Endogenous GLP1 is detectable in synovial fluid, strengthening the case for a direct role in joints.
GLP1 medicines already have efficacy in osteoarthritis clinical trials – if direct, GLP1 could be suppressing inflammation, protecting cartilage or reducing pain signalling.
Six Things I See in My ‘Strongest’ 80-Year-Old Patients
I am 63 now, and after three decades as an orthopedic surgeon, I have examined thousands of people in their eighties. Some arrive frail and afraid, others walk in straighter and more confident than patients half their age.
They’re still skiing, still gardening, still picking up grandchildren without a second thought. The gap between those two groups is not luck, and it is rarely genetics alone. The same patterns keep showing up in those who are thriving.
Here is what they have in common. The most important reasons are lower down in the list…
Nope... Running Will Not Wreck Your Knees
Evolution and Data...
We did not evolve to sit in chairs. We evolved to run... for miles, in the heat, until our prey collapsed. The human body is a distance-running machine, shaped over two million years of natural selection. And most of what people believe about running and joint health is wrong. A thread.
The Frozen Shoulder... a thread.
A frozen shoulder is one of the most misunderstood conditions in orthopedics. It is not purely a mechanical problem. It is a metabolic one. The shoulder capsule becomes a target of systemic inflammation, hormonal disruption, and glycemic dysfunction. Most people, and some surgeons, still treat it as if something is stuck and just needs to be loosened... Properly managing this and the contributors is essential to resolving it.
Don’t believe the influencers telling you endurance sports will destroy your joints and damage your health.
The literature says the opposite.
Joints. The 2023 Dhillon systematic review and the Timmins 2017 meta-analysis both found running is not associated with worsening knee OA and may be protective against knee pain.
The Chakravarty Stanford cohort followed runners for 20 years and found less radiographic OA progression than non-runners.
Recreational runners in the Alentorn-Geli meta-analysis had a 3.5% pooled prevalence of hip/knee OA versus 10.2% in sedentary controls.
A serious caveat about that data. These studies have real bias problems. The Alentorn-Geli authors flagged high risk of selection, performance, detection, attrition, and reporting bias across included studies.
The authors acknowledged survivorship bias too — their runners were people who stayed runners into their 50s and 60s, which selects for individuals whose joints tolerated the activity in the first place.
So… The best take possible: the available evidence does not show running causes OA, and probably shows the opposite — but it does not prove protection.
What the data does rule out is the screaming influencer claims that running predictably destroys joints. Rubbish.
A-fib. The signal is real. Lifetime endurance loads above ~1,500–2,000 hours raise lone afib risk roughly 2–5x. But the Birkebeiner/Tromsø 10-year prospective study of older male endurance athletes — the only long prospective dataset in this population — found that despite higher afib incidence, stroke risk was substantially lower than in non-athletes.
Athletic afib is mostly vagal, lone, and occurs in people without the metabolic comorbidities that drive most embolic stroke.
Metabolism. Muscle that can actually prioritize fat oxidation is the single biggest determinant of metabolic health you can build…. and sustained submaximal endurance work is the most reliable, dose-dependent way of getting there.
Strength training won’t get you there.
The right answer is simple. Lift and run. They do different things.
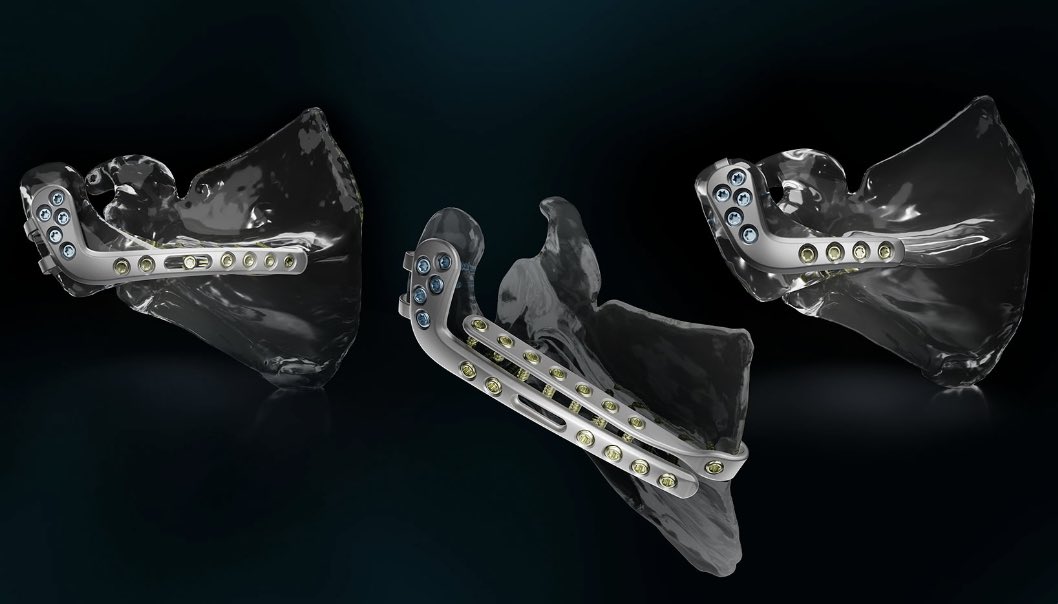
Cleveland Clinic's Great Shoulder Team
.....joined up for my last lab before launching Advita Equinoxe, the only acromial fracture solution for reverse Total Shoulder Arthroplasty. 1rst Case maiden voyage in Saint Paul tomorrow God willing!
https://t.co/uAPP0RYoMr
We had a blast discovering, sharing, learning.....
The morning lineup of cars descending at the main pavilion for patients entering for the 130 operating rooms is just like airport pickup at Christmas Time--what a Buzz!
#ClevelandClinic #ShoulderSurgery #OrthopaedicInnovation #ReverseShoulderArthroplasty #AdvitaOrthoEquinox
Viruses and Joint and Tendon Pain
You had a cold two weeks ago. Nothing serious. But now your knee hurts more than it has in months. Your achilles is flaring. Your easy run felt like a half-marathon. You didn't do anything wrong. Here's what's actually happening...
65-year-old man with acute ulnar-sided wrist pain. Referred from the ER to rule out fracture.
X-ray shows an amorphous (cloud-like) calcification just proximal to the pisiform, with adjacent soft tissue swelling.
This is typical of calcific tendinosis of the flexor carpi ulnaris tendon insertion, due to Hydroxyapatite Deposition Disease (HADD).
Often presents with acute, severe pain when the deposits becomes inflamed (resorptive phase).
No cortical break, no true fracture fragment
In the same patient, there is a separate, sharp linear subtle calcification in the triangular fibrocartilage complex (chondrocalcinosis) , consistent with Calcium Pyrophosphate Deposition Disease-(CPPD).
Do not mix the two:
•HADD (FCU) → amorphous, cloud-like, peri-tendinous.
•CPPD (TFCC) → thin, linear, cartilage-based.
Both can coexist. The painful one is usually HADD. CPPD is often incidental.
— Pearls, pitfalls and wisdom from today’s reporting list
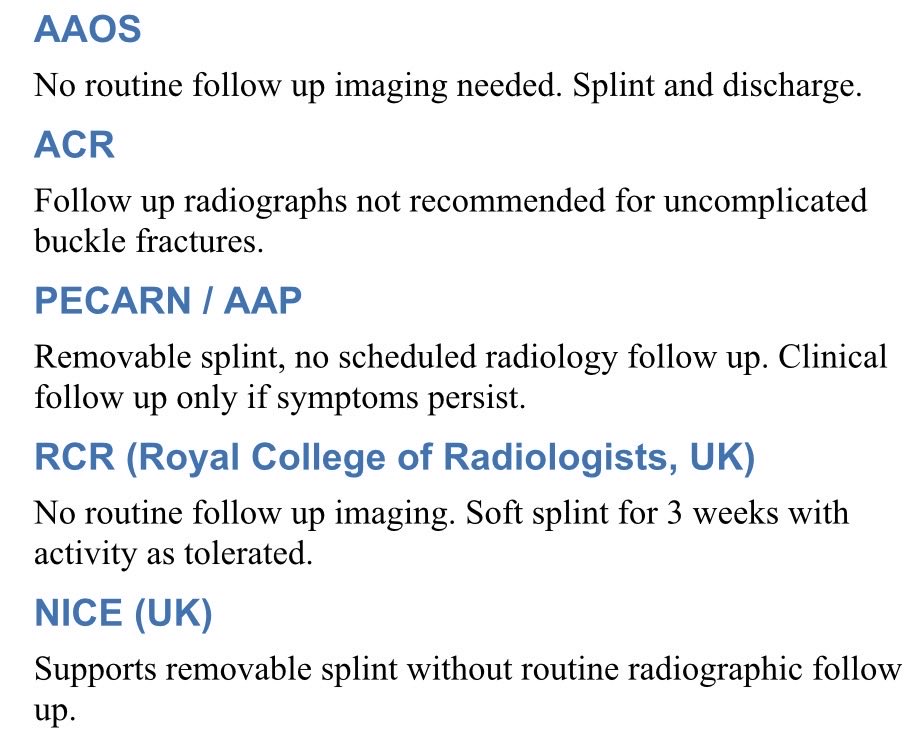
Third follow up. No new injury. Py progressing well, improving as expected and now essentially asymptomatic. Yet received 4 fu clinic x rays for buckle. At minimum sharing guidelines w parents (or PA?)could save $/time/radiation?
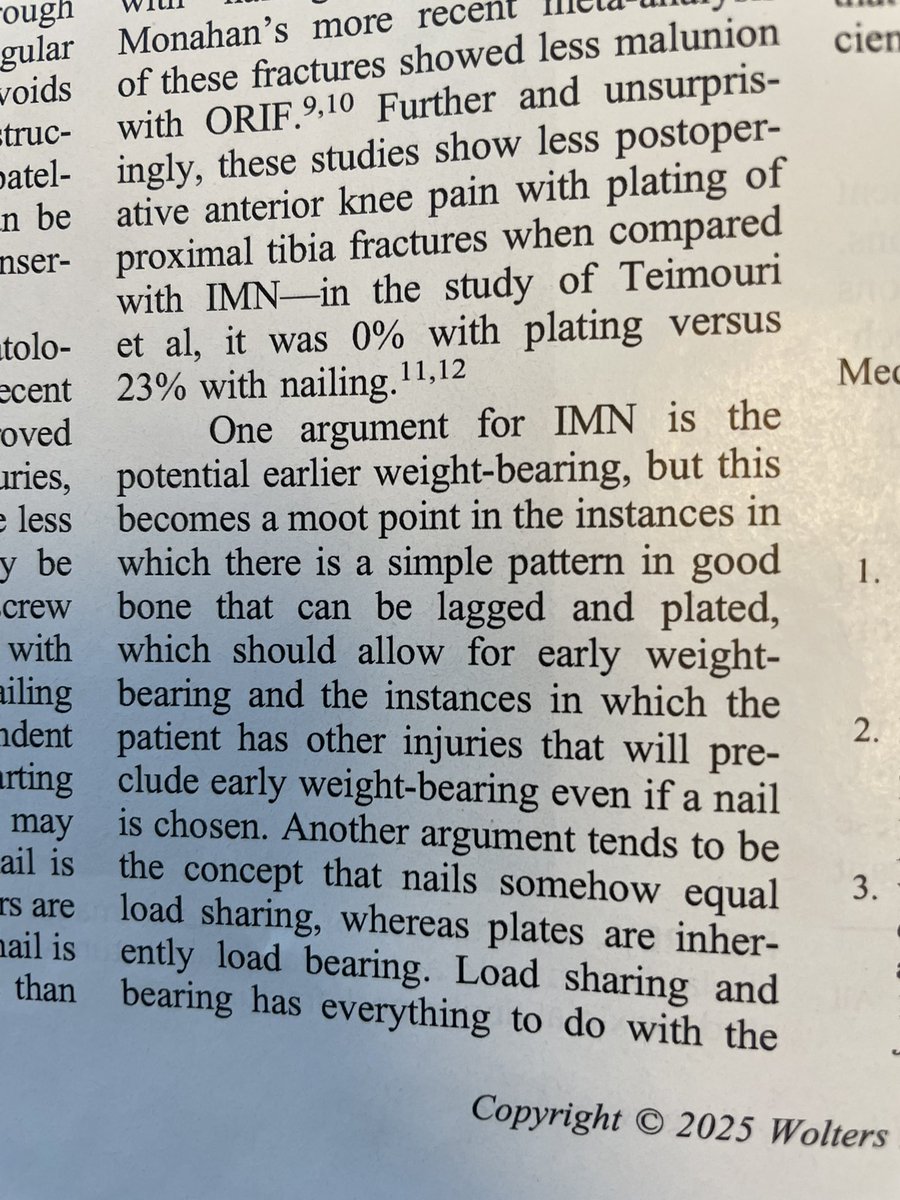
So, the whole Nail = load sharing & plate = has always seemed like b.s. to me but I never saw it written anywhere (maybe I just couldn’t find). So I wrote it (w/LS). Generations of residents (& attendings) have parroted this. No more.
The irony I find myself returning to is that MRI technology has not made us better diagnosticians. It has, in many cases, made us worse ones, because the image is so concrete and the language of the report so authoritative that it takes deliberate effort to resist anchoring to it.
When the MRI arrives before the history is fully taken, the finding shapes what questions get asked and which ones don't. Bias abounds throughout the encounter.
The encounter organizes itself around what the scanner found rather than what the patient experienced, and that is very difficult to undo once it has happened.
Don't look at the scans first... the basics matter. Take a history... confirm it with an exam, then see if the MRI findings make sense in the same context.
Another study from @ficebo presented today at #AAOS2026 in New Orleans.
Cost‑effectiveness of surgery vs functional bracing for humeral shaft fractures.
Presented by Cyrill Suter — Switzerland’s gift to FICEBO.
Based on the landmark FISH randomized clinical trial.
If you missed this study, it's well worth a look
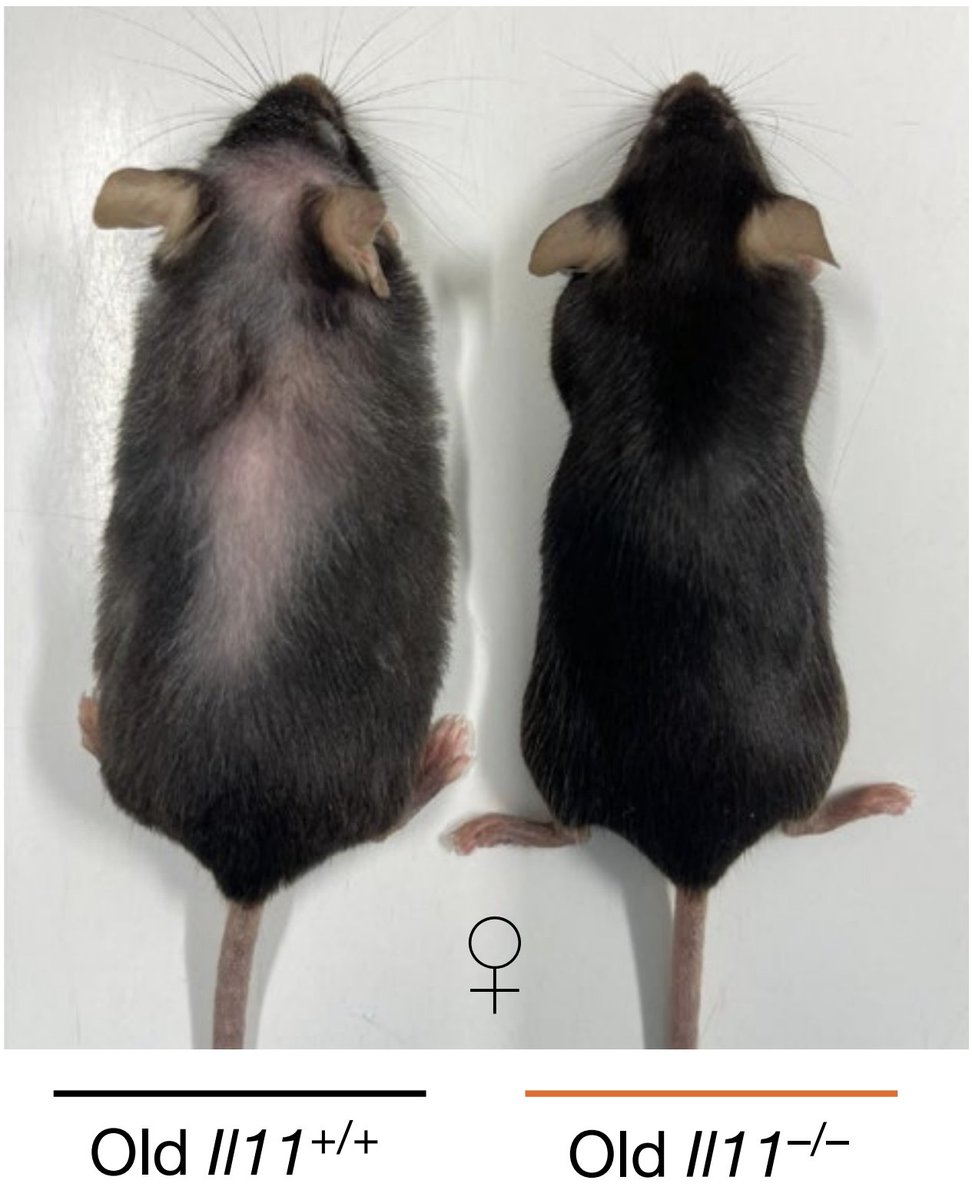
Blocking the pro-inflammatory cytokine, IL11 (by deleting it, or with a therapeutic antibody) makes mice live healthier, for longer — and they look younger too
In science, p < 0.05 has become a religion
It is simply a probability statement about data under assumptions, yet scientists and society treat it as the essential stamp of truth