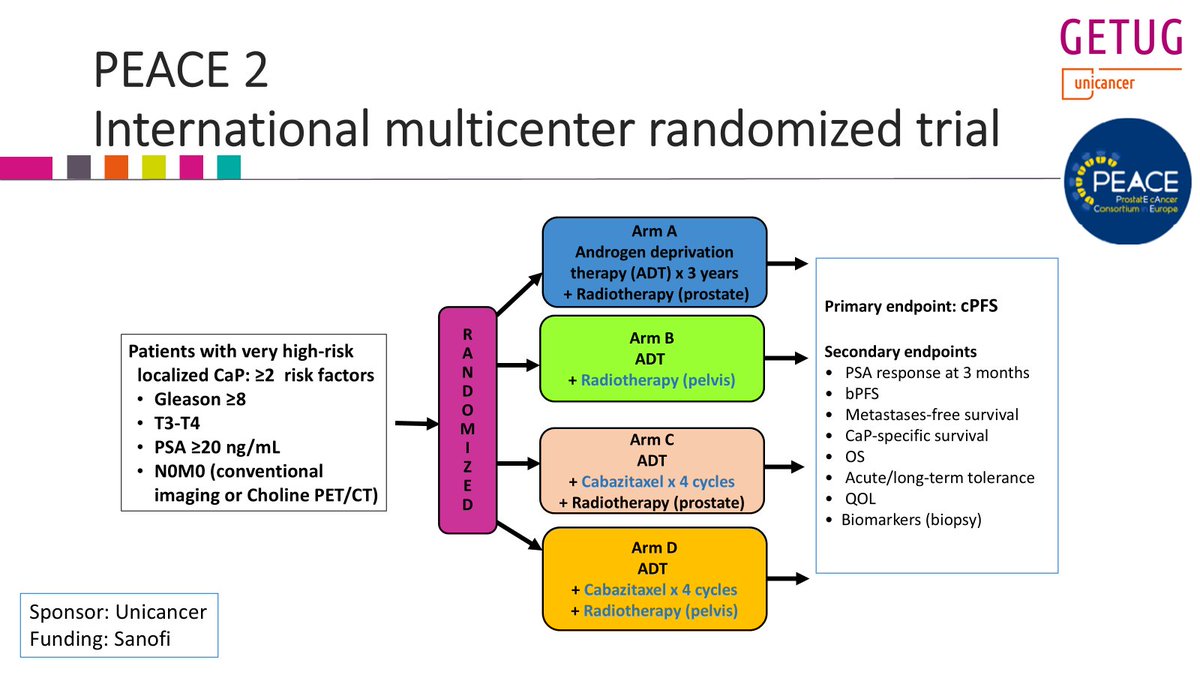
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
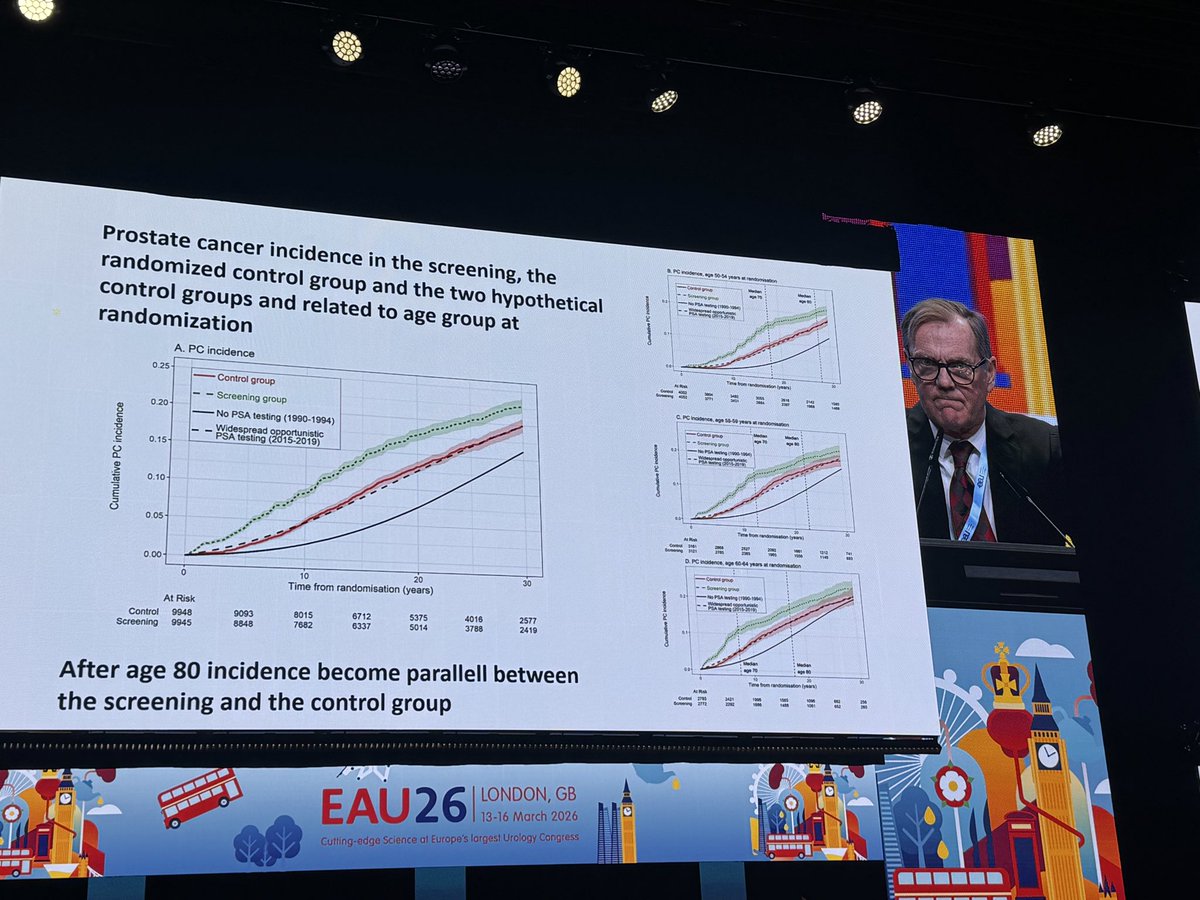
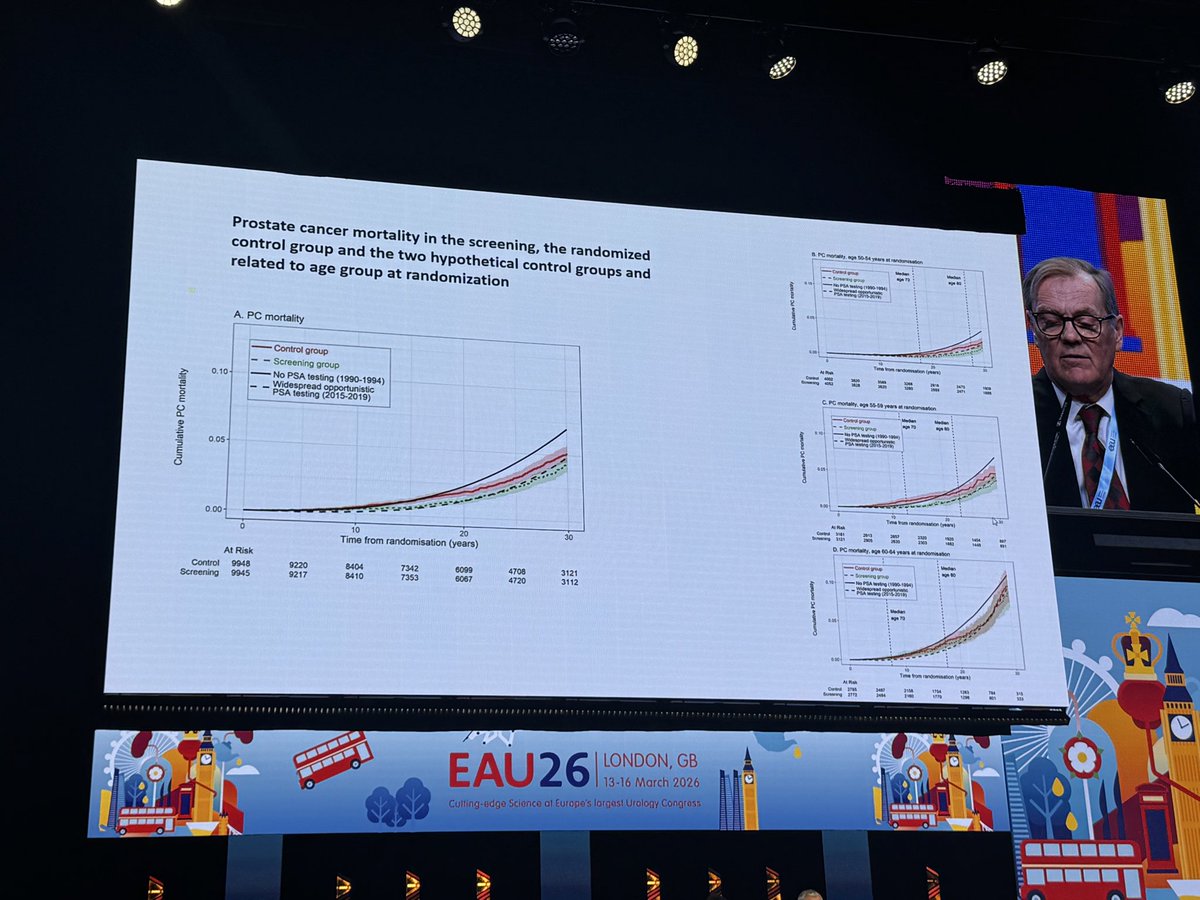
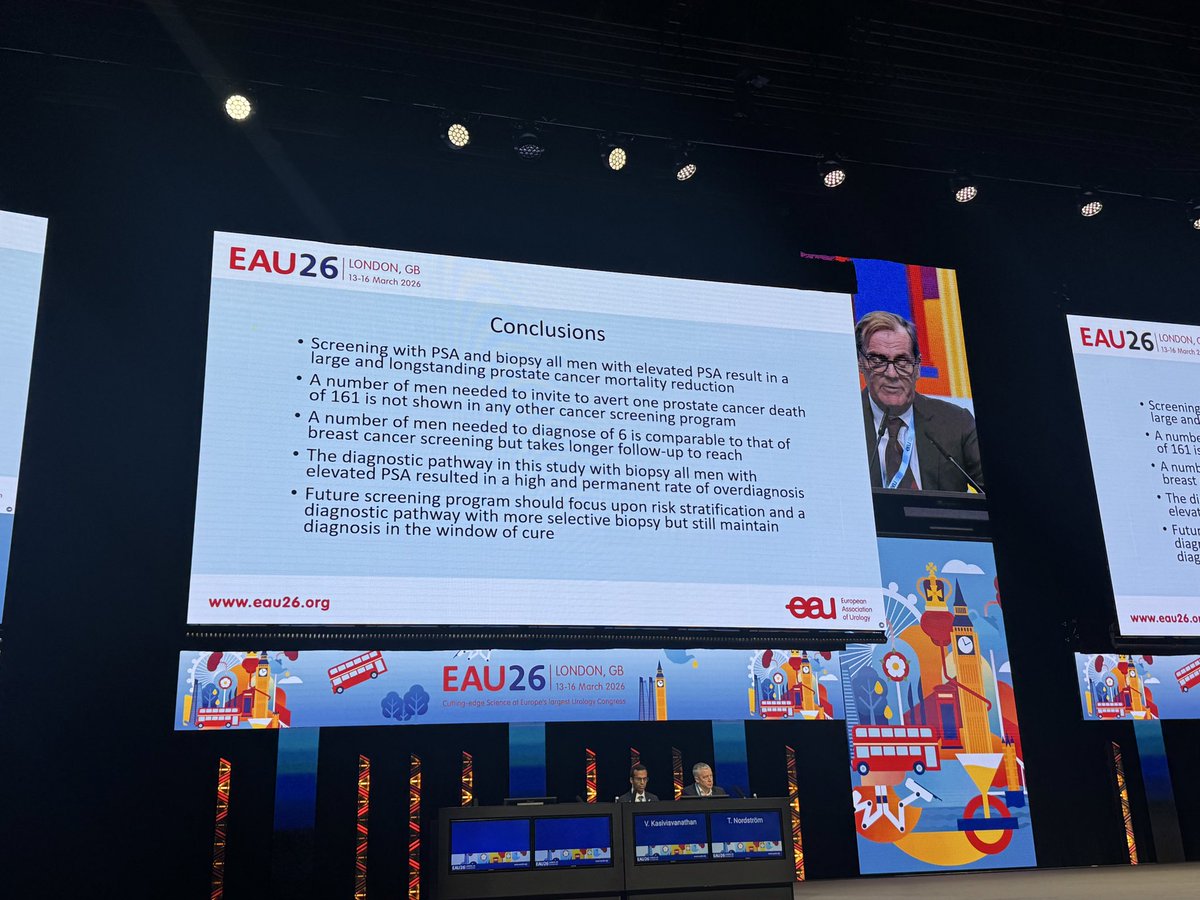
Prof Hugosson: Göteborg trial with 30 year outcomes! NND falls to -6-, with greatest benefit for men 50-59 at randomization. Despite no image guidance, high overdx, and suboptimal tx. Best evidence we have re: the evidence for #prostatecancer screening. Get tested! #eau26@uroweb
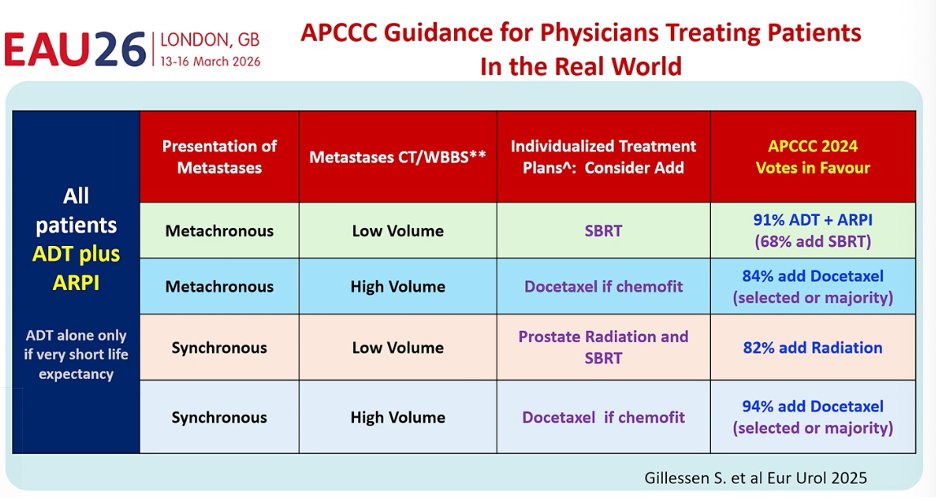
#EAU26@ChrisSweens1: the field is reaching a consensus in mHSPC.
ADT + ARPI for nearly all patients, then personalize intensification:
• SBRT for low-volume
• Prostate RT in synchronous disease
• Docetaxel if high-volume and chemofit
🕒 The hope for the future: biomarkers to guide therapy, global access, and drug prices coming down so evidence-based care becomes feasible worldwide.
@uroweb@UroToday
@tompowles1@weoncologists@Uromigos@kalasri3 Thanks for the shoutout Tom.
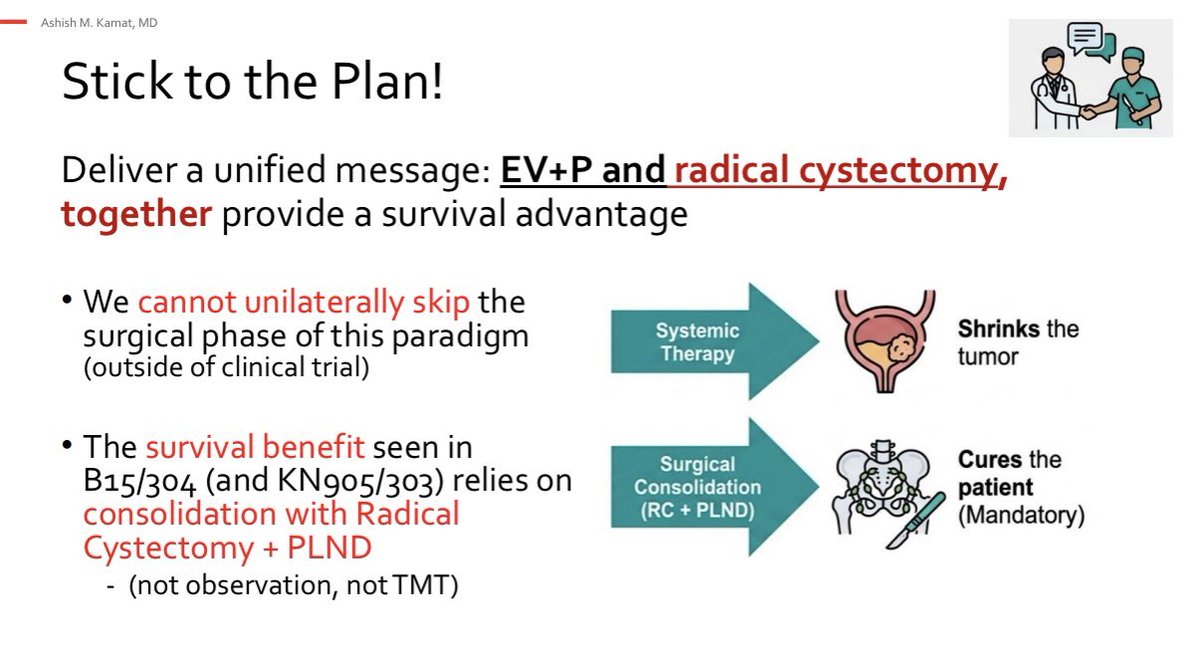
We need to help our patients and deliver a unified message:
The OS advantage seen with EV+P
relies on consolidation with Radical
Cystectomy + PLND
(not observation, not TMT)
#EAU26
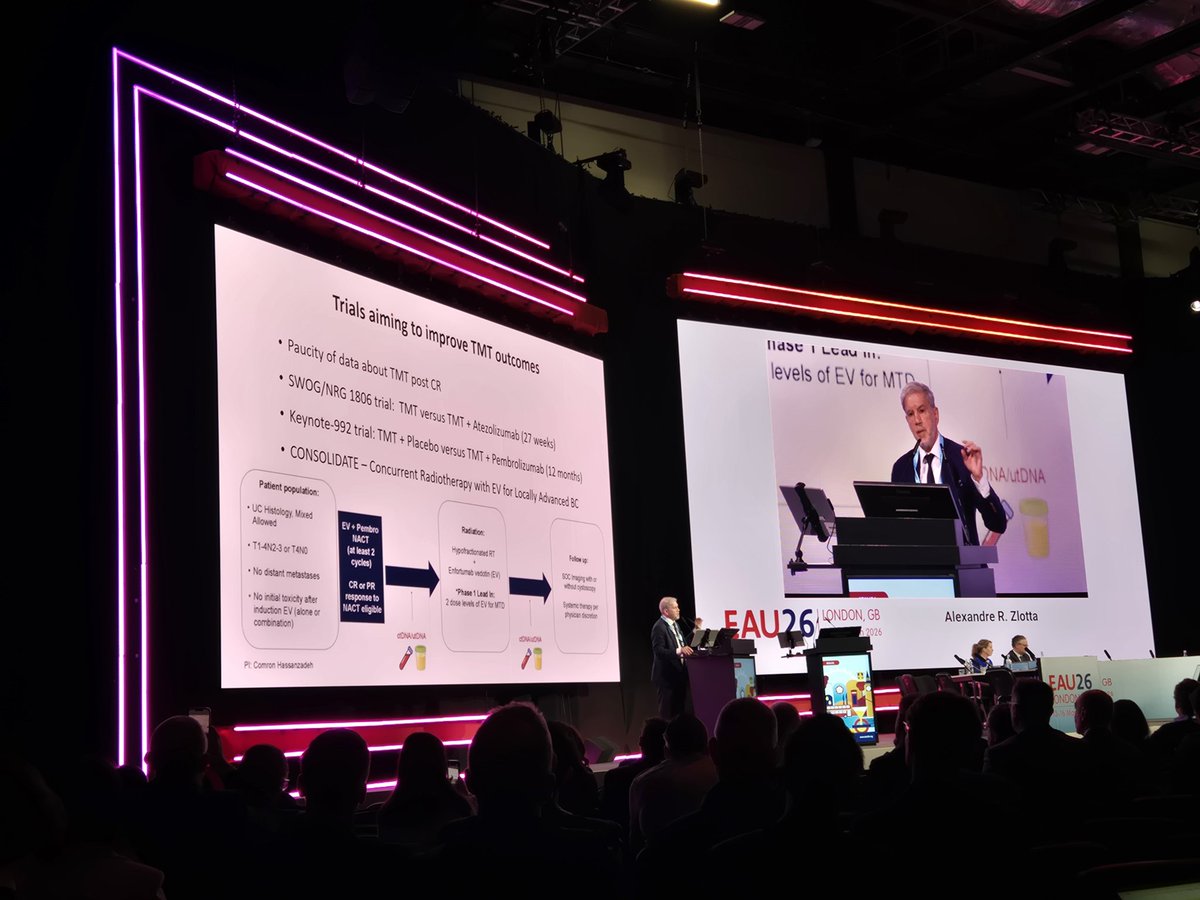
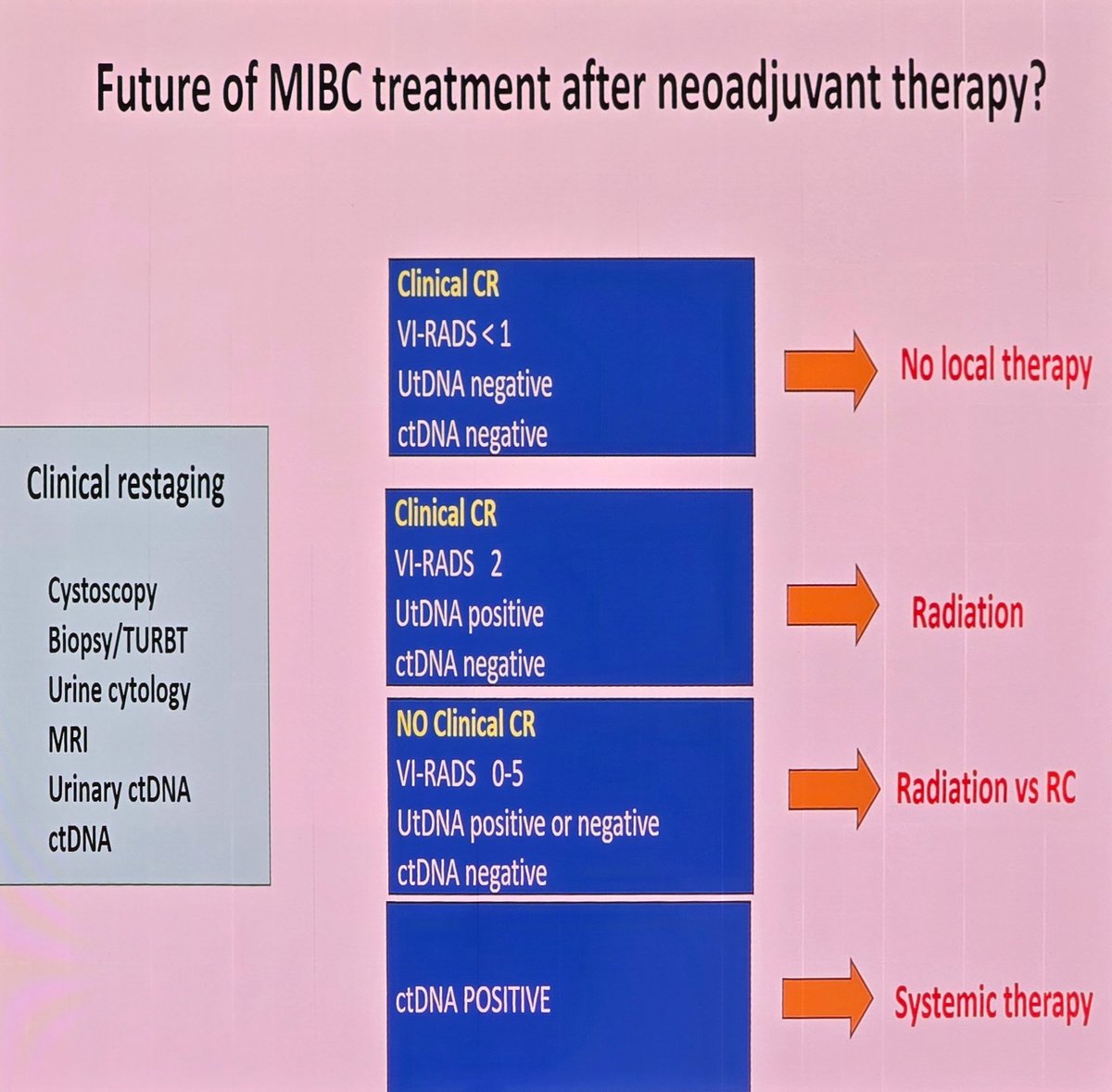
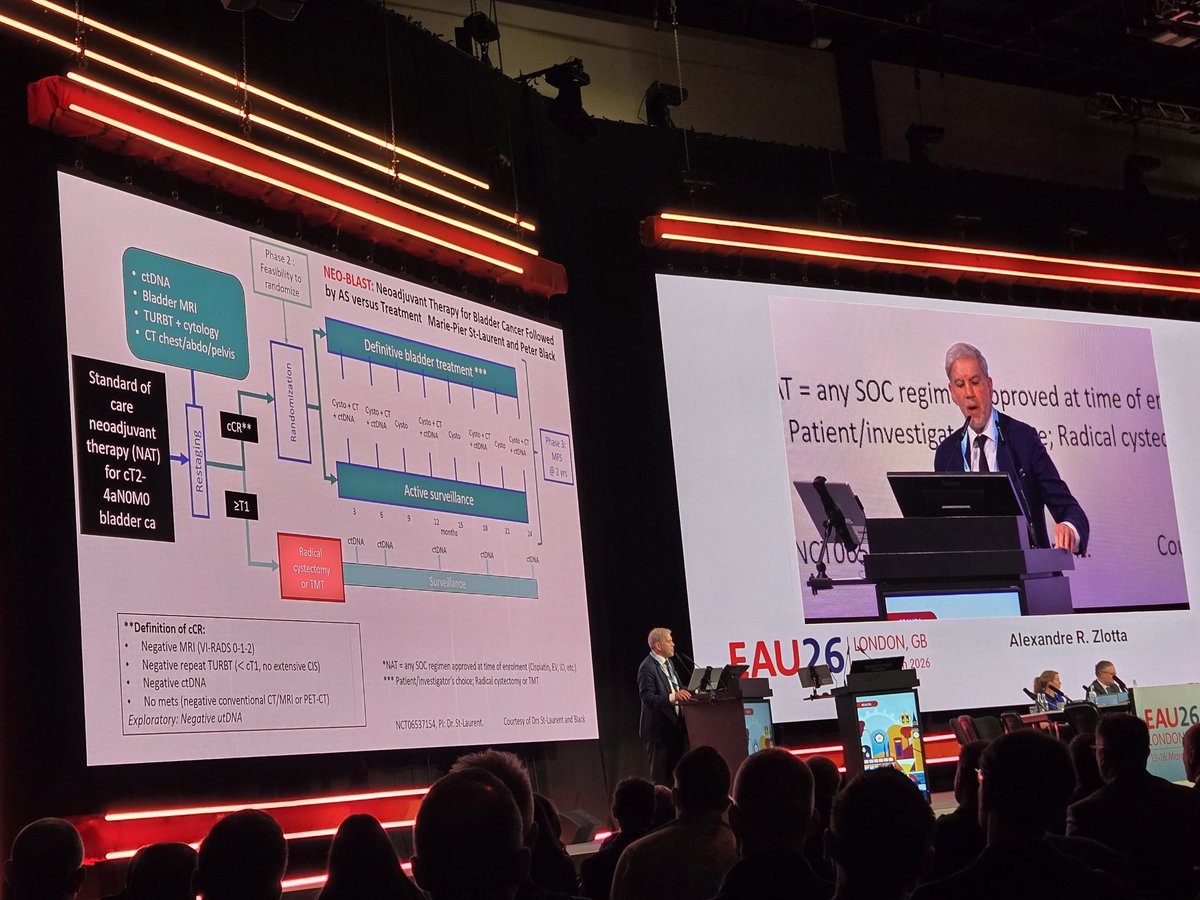
"Who needs surgery after neoadj chemo" plenary by Dr. Zlotta #EAU26
- pCR now >50% w/ EV+P regardless of cis-eligibility
- Predicting pT0 remains a challenge
- Future of MIBC tx will need multi-modal, risk-adapted approach (🔊 NEO-BLAST trial led by @MariePierStLau1@pcvblack)
Meta-analysis in HR-NMIBC: intraves Gem/Doce showed 24-mo RFS of 78% (BCG-naïve) and 41% (BCG-exposed/unresponsive); PFS 97% & 85%. No significant RFS difference vs BCG in comparative BCG-naïve cohorts🔗https://t.co/4DVO22nt2T @Pietro9609@UroMoschini@BenjaminPradere@SBoorjian
3 studies testing Perioperative immune bases therapy (EVP or Gem/Cis/Durva) in muscle invasive bladder all have shown an OS advantage vs standard of care. KN905 (EVP) is distinct in that it’s in a cisplatin ineligible population (accounting for the poor performance of the control arm). It’s also a smaller trial. The control arm of KN-B15 performed slightly better than NIAGARA (Gem/cis for both), but the trials are otherwise similar. The pCR in the EVP trails and the consistent efficacy of EVP is striking. #GU26
IT IS THIS TIME OF THE YEAR AGAIN!
TOP 10 GU clinical trials in 2025!
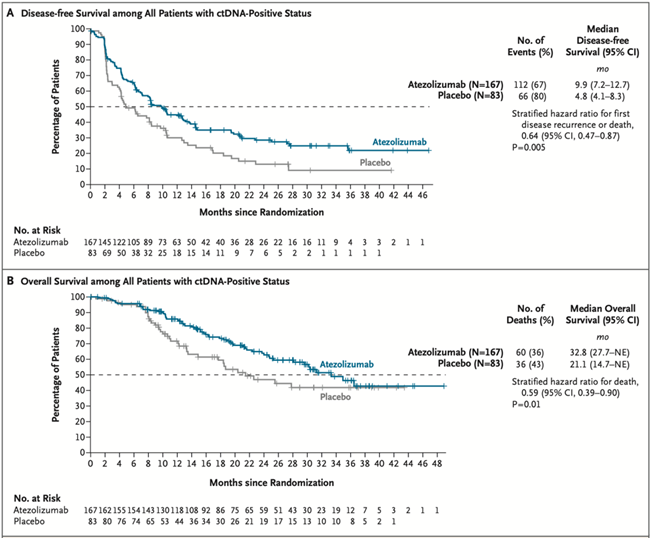
1/ Practice-changing IMvigor011: In ctDNA+ MIBC post-cystectomy, adjuvant atezo improved DFS (HR 0.64) & OS (HR 0.59) vs placebo. ctDNA- pts spared therapy w/ 2-yr DFS ~88%.
@tompowles1@DrYukselUrun@OncoBellmunt@NEJM #ESMO2025 Plenary @myESMO
https://t.co/mbl2VKLZ2N
1/ Ze zetten in tijden van digitalisering en algoritmes hun stempel naast de stempel van het RIZIV.
2/ Ze beweren fouten bij afrekeningen te corrigeren maar zijn tegelijk de grootste ziekteverzekeraars van het land. Ze zijn stroper en boswachter tegelijk. Ze bieden allerlei diensten aan die ver buiten hun oorspronkelijke doelstellingen vallen, van verzekeringen en vakanties tot kortingsbonnen, die in een volwassen dienstenmarkt goedkoper en beter worden ingevuld.
3/ Er zijn naar schatting 1100 kantoren in België, elk met hun eigen gebouw, hiërarchie, IT-infrastructuur, koffiezetapparaat, bedrijfsauto's, maaltijdcheques, cv-ketel en poetshulp. Het "belang van hun klanten" is al opgesoupeerd voordat ze de drempel hebben overschreden.
Last week at #ERUS2025, @minerviniandre convinced me to give the stentless #FloRIN neobladder a go. Thanks to his tips & tricks the #neobladder part took just under 3 hours and went super smoothly. Thanks Andrea!
New EUPlatinum Opin. in European Urology:
IDC & cribriform PCa = high-risk, underdetected, poorly reproducible. Time to rethink grading, imaging, and surveillance.
📄 https://t.co/w3lBnHIFu5
#ProstateCancer#UroPath#EurUrol
Of het over corona, klimaatverandering of oorlog in het Midden-Oosten ging of gaat, geleidelijk kregen of krijgen we een narratief opgedrongen dat de ruimte voor nuance almaar verkleint en zelfs iemand met een licht afwijkende mening moreel veroordeelt. Een gevaarlijke trend.
@terzaketv@m2matthijs@CoolsKat Triest dat er geen dialoog kan zijn. Hij weet dat ie daar de argumenten niet voor heeft... En dat is net wat hem kwalijk genomen wordt, dat autoritaire, belerend..
@IveMarx Op dit moment wordt de innovatie in de ziekenhuizen grotendeels gedragen vanuit de supplementenpot... Denk aan dure robots en andere toestellen bvb. Daar is meestal geen vergoeding voor opgenomen in de riziv vergoeding. Wél een bewezen voordeel voor de patiënt..
NIAGARA’s surgical safety results #EAU25 with Jim Catto. Results show the addition of duvalumab to neoadjuvant platinum chemotherapy did not increase surgical complications or cystectomy rates.