Cardiology Pharmacist - CVRM | Honorary Lecturer | Coffee & Chocolate Connoisseur | Enjoy watching cars race and people hit a green fluffy ball back and forth
Tl:dr version: giving MDs financial bonuses for controlling their patients’ blood pressure paradoxically worsened blood pressure treatment because incentivized doctors were more likely to re-measure elevated BP until “normal” (rather than treat), resulting in many more strokes.
I wouldn't call 23% a miss.
SURMOUNT-1 data reminds us that tirzepatide did not work for weight loss in ~10% of people.
All of my patients who didn't see significant #weightloss with tirzepatide will be trialed on CagriSema. Amylin introduces a different mechanism.
The differentiation here will unmask the heterogeneity of #obesity
This is so incredibly dangerous and will be seen by millions of people.
I'm a cardiologist who opens the arteries of people with heart attacks.
1. Secondary vs primary prevention - Here, Malhotra is talking about someone taking a statin who has *already had a heart attack*.
First of all, if you survive a heart attack without any major damage, you're lucky. A lot of people aren't as lucky. I know this because I do this work for a living.
Primary prevention is for people who've never had any clinical event. If you've had a heart attack, you are NOT THE SAME as someone your same age, etc who has NOT had one. The game is changed and much riskier for you. You are at a HIGHER RISK of ANOTHER heart attack. You need to be MORE AGGRESSIVE to lower that risk. If your first one spared your life, the second one might not. That is secondary prevention.
2. "Benefit over 5 years" - This is such a classic, silly misinformation trick. OK sure - but that assumes you're only planning on living another 5 years and then are ok with just dying.
That's obviously absurd and I don't believe anyone agrees with that. As your cardiologist, I'm not trying to keep you alive and well for just 5 years. I'm talking 10, 20, 30 years, decades.
The real true benefit of statin therapy is over decades. As in, they help keep you alive longer. You can't just measure it at an arbitrary 5 year cut off.
3. Not magic bullet - Prevention is not just statins. It is changing your entire lifestyle, diet, exercise, etc, and meds. Statins are not magic either. People on statins have heart attacks too.
But life is about risks and probabilities. You do what you can to reduce risk as much as possible. You cannot reduce risk to 0, but you can bring it pretty damn close to 0.
It is so fascinating to me that there are so many highly intelligent and accomplished people who have an intimate understanding of risk and probabilities, and who make major decisions in their daily lives based on this understanding. But when it comes to statins and vaccines, they just abandon all logic.
🚨 Nicotine is a cardiovascular toxin — regardless of delivery system.
A new expert consensus outlines 12 evidence-based messages showing that cigarettes, e-cigs, heated tobacco & nicotine pouches all harm vascular and metabolic health 🫀⚠️
👶 Alarmingly, flavoured products and aggressive marketing are driving a paediatric addiction crisis, fuelled by the myth of “safer nicotine.”
📜 The paper calls for comprehensive regulation: advertising bans, flavour restrictions & indoor-use prohibitions-across all nicotine products.
https://t.co/CikJyAB3zj
@DHSCgovuk
New @TheLancet Meta-Analysis by #NelsonWang@BrighamWomens HF Fellow
What is the expected BP lowering with various antihypertensive regimens?
Robust model derived from n=104,176 pts across 484 RCTs
Terrific user-friendly tool: https://t.co/jaWeX3V1fn
https://t.co/rdHV0EkEeF
Fantastic result for obicetrapib which reduced CV events at 12 months in a phase3a trial
we have another tool in our war against CV disease coming 🤞🏻
⭐️ Well done @ProfSNicholls@JohnKastelein@ProfKausikRay ⭐️
Let’s see what the Prevail trial shows
https://t.co/VrtrlT7wM1
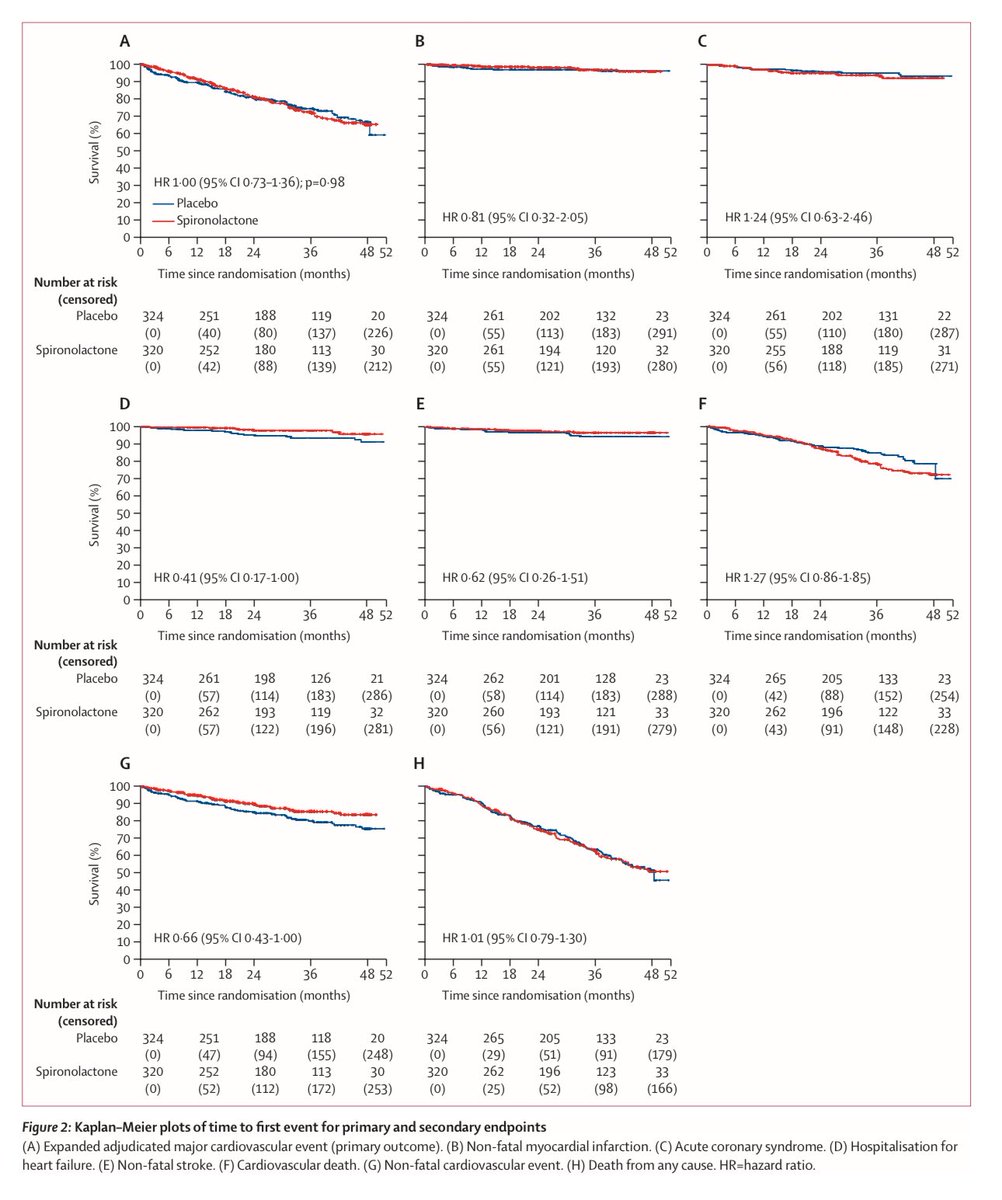
ALCHEMIST & ACHIEVE in @TheLancet this week
Spironolactone does not reduce cardiovascular morbidity / mortality in hemodialysis patients
Huge congrats to Mike Walsh, Patrick Rossignol & all involved
https://t.co/iL9myhNXWt
https://t.co/1tK6IfLydt
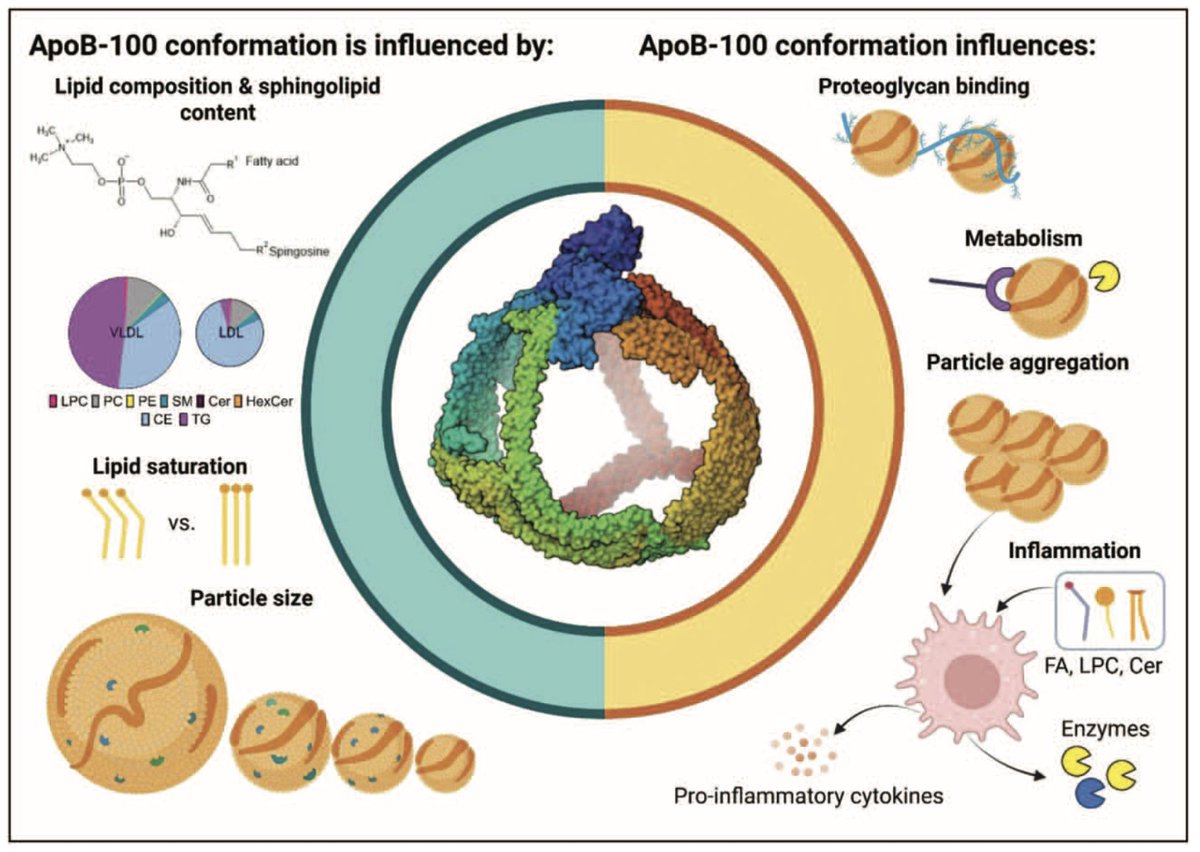
🧬 ApoB Conformation and LDL Atherogenicity
👉This paper delves into how specific conformational changes in apolipoprotein B-100 impact LDL particle behavior — particularly its binding affinity to arterial wall proteoglycans. These structural transitions increase LDL retention in the subendothelial space, accelerating atherogenesis independently of cholesterol content.
👉The study underscores that ApoB’s spatial conformation, not just its presence, is critical in mediating LDL particle pathogenicity.
☝️Implication: Advanced lipid profiling should move beyond simple concentration metrics — structural-functional assessments of ApoB may open new frontiers in cardiovascular risk stratification.
📌 Bottom line: not all LDL particles are created equal — shape also matters.
🔗 A must-read for anyone who still thinks "LDL is just cholesterol." https://t.co/aqRSC0GkBN
@society_eas@CO_Lipidology
"The @NHSEngland interim guidance re 'Weight loss drugs' will leave primary care clinicians in the lurch.
Because only a fraction of the population will be eligible, it will fall on clinicians to explain this “rationing.”"
Via @bmj_latest
cc @GilesYeo
https://t.co/uQe6R0nRpY
🚨 What’s the best diet for long-term health?
There’s no single “best” diet —> but there are evidence-based principles that promote optimal health. 👍🏼
This post focuses on cardiovascular health - the leading cause of death globally: 🫀🧵
New study result 🚨
Tirzepatide vs semaglutide SURMOUNT 5 RCT
📉Total body weight loss:
−20.2% with tirzepatide
−13.7% with semaglutide
🤢Discontinuations due to gastrointestinal events: tirzepatide 2.7%, semaglutide 5.6%
🤮vomiting tirzepatide 15.0% vs semaglutide 21.3%
https://t.co/4TwFLgWBOq
Whilst we wait for the results of the inclisiran CVOTs this analysis led by Benoit Arsenault using instrument variables to mimic hepatic and circulating pcsk9 suggests it’s all proportional to atherogenic lipid change #hope
https://t.co/fYmR9Bwx3z
If anyone believes they can keep a lid on the use of GLP-1 analogue medicines for weight loss in the #NHS?
They just need to see the signs all around
People are choosing to avoid the “standard” means
The #NHS would be better off trying to ensure safety measures are in place
Rather than futile attempts to restrict access with words like “wraparound care”
@DrSdeG@FionaQuigs
https://t.co/gYIbm5ri7J
🚨 When ‘high LDL causes heart disease’ becomes controversial, you know science is in trouble.
The evidence showing that lifelong LDL exposure causes heart disease is arguably the strongest evidence base we have in all of medicine.
🚨 We have just published our commentary on the KETO CTA study! 🔥
Abstract as follows:
“A recent study by Soto Mota et al. @nicknorwitz@realDaveFeldman@AdrianSotoMota has generated widespread attention for its claim that apolipoprotein B (ApoB) does not contribute to coronary plaque progression in individuals adhering to a ketogenic diet. However, critical examination reveals major concerns about selective outcome reporting, interpretation bias, and scientific framing.
The pre-specified primary outcome, percent change in non-calcified plaque volume (NCPV), was not clearly reported in the published manuscript, despite being available and later disclosed via social media as a median increase of 18.8 mm³ (~43% from baseline). This degree of progression, seen in participants with uniformly elevated Apolipoprotein B (ApoB) and Low-Density Lipoprotein Cholesterol (LDL-C) levels, far exceeds rates observed in both low- and high-risk cohorts from prior studies. Moreover, the study’s null association between ApoB/LDL-C and plaque progression is uninterpretable without the variation in exposure of a comparator group, and the use of this exploratory analysis to inform the title and conclusions is scientifically inappropriate.
Mischaracterisation of the study as a “trial” and emphasis on biologically uninformative explanations further undermine the credibility of the findings. Given the public health implications and potential for misinterpretation, it is vital to clarify that this study in fact provides evidence of accelerated atherosclerosis in a population described as “metabolically healthy.”
Everyone needs to be aware of the fundamental flaws with this study as well as the dishonest communication of their authors. Share widely! 👏🏼
@drgarymcgowan@DrNadolsky