, D. Y. Journal of the American College of Cardiology, 84(24), 2380–2389. https://t.co/p9iMZBqx7M
Swan, D., Research and Practice in Thrombosis and Haemostasis, 8(6), 102548. https://t.co/61A5TyzWbO
Thompson, A., Journal of the American College of Cardiology, 84(19), 1869–1969. https://t.co/ExOBujTyfY
50%+ pts w/ #cvCAD & ischemia report dyspnea, & ~10% may have undiagnosed #HFpEF. Those w/ high HFpEF probability had worse symptoms, lower exercise capacity, & higher HF hospitalization risk, but saw the greatest benefit from an invasive strategy. https://t.co/dtUaOV69km #JACCHF