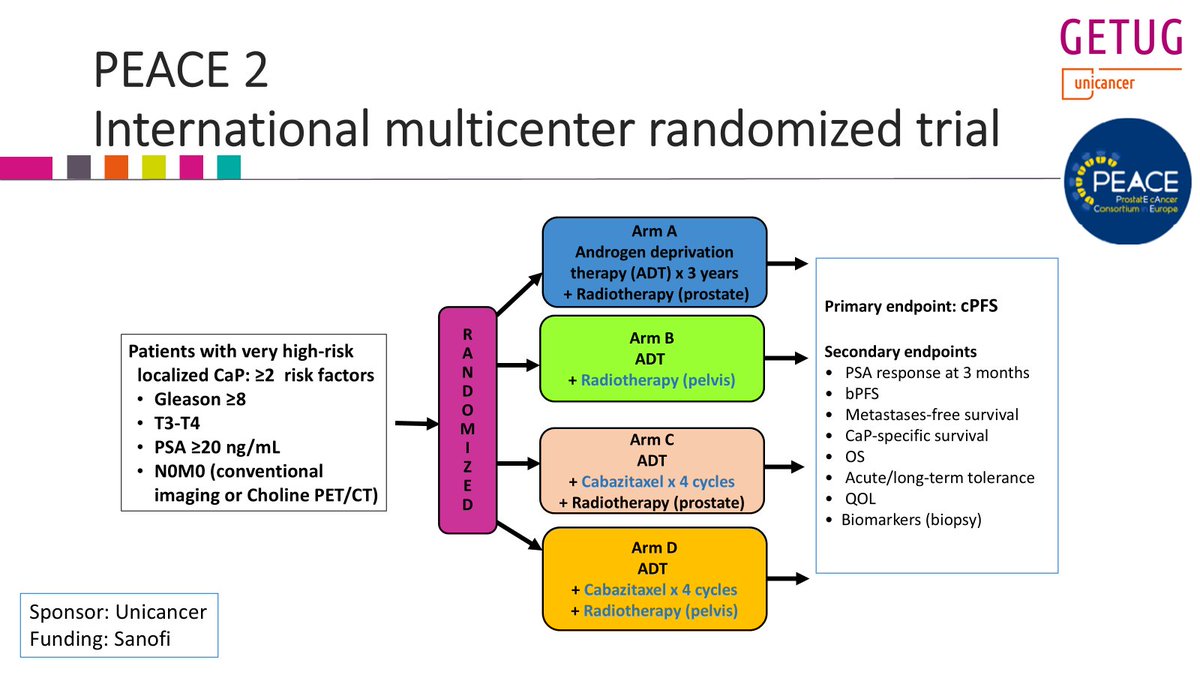
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n
Here is Version 2.0 of when to hold systemic tx during RT. Updated & w 3 additional drug categories (ADCs, CDK4/6 inhibitors, PARPi).
More details on newer drugs in 🧵 below.
Please use this version as reference & thanks for all input/experience crowdsourcing! (1/3)
Presented at #ASCO25:
A 3-year structured exercise program after adjuvant chemotherapy for colon cancer improved disease-free and overall survival, physical functioning, and fitness, as compared with health education alone. Full CHALLENGE phase 3 trial results: https://t.co/j3kWJDjuVz
@ASCO
The most practice changing trial from #ASCO25 is now live on @NEJM .If this was a drug, this would be approved today. Globally relevant and low-cost intervention that is not only delaying relapse but actually improving survival.
Perfect case example of a #cancergroundshot trial.
https://t.co/ZnqeplJ7IA
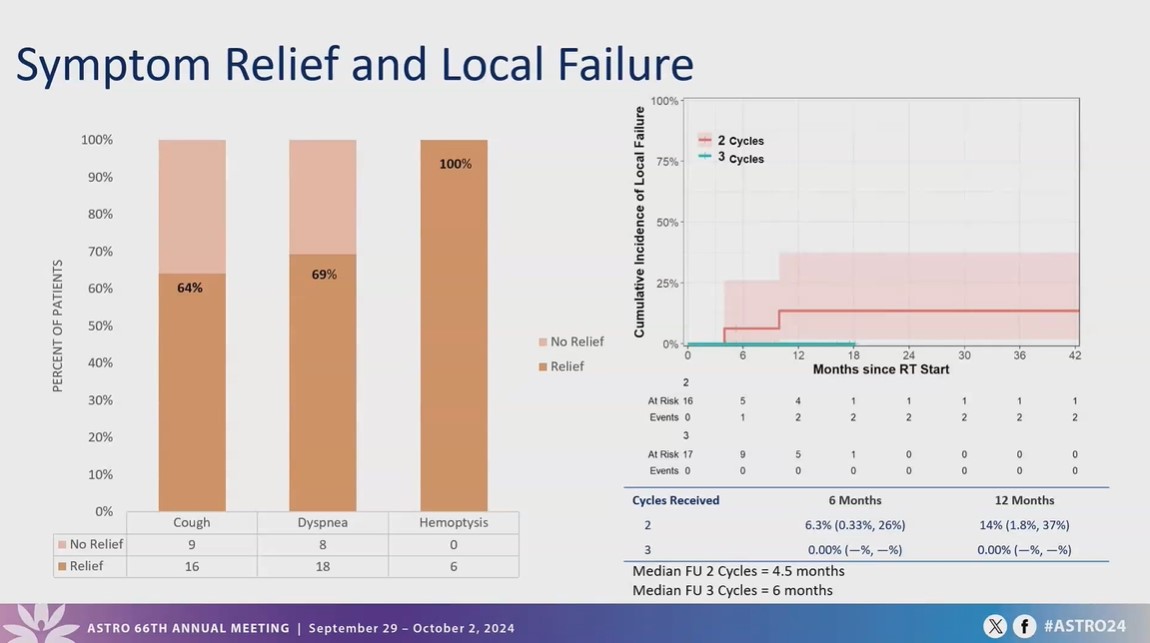
Can QUAD be used for thoracic tumours?
🟰YES!
➡️ 3 cycles of quad shot is safe and feasible with concurrent systemic therapy for centrally located thoracic tumours
➡️Limited grade 3 toxicities
➡️ Majority of patients experienced symptom relief as measured by PROs
#ASTRO24
Are you a PGY4/5? We invite you to apply for our 300in10, 2-month fellowship program focusing on advancing #brachy. This is an opportunity to immerse yourself in a community committed to training competent brachytherapists. https://t.co/x3ufmtPxKe @AndrewFarach@daniel_petereit
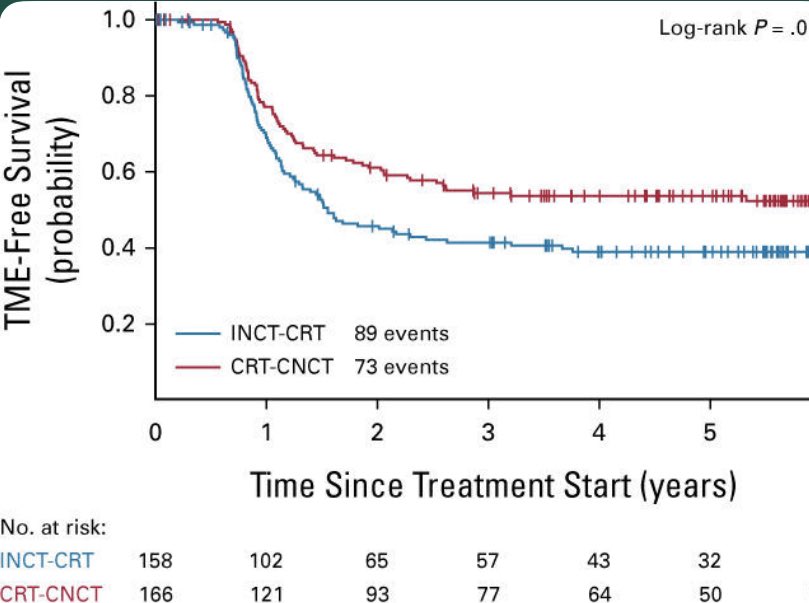
🎙️ OPRA updated analysis confirms the long-term organ preservation with total neoadjuvant therapy for #rectalcancer ‼️@OncoAlert@ASCO
📌Ph2 trial w/ 👥random to induction CTH followed by CRT (INCT-CRT) or vice versa
- Complete/near-complete responders were offered WW, incomplete responders ➡️🔪
🥇🎯: DFS. 🥈 🎯: TME-free survival
📊RESULTS
-324 👥, median FU 5.1 y
- 5-y DFS rates: INCT-CRT 71%, CRT-CNCT 69% (no sig)
- TME-free survival: INCT-CRT 39%, CRT-CNCT 54% (P = .012)
- 94% of regrowth within 2 y, 99% within 3 y
- DFS similar for TME post-restaging and WW followed by TME post-regrowth (both 64%, N🚫 sig)
#radonc https://t.co/mD3wkwU6ih
Grateful for our work examining the success of peer-to-peer authorization strategies highlighting @NCCN guideline-cited Level 1 evidence in reversing insurance denials for spine #SBRT being published in @AJCOonline! #KillCancer#FixPriorAuth#SPORTSMEN
https://t.co/7T2Lgbmcju
IMPORT 10y:
Late normal tissue effects at 10y ~5% in PBI arm vs ~30%(!!!!) in whole breast arm, and local control "better" with partial breast(!)
Frankly, whole breast radiotherapy is the *wrong* tx for older women w/ early, low risk #breastcancer
https://t.co/fbD56Jm03y
This is hugely important for our patients in making an informed decision about adjuvant treatments -- particularly as we enter #BreastCancerAwarenessMonth ! Fully agree RT alone (particularly #APBI) should be discussed alongside single modality endocrine therapy
This #ASTRO2023 presentation was one of the most important for our specialty. Tumor boards are recommending adjuvant endocrine therapy alone after surgery, but rarely RT-alone. Low-risk breast cancer is one of the most common things we treat. We need better advocacy for RT.
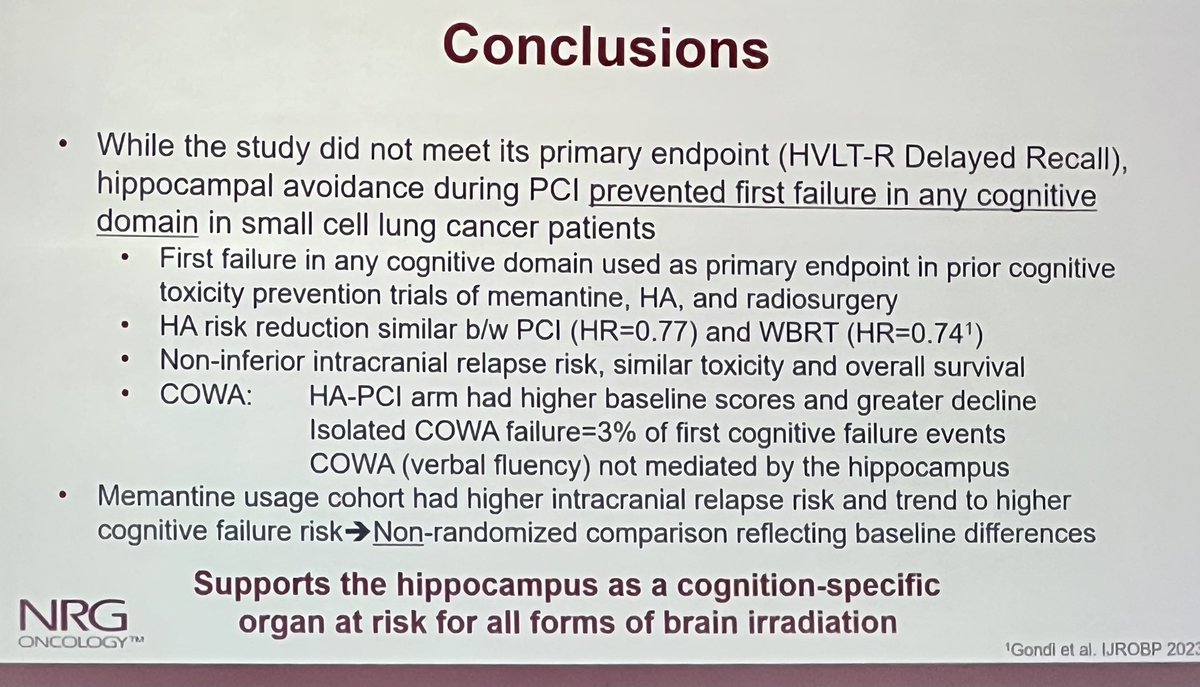
💥First plenary #ASTRO23@vinaigondi presented PCI +/- hippocampal avoidance for small cell lung cancer. 🧠
⭐️HVLT-R no different (primary end point)
⭐️Did reduce first failure in any cognitive test (2nd endpoint)
⭐️No diff in intracranial failure 👏