Neurologist at Sarah Network of Rehabilitation Hospitals, Movement disorder specialist, Botox administration since 2005, Neuromodulation enthusiast since 2014.
I needed to create this new account because the last one @DrGuerraA isn’t loading messages. I don’t know why. I thought it would be some temporary problem, but it persisted until now. I hope now I can read the tweets and interact again with so many great people and organizations.
Key Point 4 from the article Sex Differences in Stroke Diagnosis, Treatment, and Outcome by Dr. Cheryl E. Carcel from the June #CerebrovascularDisease issue, which is available to subscribers at https://t.co/iIfDdVpIkR. #NeuroTwitter#MedEd
@IMGLOBAL Patriot Platinum vs Patriot Lite (Europe/Andorra) — practical, real-world questions before buying
I’m comparing Patriot Platinum vs Patriot Lite for a trip across Spain/Portugal/Andorra (including recreational on-piste skiing, with ski school). Before purchasing.
@IMGLOBAL Hi IMG,
Planning Spain/Portugal/Andorra trip (Feb 2026). Patriot Platinum vs Lite:
• Europe: WhatsApp? Portuguese support? Direct billing or reimbursement only?
• How does assistance actually work in Europe?
• What guarantees do non-US buyers have?
How can I get reliable info?
@IMGLOBAL Hi IMG,
Planning Spain/Portugal/Andorra trip (Feb 2026). Patriot Platinum vs Lite:
• Europe: WhatsApp? Portuguese support? Direct billing or reimbursement only?
• How does assistance actually work in Europe?
• What guarantees do non-US buyers have?
How can I get reliable info?
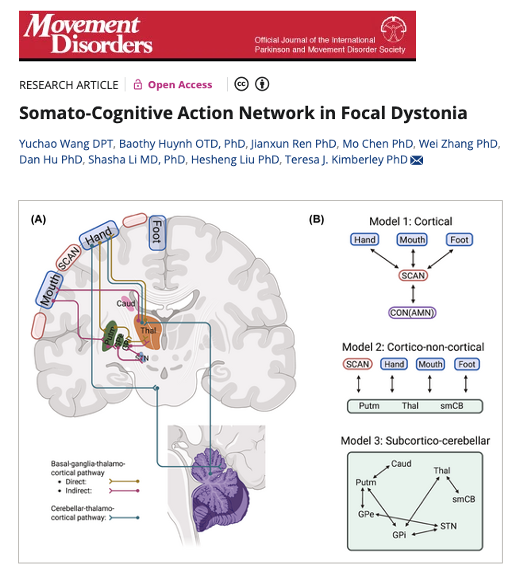
A new study in Movement Disorders highlights the role of the somato-cognitive action network or SCAN in focal dystonia. Today marks the start of the DBS Think Tank and I will be asking Nico Dosenbach: When you keynoted the DBS Think Tank a few short years ago, did you imagine the impact of SCAN imaging on decoding so many diseases? Could this most recent dystonia study help us to reshape how we think about task-specific voice and hand disorders?
Key Points:
- SCAN connectivity was abnormal in both laryngeal and hand dystonia, regardless of which body part was affected.
- Persons w/ dystonia showed higher SCAN connectivity w/ vocal regions and lower connectivity w/ the cingulo-opercular network suggesting impaired communication between intention and action.
- An exploratory analysis revealed an asynchronization between SCAN and the cerebellum pointing toward a potential shared pathological mechanism in dystonia.
My take: The somato-cognitive action network introduced by Gordon and Dosenbach has been helping us put together a lot of missing puzzle pieces for many diseases. Though this study was small, there were 5 points that resonated w/ me about dystonia and SCAN: 1- Dystonia is not just a muscle problem, it involves brain networks that link thinking to movement. 2- The SCAN is a brain hub that helps translate intention into action and it appears disrupted in dystonia. 3- Abnormal SCAN activity was found in both voice and hand dystonia suggesting a potential common cause. 4- The brain’s normal balance between SCAN and the cerebellum was altered, which may explain some dystonia symptoms. 5- Understanding these network changes may open doors to new treatments and possibly brain stimulation targets.
https://t.co/mTuhegf3Yv @ndosenbach@DBSThinkTank@ParkinsonDotOrg@dmrf #dystonia @TylersHope@SfNtweets@FixelInstitute
Kapil Sethi M.D. (1953-2024) a legend has passed and Professor @JankovicJoseph just honored at the @movedisorder Aspen Movement Disorders Course where he was a past distinguished faculty. His legacy will be with us forever, as he was such a kind and wonderfully inspiring leader who always made the young people around him 'feel like they were the most important people in the room.' It was his 'superpower.' From 'Aspen in Aspen' to 'Aspen in India' to 'MDS video challenge' to 'Neurobowl' and he impacted so many lives of persons with disease, and he inspired the future generation of trainees. Rest in peace my friend, and 'our friend.' We will all miss you so much. Every time you walked into a room you made it better. Every young person you interacted with came away inspired to impact the world. Every person with disease you touched lived better because of you.
This @TheLancetNeuro interview in 2017 captured him and his legacy so well.
"You may know him as Professor Emeritus of Neurology at the Medical College of Georgia, Augusta University (Augusta, GA, USA), as director of the College's Movement Disorders Program (1985–2016), or perhaps as director of its National Parkinson's Foundation Center of Excellence (2000–2009). You may know him from the many (many) clinical trials on Parkinson's disease, restless legs syndrome, and other movement disorders with which he has been involved. Many of you will know him best as your teacher—the expert in movement disorders who tried to make your medical training more meaningful, more relevant, and whenever possible, more fun. His own primary school teachers back in the Punjabi town of Sultanpur, however, knew him as the little rascal who used to run away from school and who had to be dragged back to class (yes, truly held on jute mats under a shade tree). While he tells me his story, I wonder if what I write should be a tribute to him or to those teachers, whose brilliant educational diagnosis and application of the right treatment planted the seed that grew into those different Kapils we know today.
“I hated didactic teaching and was bored stiff”, he remembers. “After leading school prayer at 9 am I used to quickly run away to play with boys who never did any schooling. We would jump on the backs of water buffaloes and bathe in the stream nearby to cool off. I have vivid memories of the schoolteacher sending half the class to find me, and of the bigger boys who brought me back, kicking and screaming. The teachers soon discovered that the only way to keep me in school was for me to teach a junior class and sometimes even my own. I guess that set the stage for the rest of my life.”
To stop his own medical students from running away, Kapil has championed the idea of patient-centred, problem-based learning. “It's about starting with a patient's problem and learning backwards”, he explains. “In traditional medical teaching, students don't see a patient for at least two years, but as soon as they get into a clinical rotation their eyes light up! They realise that everything they learnt for those two years was for a reason, but they also know that that time was SO boring! But does it have to be so? In our movement disorder program we have students from the first year seeing patients, at least on videos. They want to be doctors, and this way they see the problems that people have. We then help them try to come to a diagnosis and choose treatment options. The book learning on disease mechanisms, patient management, the equations, etc. comes later and is integrated into this clinical experience, making that learning more meaningful.” His own teachers at the DAV College, Jalandhar (Punjab, India), where Kapil did his undergraduate studies, didn't use those techniques, “…and during my fist year I missed half the didactic classes and watched about 200 Bollywood movies instead”, he recalls (perhaps not without a little shame).
But while Kapil is best known in different ways to different people, everybody knows him as the judge at Neurobowl, one of the most popular opening events at the annual American Academy of Neurology meetings. “Neurobowl was the brainchild, over 20 years ago, of Tom Swift, my Augusta colleague and mentor. We collect case examples of difficult and rare cases, and everyone tries to figure out what the patient may have and how to help. It's educational, it's training, and it's fun. Basically, it's how we teach in our movement disorder program.” The International Parkinson and Movement Disorder Society now runs something similar at its meetings called the Video Challenge—and guess who is Co-Master of Ceremonies? Were it not for his father's insistance, however, he might never have sat in the judge's seat. “I wanted to be a singer when I was young, but my Dad thought I wouldn't make a very good living at it, and he had other ideas”, he recalls. “Basically, he told me that I was going to be a doctor! I have, however, kept my interest in music and learned to play amateurish tabla and I still sing Hindi and Panjabi songs”. In fact, he is a member of a band along with his daughter and son-in-law.
After Kapil's arrival in Georgia in 1983 following a two-year stint in the UK and seven years training in India (having graduated in medicine from the Christian Medical College in Ludhiana, Punjab), it was the same Tom Swift who suggested he develop an interest in movement disorders. “And after nine and a half years of residency, I was sick of being trained and re-trained”, says Kapil, “so one fine morning I declared myself to be a movement disorders specialist. Now all I had to do was prove that I was not a fake!”
Just before our time winds up, Kapil mentions something that makes movement disorders seem the perfect career choice for someone who in his own words “hated didactic teaching”. “With these disorders you always have to start with the patient,” he insists. “It's about keen observation and coming to a diagnosis through that. You can't learn that from a book.” It kind of sums him up. As I pack my recording equipment, my thoughts drift back to that empty jute mat under the shade tree, and I wonder what Kapil's primary school teachers would think of him now, and of their achievement: a professor of movement disorders made out of a little boy who, long ago, they understood how to make sit still." https://t.co/kz12pEncFC
Modulating networks using DBS is an effective treatment for PD – but which circuits map to improvements in individual symptoms such as tremor, bradykinesia, rigidity, and axial? A 🧵 about our new paper out now in @NatureComms https://t.co/4KPUBGgsRd @netstim_org
Master's Thesis Defense successfully completed.
Levodopa-Responsive Dystonia due to Mutations in GCH1/TH Genes in a Patient Cohort Treated at the SARAH Network of Rehabilitation Hospitals.
Thank you to everyone who contributed to making this possible, especially to God.
Do you know the 7 new 'best practices' for relaying a diagnosis of dementia? Did you know previous standards did not take input from the person with disease or from the caregiver/care-partner? This is a super important issue and Melissa Armstrong @FixelInstitute and colleagues performed an important 'freshly' published study.
Key points:
- It is common for folks to report not receiving a dementia diagnosis.
- There are standards and as the authors point out they are more than 10 years old.
- Guess what, the standards were developed without asking the person with disease or caregiver/care-partner.
- The authors used a multi-stakeholder working group: a person w/ disease, caregivers, Alzheimer's Association staff and clinicians from diverse backgrounds.
- Employed American Academy of Neurology process for recommendation development w/Delphi voting for consensus.
- 7 best practice statements achieved consensus.
- 1 Clinicians must show compassion and empathy when delivering a diagnosis of dementia (level A). - During dementia diagnosis disclosure, clinicians should - 2 ask regarding diagnosis preferences.
- 3 instill realistic hope.
- 4 provide practical strategies.
- 5 provide education and connections to high-quality resources.
- 6 connect caregivers to support resources.
- 7 provide written summaries of the diagnoses, plan, and relevant resources (each level B).
My take: It is about time someone addressed this topic and included both persons with disease and relevant stakeholders. The 7 best practices are simple and practical. In my experience many clinicians avoid this discussion rather than 'leaning into it.' If clinicians are concerned that cognition is slipping, measuring function over time and employing the use of neuropsychology can be very helpful. These discussions are as important to caregivers and care-partners as they are to family members. I love the author's suggestion that 'health system changes (e.g., for sufficient time), improved access to specialty dementia care, and clinician training for delivering difficult diagnoses' are all needed.
https://t.co/2PaJqUfk7h
Going for a 20 minute walk in nature is an underrated form of therapy.
Walking improves recovery by stimulating blood flow throughout your entire body.
Walking as little as 6000 steps a day has been correlated with decreasing all-cause mortality by 45%.
Walking enhances your cognitive function by boosting BDNF and promoting neuroplasticity.
Harvard psychiatrist John Ratey, MD, author of Spark: The Revolutionary New Science of Exercise and the Brain, has called physical activity
“A little bit of Prozac and a little bit of Ritalin” and “Miracle-Gro” for the brain.
You only get old when you stop walking. You don't stop walking because you get old.
Do you want an easy way to improve your health? Go for a walk.
This study's findings suggest that the cerebellum is the central hub of a network commonly connected to structural and metabolic abnormalities in essential tremor: https://t.co/XJjuqmMP0X
#NeuroTwitter
Reunião científica do capítulo ABN-DF - Distúrbios do Movimento.
A reunião ocorrerá dia 06/07/2023, quinta-feira às 19h, no auditório I do HUB.
É necessário se inscrever no link:
https://t.co/7CxQ46kI2N
Why everyone with Parkinson's disease should take 'just one' multivitamin a day, especially if on levodopa therapy. Read this month's blog which also has some tips on vitamin toxicity. Let's celebrate Parkinson's Awareness month by learning together. https://t.co/GngtmaolXj
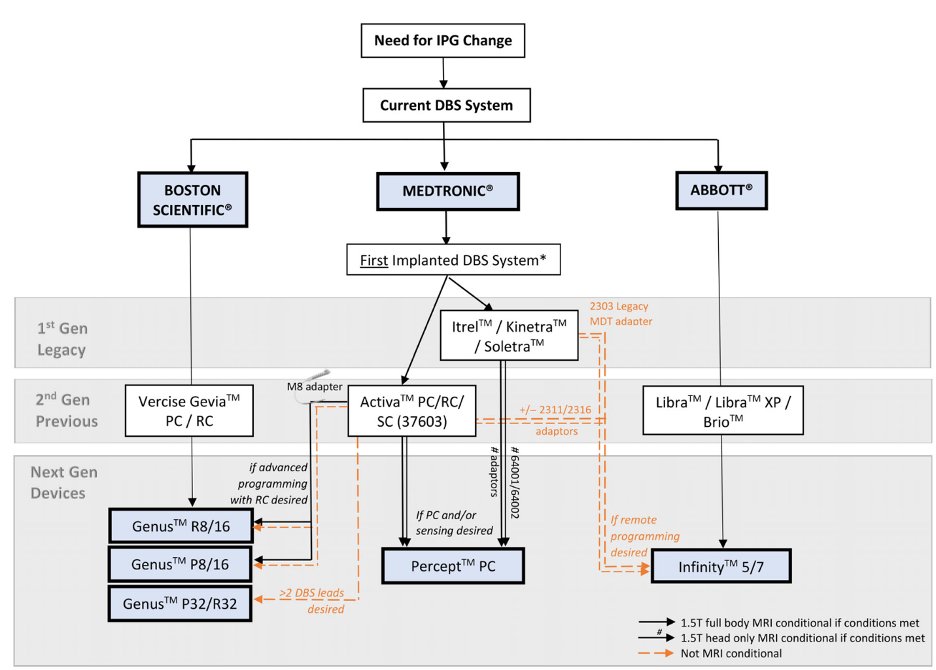
Deep Brain Stimulation, or DBS, is an excellent treatment for a variety of movement disorders. Next-generation implantable pulse generators (AKA, DBS batteries) have revolutionized the field, leading many patients to consider upgrading their existing DBS systems.
@PennNSG
When you have mild cognitive impairment and are trying to determine if #Lewybody or #Alzheimers guess what? It is tricky clinically. This paper is a START to looking at features which may or may not be helpful. Time is usually the ultimate jusge. Thoughts?
https://t.co/3Y1CxCCOF8
In a prospective longitudinal study, Wilson et al. provide a detailed description of recovery from aphasia in the first year after stroke, documenting distinct trajectories of recovery for different speech and language domains. https://t.co/wr8187ZHZK
Excellent talks on prodromal & motor symptoms of #parkinsons, #neuropsychiatric issues, & treatments at #admufmg30 in Ouro Preto 🇧🇷. Werner Poewe, Eduard Tolosa, Henrique Ferraz, @stcamargos & more, honoring Francisco Cardoso’s unit. Obrigada! @movedisorder
Could a history of childhood abuse change your neural network? Check out data from this new @JAMANetworkOpen which suggests it may be possible!
Neural Connectome and Early Abuse in Adults https://t.co/F32AJ3mHBJ