NORMAL PRESSURE HYDROCEPHALUS
NPH is one of the more controversial diagnoses in neurology. Depending on who you ask, it’s vastly overdiagnosed, underdiagnosed, or even nonexistent. Here’s a thread on diagnosis, imaging, and management.
Amyotrophic lateral sclerosis (#ALS) is an adult-onset neurodegenerative disorder characterized by progressive muscle weakness due to degeneration of upper motor neurons in the brain and lower motor neurons in the brainstem and spinal cord.
Diagnosis relies on clinical criteria with mixed upper and lower motor neuron features, and is often supported by electromyography and genetic testing, which may direct treatment.
📌 Learn more in this JAMA Review: https://t.co/2gvxr8EQUA
#RadInTraining#Tweetorial
1/16
Clinical MRI Biomarkers to Differentiate Parkinson's Disease from Its Mimics 🧠 ✨
Parkinson's disease is still primarily a clinical diagnosis, but MRI can add meaningful diagnostic value when interpreted beyond “no acute intracranial abnormality.”
Spin Tweetorial Wednesday
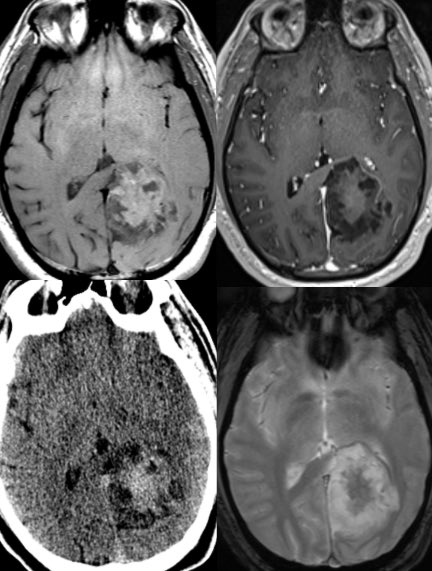
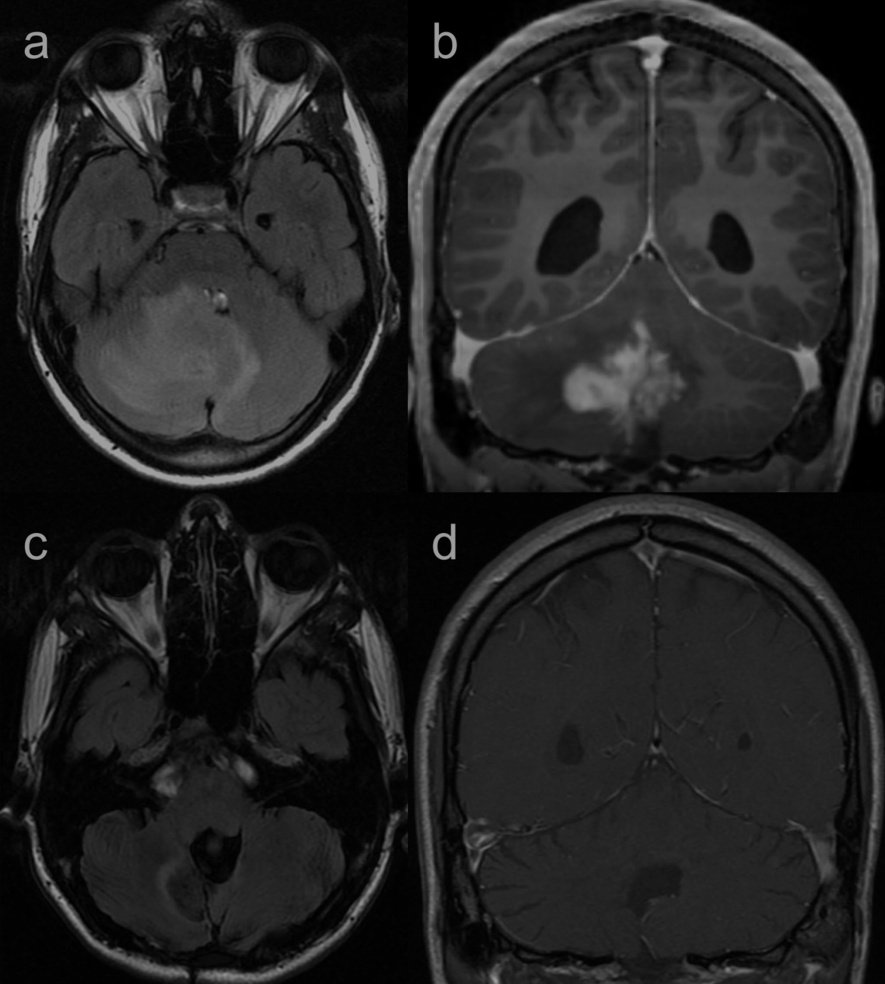
Wiskott–Aldrich Syndrome: The great tumor mimic.
📌 Young patient with immunodeficiency + thrombocytopenia
📌 Presents with progressive headache
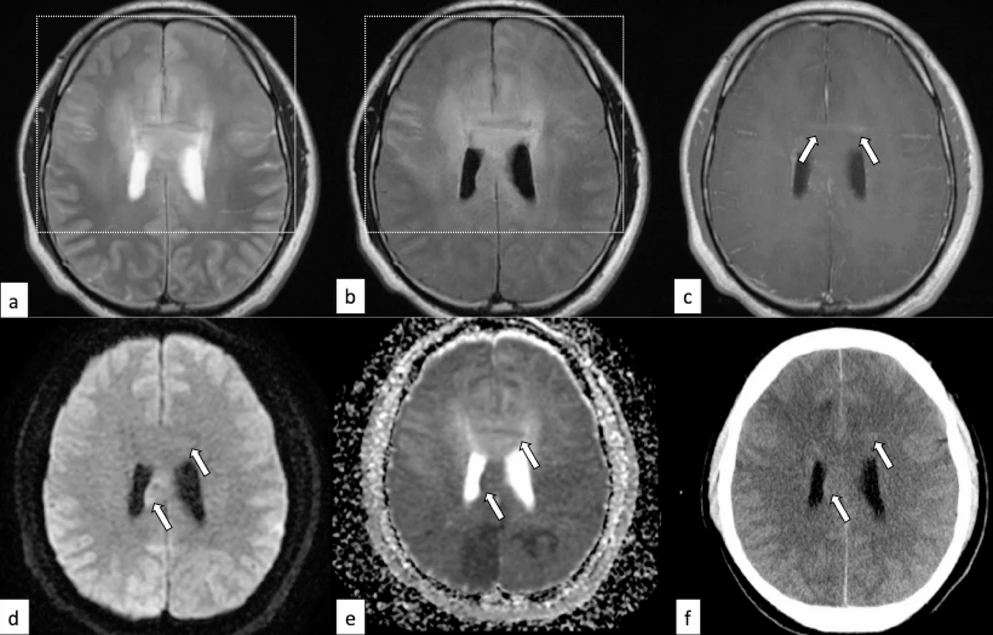
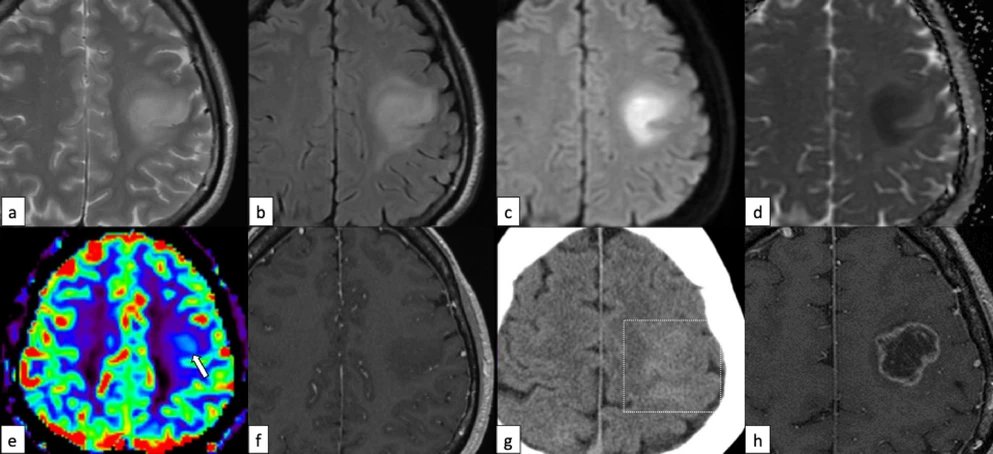
Hyperintense vessels seen on a FLAIR MRI scan are a marker of altered blood flow (hemodynamics), not a blood clot (thrombus).
*Proximal Indicators:
Serpiginous hyperintensities indicate slow forward blood flow or near occlusion of a vessel.
*Distal Indicators:
These signs suggest retrograde collateral blood flow in the penumbra territory.
*Clinical Significance:
In the early stroke window (<6 hours), these markers often represent viable penumbra; however, persistent markers may indicate ongoing occlusion and higher risk without reperfusion.
@WorldStrokeEd
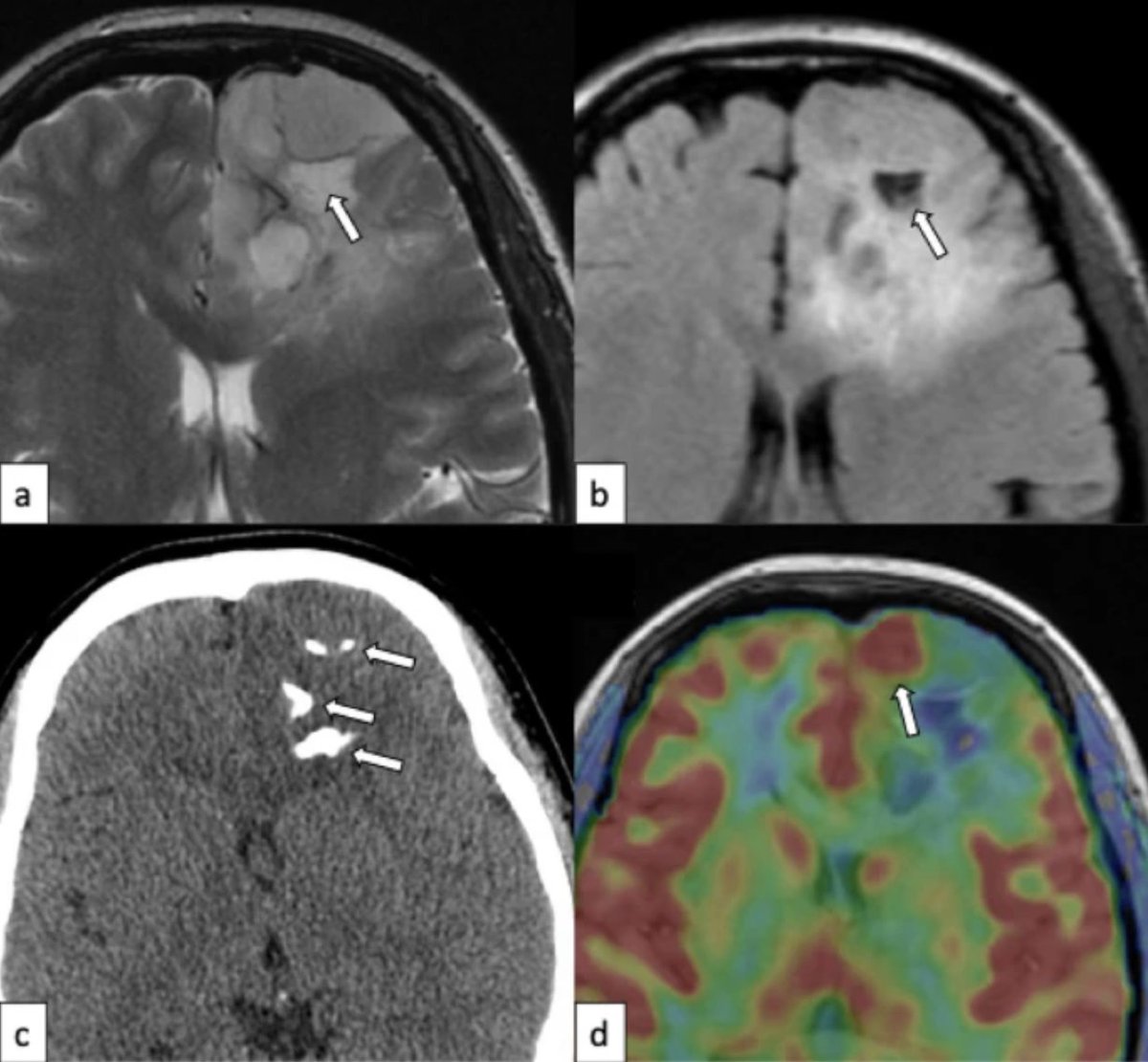
@samrad77@ongbenghooi1 This is especially true for deep (internal, subcortical) border zone infarcts, which are caused mainly by hemodynamic compromise (whereas superficial/external/cortical border zone infarcts per se are mainly associated to embolic mechanism). 👍🏼 paper -> https://t.co/UforRO0QUp
When deep (centrum semiovale) + cortical border zone infarcts coexist on the same side, the pattern strongly points to hemodynamic compromise, not embolic shower.
Check the ipsilateral vessels.
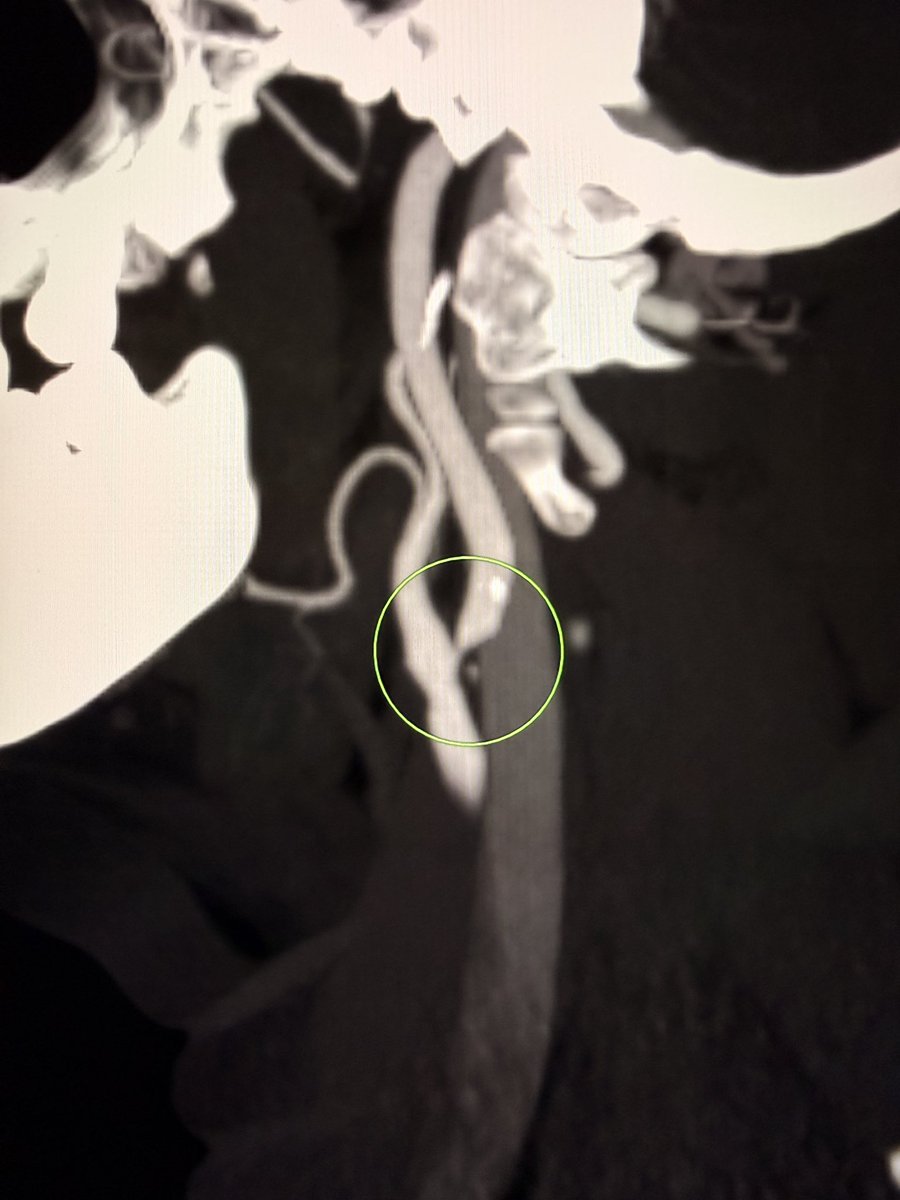
Look carefully at the carotid bifurcation and proximal ICA for high-grade stenosis.
In this case, the answer sat at the carotid bifurcation in the neck with high-grade stenosis. Intracranial vessels were clean.
Pitfall:
Labeling this as “embolic infarcts” and stopping there. You risk missing the real problem.
Wisdom:
Watershed pattern is a physiology clue. Follow it.
— Pearls, pitfalls and wisdom from Today’s reporting list
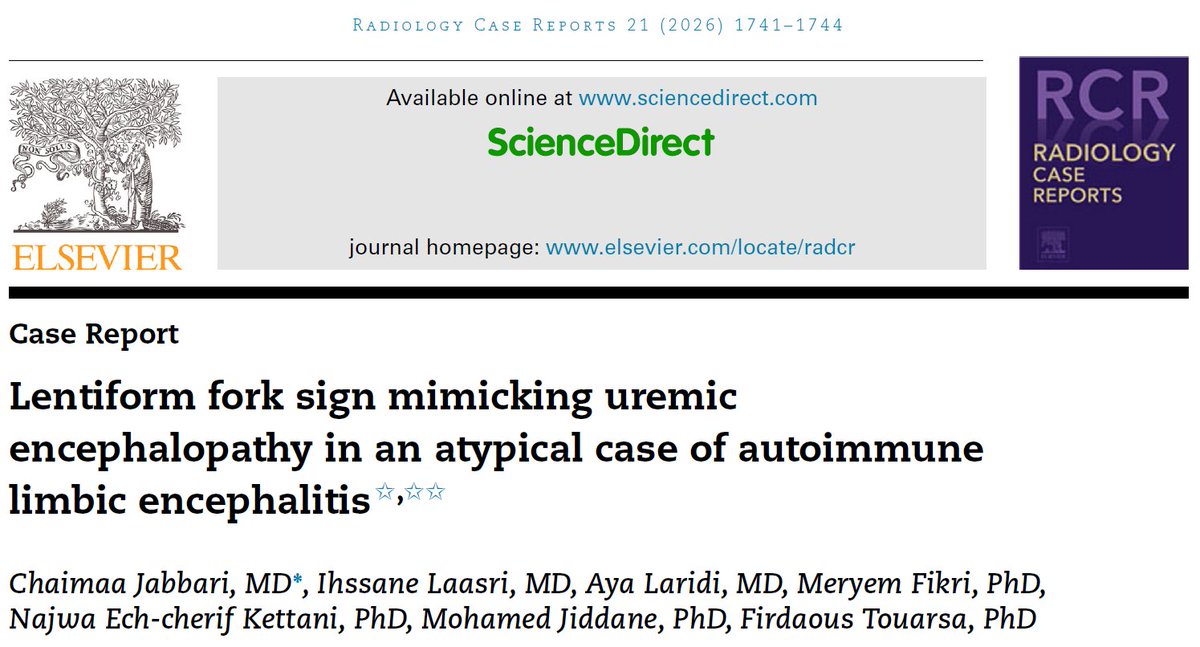
💡Lentiform fork sign on MRI typically points to uremic encephalopathy… but not always.
✅Normal renal function should raise suspicion. In this case, CSF revealed anti-NMDA receptor antibodies → autoimmune encephalitis.
https://t.co/gqKlIYOBZU
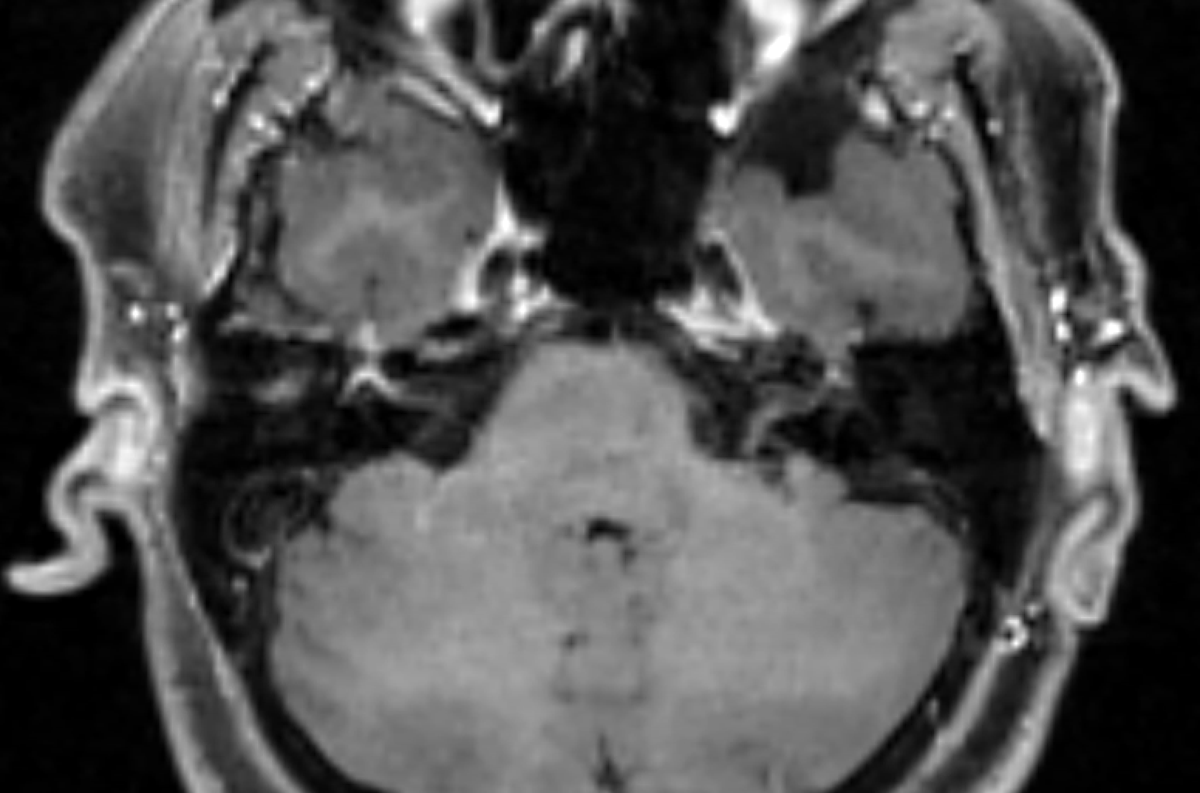
Lovely example of a right-sided Bell's palsy. Intense enhancement of the right fundal, labyrinthine, geniculate, and proximal tympanic segments of the right facial nerve (with the normal left facial nerve for comparison).
Remember that, contrary to traditional teaching, you can see mild enhancement of various facial nerve segments in normal patients. Asymmetry and intensity are clues that the enhancement might be pathological.
Recién salidas del horno: Guía AHA, 2026, de Evento Vascular Cerebral (EVC) Isquémico. Cambios o puntos relevantes:
🔴 Tenecteplase vs. Alteplase (Cambio Mayor) Se recomienda el uso de Tenecteplase (0.25 mg/kg, bolo único, máx. 25 mg) como una alternativa de primera línea, no inferior a la Alteplase, para pacientes elegibles en la ventana de 4.5 horas. Nota: La dosis de 0.4 mg/kg de Tenecteplase no se recomienda por falta de beneficio adicional y mayor riesgo de seguridad.
🔴 Ictus Leve No Incapacitante: En pacientes con déficits leves que no son incapacitantes (ej. síndrome sensitivo aislado, NIHSS bajo sin impacto funcional) dentro de las 4.5 horas, no se recomienda la trombolisis IV. Se prefiere la doble antiagregación plaquetaria (DAPT).
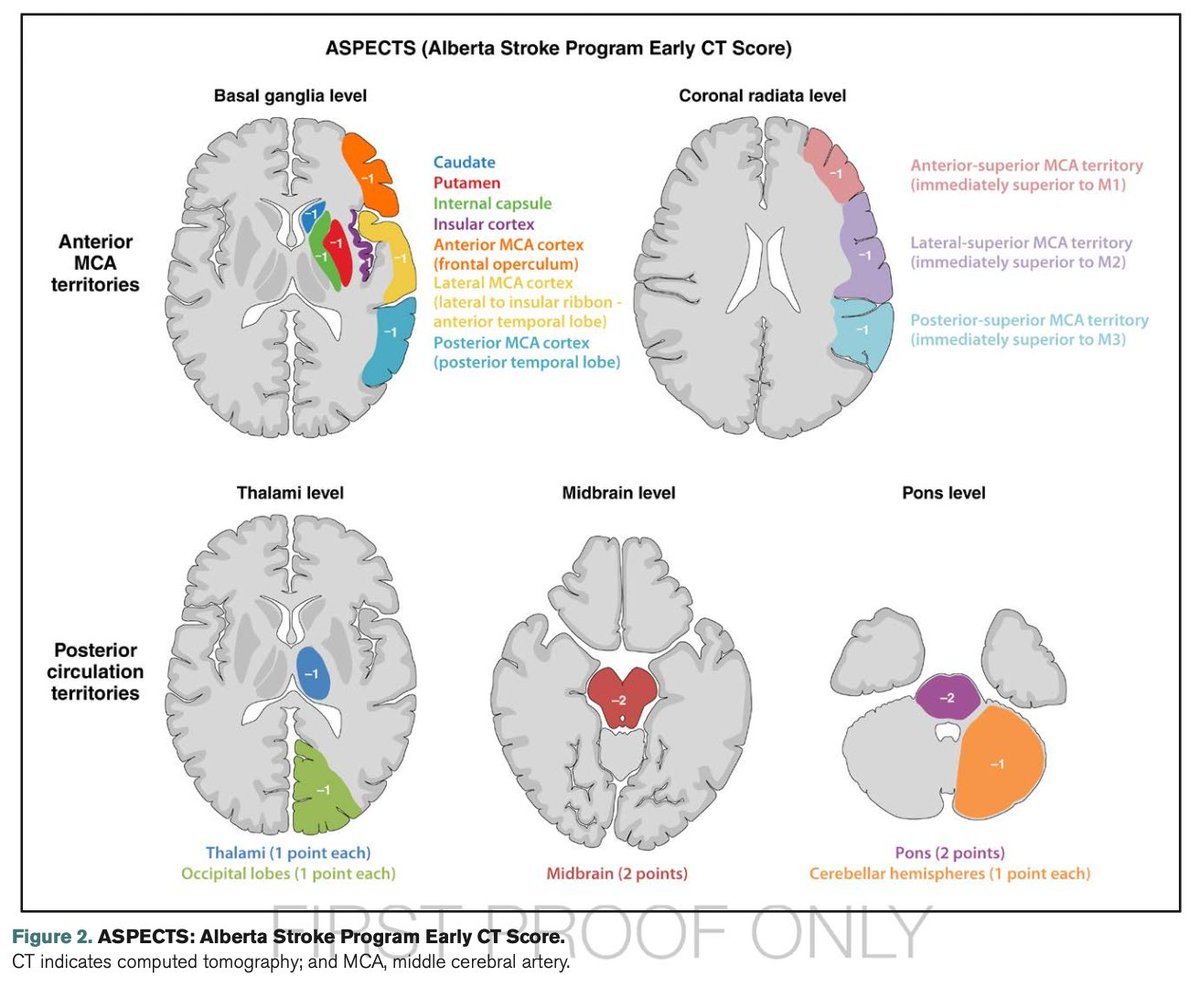
🔴 Trombectomía (EVT) en "Large Core": Se amplía la indicación de trombectomía mecánica para incluir pacientes con infartos de núcleo isquémico grande establecidos (ASPECTS 3-5), (antes eran excluidos).
🔴 Se desaconseja la reducción intensiva de la PAS (<140 mmHg) tras una reperfusión exitosa. Objetivo: TA <180/105 mmHg en las primeras 24 horas.
🔴 Oclusión de Arteria Basilar: realizar trombectomía en pacientes con oclusión de la arteria basilar a las <24 horas si NIHSS ≥10.
🔴 Control Glucémico: mantener entre 140-180 mg/dL.
🔴 Ventanas Extendidas de Trombolisis: Se recomienda el uso de trombolisis IV en ventana extendida (4.5 a 9 horas o ictus del despertar) en pacientes seleccionados mediante imagen avanzada que demuestre mismatch (DWI-FLAIR o Perfusión).
🔴 Nuevas Guías Pediátricas: Por primera vez se incluyen recomendaciones específicas para pediatría
Vamos a revisarlas a fondo para actualizar las apps.
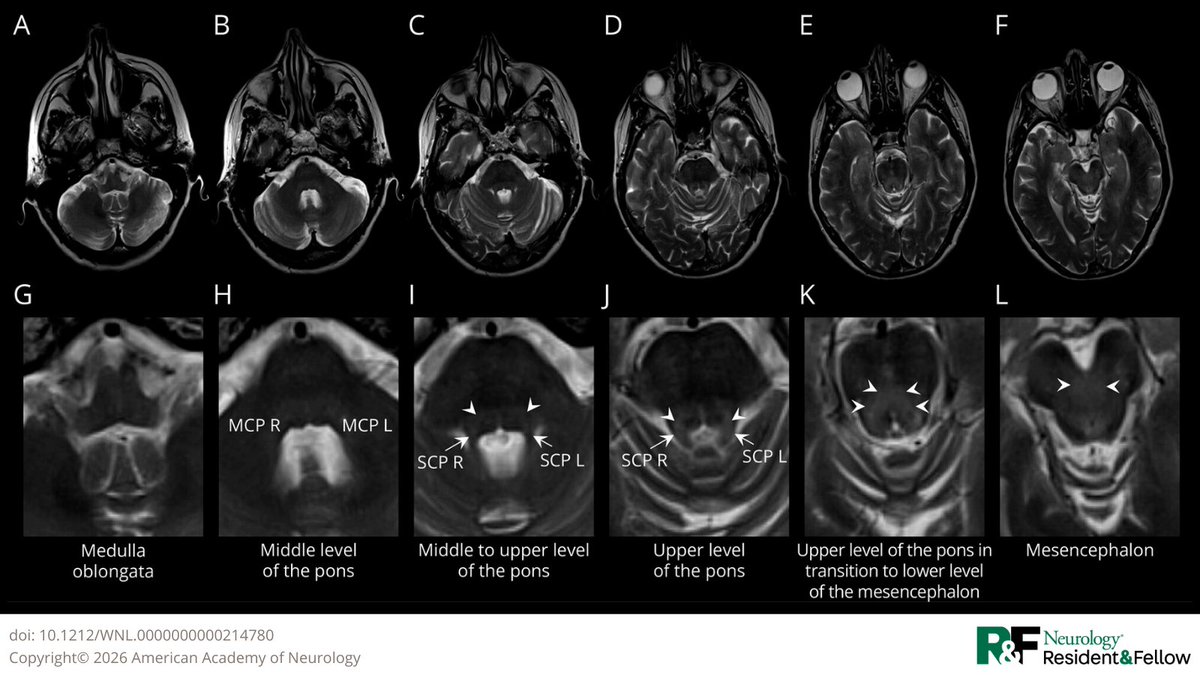
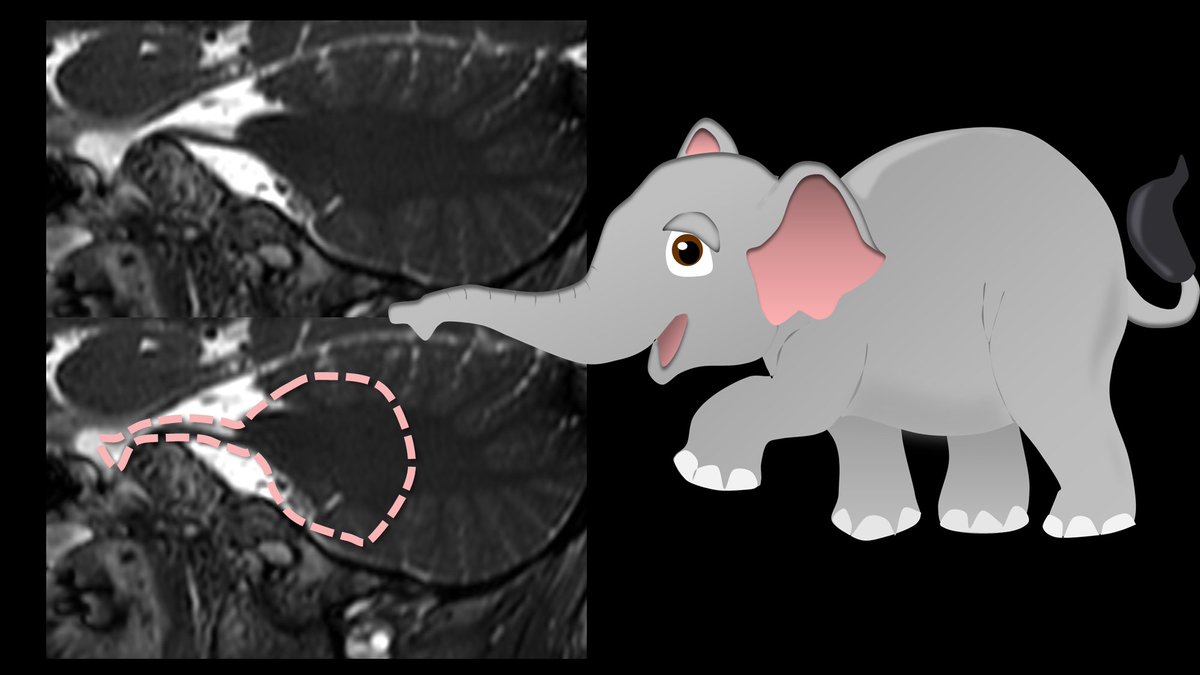
4/In the sagittal plane, the nerve looks like an elephant’s trunk coming out of the pons.
It should have a smooth curve up and over before it enters Meckel’s cave, just like the way an elephant’s trunk curves.
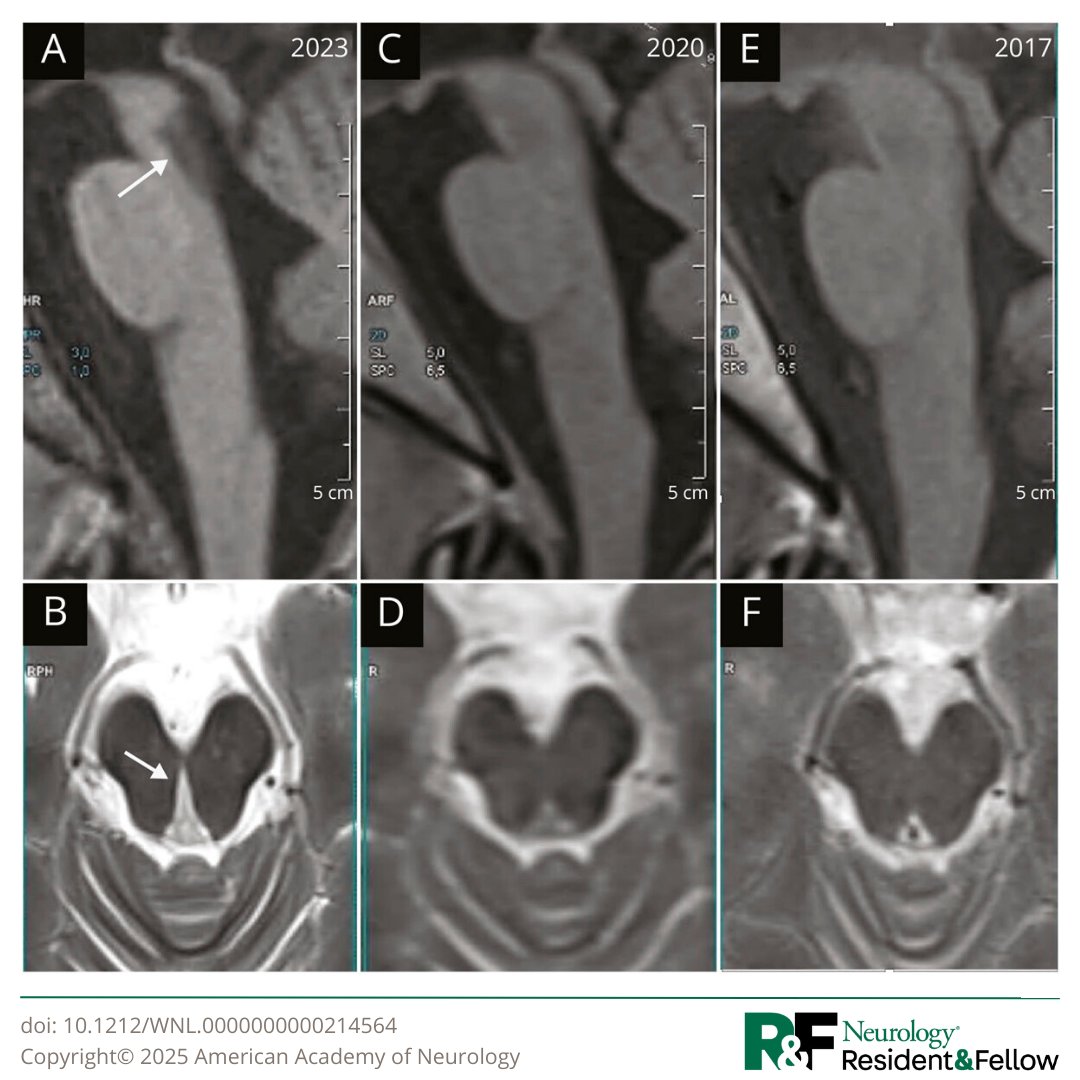
This Teaching NeuroImage case illustrates an acquired midbrain cleft in a professional boxer, believed to result from repetitive head trauma rather than a single high-intensity traumatic event: https://t.co/UsxxSUHb7C
#NeurologyRF@gmneurorx
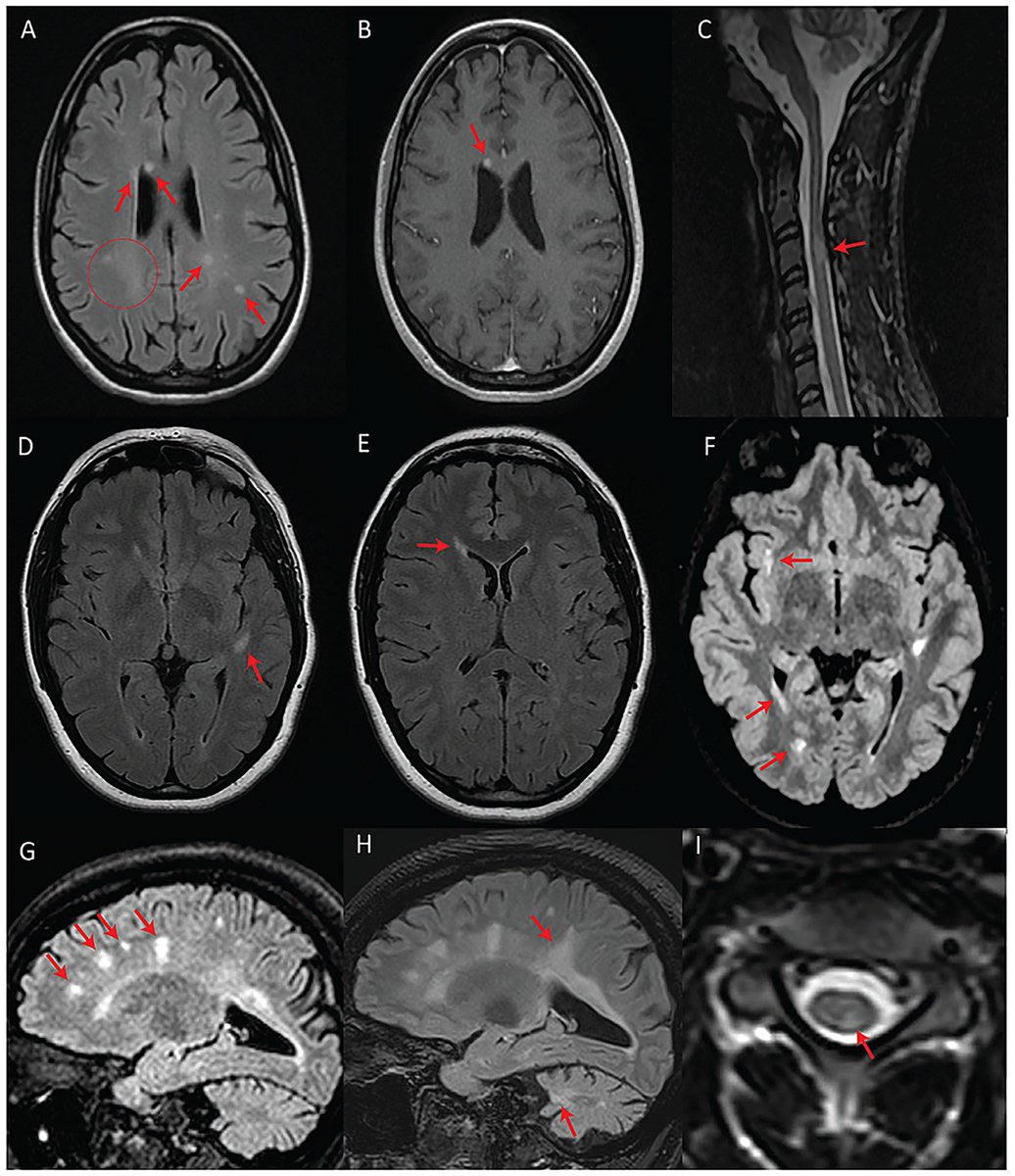
Are these MRI findings in people with multiple sclerosis? Shockingly, NO! They actually have Wolfram syndrome (WFS), a rare genetic disorder associated with pathogenic variants in WFS1 and is linked to optic atrophy, hearing loss and diabetes. https://t.co/d4CyBu23s7