#ASCO26
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
📌 Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
🧬 RAS G12 population
91.8% of patients had RAS G12 mutations
📈 OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001
📈 OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001
📊 PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001
📊 PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001
🔥 12-month OS
Overall population: 53.2% vs 17.3%
⚠️ Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.
https://t.co/Y4WJRlRRTk
@TheGutonclab@UGrewalMD@TimothyJBrownMD@OncoAlert@Onco_Nexus@ASCO@NazliDizman@LauraAlderMD@DVAraujoMD@DrBarbiOnc@LauraEsfeller@FunchainMD@YGaritaonaindia@DrSAHaddad@jgong15@iandresmeraz@SakditadMD@RamilaShilpakar@RohitBanwar@lungoncdoc
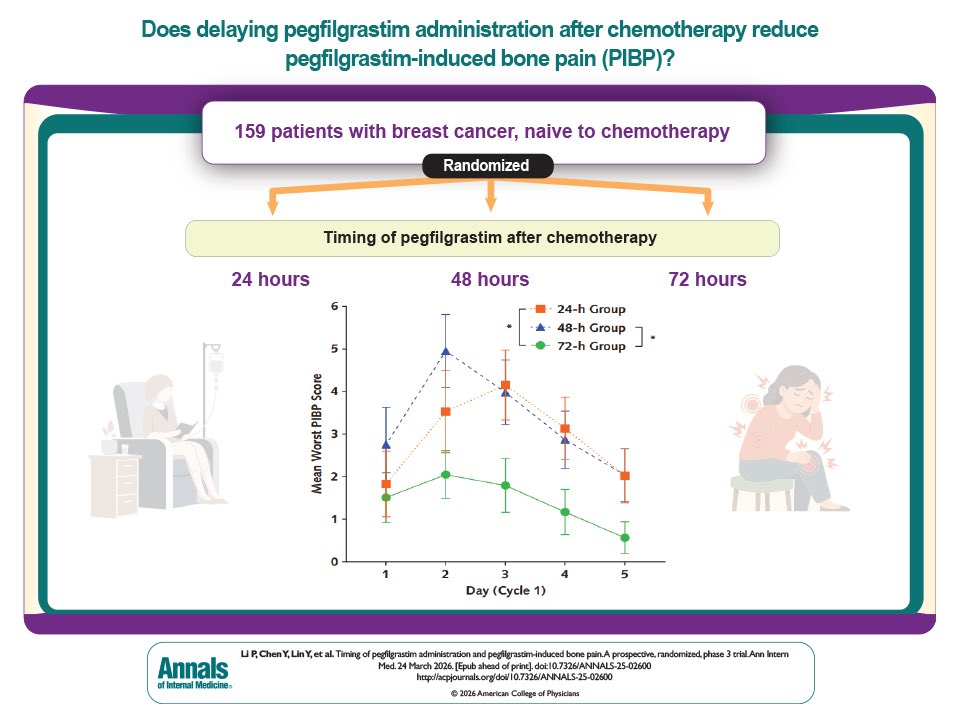
💉 Pegfilgrastim timing matters
📊 Phase III RCT (breast cancer)
⏱️ 72h vs 24–48h post-CT
📉 Bone pain (AUC): 6.05 vs 12.7–14.2 🔥
📉 Severe pain: 22.6% vs ~60%
⚖️ No ↑ neutropenia or FN
💡 Delaying to 72h may reduce toxicity without compromising efficacy
🔗 https://t.co/0bdcsKtITk
@OncoAlert
What REALLY makes a good oncologist? in @JCO_ASCO
After 10 years and 203 JCO essays, one thing became clear: expertise alone isn’t enough.
Patient-centered care.
Clear, authentic communication.
Emotional intelligence.
And the harder work
Showing up again and again.
Openness to uncertainty.
Carrying the burden of cancer care.
Continuous growth.
Clinical competence is expected
Human connection makes the difference.
Science treats disease.
Presence treats fear.
https://t.co/g9hGjSLpGu @OncoAlert
Promoting Fairness in Screening Programs for Late-Career Practitioners | New England Journal of Medicine https://t.co/yM2NqUIclB
In their article discussing screening late-career physicians (LCPs), the authors[1] build an elaborate schema to identify and possibly manage impaired LCPs beginning empirically at age 70. Cognitive and physical impairments are in fact medical conditions and should be addressed as such. Though I am sure their efforts are well-intentioned, the authors completely miss the mark in that they have failed the basic tenets of managing an identified medical disorder.
(1) Prevalence. The authors do not state the prevalence of impairment in LCPs. For published data, they rely on a single analysis[2] scanning the medical literature from 1966 through 2004. The authors of that study do not provide prevalence data regarding impaired LCPs but rather state "physicians who have been in practice longer may be at risk for providing lower quality care"; key word is "may". The absence of prevalence is a basic flaw.
(2) Validated screening tool. The authors have not outlined validated screening tools ("test instruments") with high sensitivity and specificity for identifying impaired LCPs. Such tools must first be tested, validated, and universally accepted before any screening can be considered.
(3) Establish effective outcomes with intervention. What is the appropriate treatment? This will depend on whether the impairment is physical, cognitive, or both. Though studies may provide broad guidelines, I would suspect that each institution would develop its own locally accepted methods for intervention.
Yes, there are impaired late-career physicians. I would suggest that the problem is not nearly as severe as what the authors suggest. The authors have, however, succeeded in sowing the seeds of distrust amongst the general population of physicians and LCPs, between LCPs and administrators ("gaming" the testing), and most importantly between LCPs and their patients.
We should inquire of the senior author whether such screening efforts are established in the legal profession. I would posit not. Four (Thomas, Alito, Chief Justice Roberts, and Sotomayor) of the nine US Supreme Court Justices are over age 70. I am unaware of efforts to screen for impairment of these Justices who are responsible for major judicial decisions affecting almost 350 million people.
As outlined by the authors, implementation of their proposal would be in direct violation of existing
employment discrimination law (ADEA, Age Discrimination in Employment Act).
The authors are ahead of their skis. Please go back to the drawing board, perform standard epidemiologic workup, and then get back to us.
1. Kramer DB, Gallagher TH, Osinska PH et al. Promoting fairness in screening programs for
late-career practitioners. NEJM 2026;394:401-407.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between
clinical experience and quality of health care. Ann Intern Med 2005;142:260-273.
#physician #late #career #impairment #NEJM #screen #opinion #rebuttal
Any daily #alcohol consumption is associated with certain cancers, and the risk of #cancer increases with higher alcohol intake.
📊 This JAMA Insights discusses the evidence related to the @Surgeon_General’s Advisory on alcohol and cancer risk.
https://t.co/7iNaQIWYOb
State legislators, attorneys general, and insurance regulators all agree that a 10-year moratorium on state regulation of #AI, including health AI, is bad policy. Patients and physicians can’t wait for federal action--states policymakers must be able to establish guardrails around AI. Read their letters to Congress -
➡️ National Conference of State Legislatures: https://t.co/M2shqyesAn
➡️ National Association of Attorneys General: https://t.co/Dw1hvRdCSf
➡️ National Association of Insurance Commissioners: https://t.co/7g3KzaRipF
🧂Hyponatremia is a common the ICU, but correcting it smoothly & safely can be challenging.
🧠Rapid correction risks serious complications like ODS/CPM
📈That's why I built NaPathway - a free app - to help clinicians monitor sodium correction
Try it https://t.co/nE8tFI5d0k
🧵
A @PennCancer team has defined a network of tumor-intrinsic and immune-related molecular traits that distinguish the subset of early stage HPV+ oropharyngeal cancers predisposed to fail standard therapy:https://t.co/aRNxdBAjw1
@basulab1@PennMedicine@Penn_ENT@Penn_CBIO.
International Myeloma Society/International Myeloma Working Group Consensus Recommendations on the Definition of High-Risk Multiple Myeloma | Journal of Clinical Oncology https://t.co/0hGDHjyQLf
In the VERITAS trial, biopsy of indeterminate pulmonary lesions with navigational bronchoscopy was noninferior to that with transthoracic needle biopsy and led to fewer complications. Full trial results and Research Summary: https://t.co/w31rawTjYa
@BAUSurology@ProstateUK@thetimes@vishhanchanale@rylance_amy Nonsense. Again, more of the hand-wringing touchy-feeliness of the nanny state. Physical examination is the mainstay of medical practice and must remain so. Laboratory and imaging results do not replace the time-tested value of the physical examination.
🧬 New study highlights germline risks in gastric cancer (GC):
📊 Of 3,706 GC patients tested, 13.3% had pathogenic/likely pathogenic variants (PGVs)
🧠 Most common genes:
🔹 BRCA1/2, PALB2, ATM (HRR) – 35%
🔹 CDH1, CTNNA1 (Hereditary Diffuse GC) – 19.5%
🔹 Lynch syndrome genes – 17.4%
👨⚕️ PGVs more common in males & those with other cancers (OR ~1.3–1.4)
📈 Significant enrichment vs non-cancer cohort
🔍 Implication: Germline testing should be considered in all GC cases!
https://t.co/EVjuDuleTw