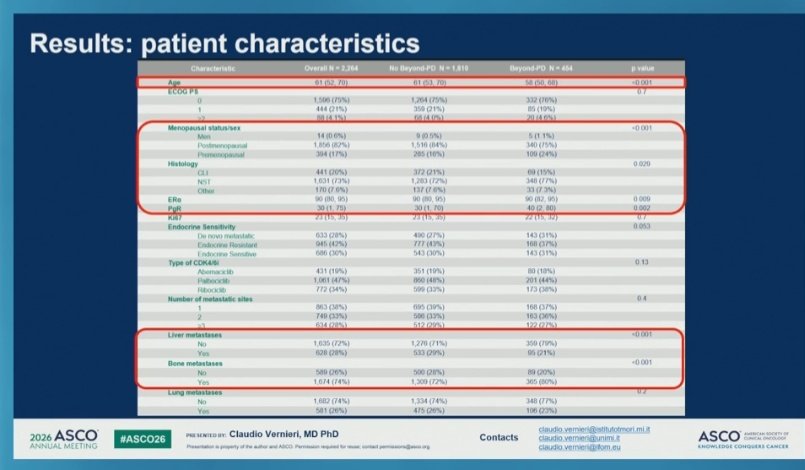
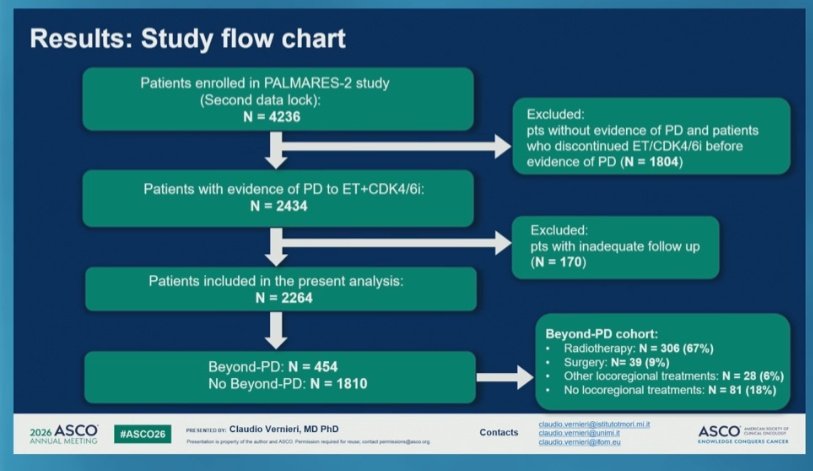
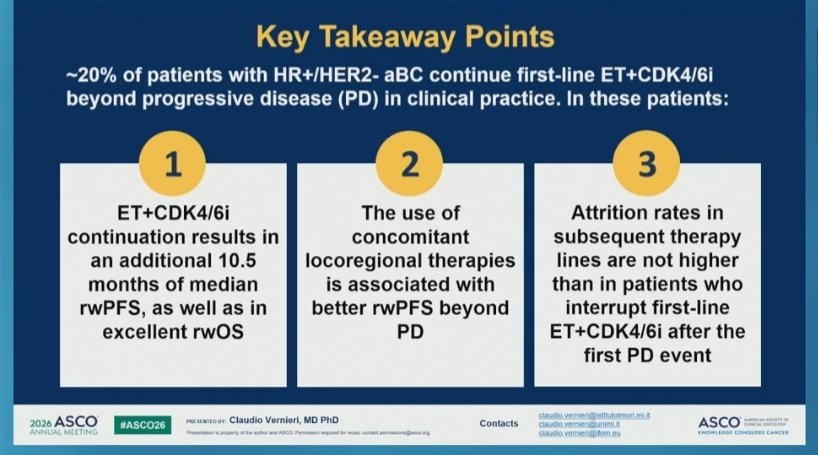
In the real world 🇮🇹 PALMARES2 trial, continuation of CDK4/6i+ET beyond progressive disease resulted in additional 10.5 mos in median rwPFS
Loco regional tx was associated with better rwPFS
@OncoAlert#asco26
Just published in JACC @JACCJournals!🫀
Acute HF care is evolving:
📍Rapid diagnosis
📍Early decongestion
📍Timely GDMT initiation
📍Structured follow-up
📍Focus on long-term outcomes, not just symptom relief
Grateful to have contributed to this international collaboration & learned so much from the exceptional experts involved in this work. Congratulations to @Jolie_Bruno_ and @AlexMebazaa for the leadership & to all co-authors on this important publication🫀
Read the full paper🔗: https://t.co/408QmNOznr
#HeartFailure #AcuteHeartFailure #JACC @jozinetm@BiykemB@GianluSava@pmyhre
Prevalence of symptomatic skeletal events (SSE) with reduced denosumab (Dmab) dose density (every 12 weeks versus every 4 weeks): A randomized phase III non-inferiority trial SAKK 96/12 REDUSE. Abstract 1004 to be presented at #ASCO26
https://t.co/ioQu0sQMYP
The SAKK 96/12 REDUSE trial demonstrated that denosumab administered every 12 weeks after an initial loading phase was non-inferior to standard every-4-week dosing in patients with 🦴bone-metastatic #BreastCancer or castration-resistant #ProstateCancer . Time to symptomatic skeletal events was comparable between schedules, while📉 reduced-frequency dosing resulted in lower rates of hypocalcemia and osteonecrosis of the jaw.
These findings support Q12W denosumab as a new standard of care, reducing toxicity, treatment burden, and healthcare costs without compromising efficacy.
@Silke_Gillessen@RothschildSacha@OncoAlert@AOmlin@weoncologists
🌟 Honored to speak at #ESMOBreast26 today on "Adjuvant CDK4/6 inhibitors: Could they replace chemo for intermediate-risk ER+ eBC?"
Outstanding educational session chaired by @SibylleLoibl, with C. Denkert, FC. Bidard & H. Parsons. 🎓
1/ Very pleased to share our new State-of-the-Art Review in JACC: CardioOncology
In this review, we outline a practical framework for developing and evaluating risk prediction tools that are actually fit for cardio-oncology.
https://t.co/GpO8MPrEez
One of the most notable studies from #AACR26:
Daraxonrasib + gem/nab-paclitaxel shows a strong early signal in 1L mPDAC.
ORR 58%
DCR 90%
6-month PFS 84%!!
Things are finally moving in pancreatic cancer👇
https://t.co/ijyGOW6hmE
للمهتمين بالبحث العلمي 📚
ملف جدا جميل يشرح لك خطوة بخطوة طريقة نشر بحثك في مجلة ذات تصنيف عالي Q1 وطريقة العثور على المجلات المناسبة لبحثك
رابط الملف:
https://t.co/MnqIXZIpt5
In mBC, not all imaging changes mean your therapy has stopped working and switching too early is a real risk.
1/ RECIST 1.1 sets a clear bar for progression: ≥20% increase in the sum of target lesion diameters (with ≥5mm absolute increase), unequivocal progression of non-target lesions, or new lesions. Not every change on imaging meets this threshold.
2/ Three scenarios commonly and incorrectly flagged as progression: new asymptomatic sclerotic bone lesions, small mm asymptomatic changes in known lesions, and increased SUV on PET without corresponding size change. None of these, in isolation, trigger a therapy switch for me.
3/ Sclerotic bone lesions deserve particular attention. When effective therapy kills tumor cells in bone, the body lays down new bone matrix appearing dense and white on CT. This is a healing response, not new disease.
4/ The consequences of switching too early are real: loss of disease control from a working regimen, premature exhaustion of sequencing options.
5/ My approach: I integrate clinical symptoms, tumor markers, and serial scans together before making any decision to change therapy.
6/ Bottom line: confirm true progression before changing course. When in doubt, a short interval rescan is almost always preferable to an unnecessary switch.
#BreastCancer #MedOnc
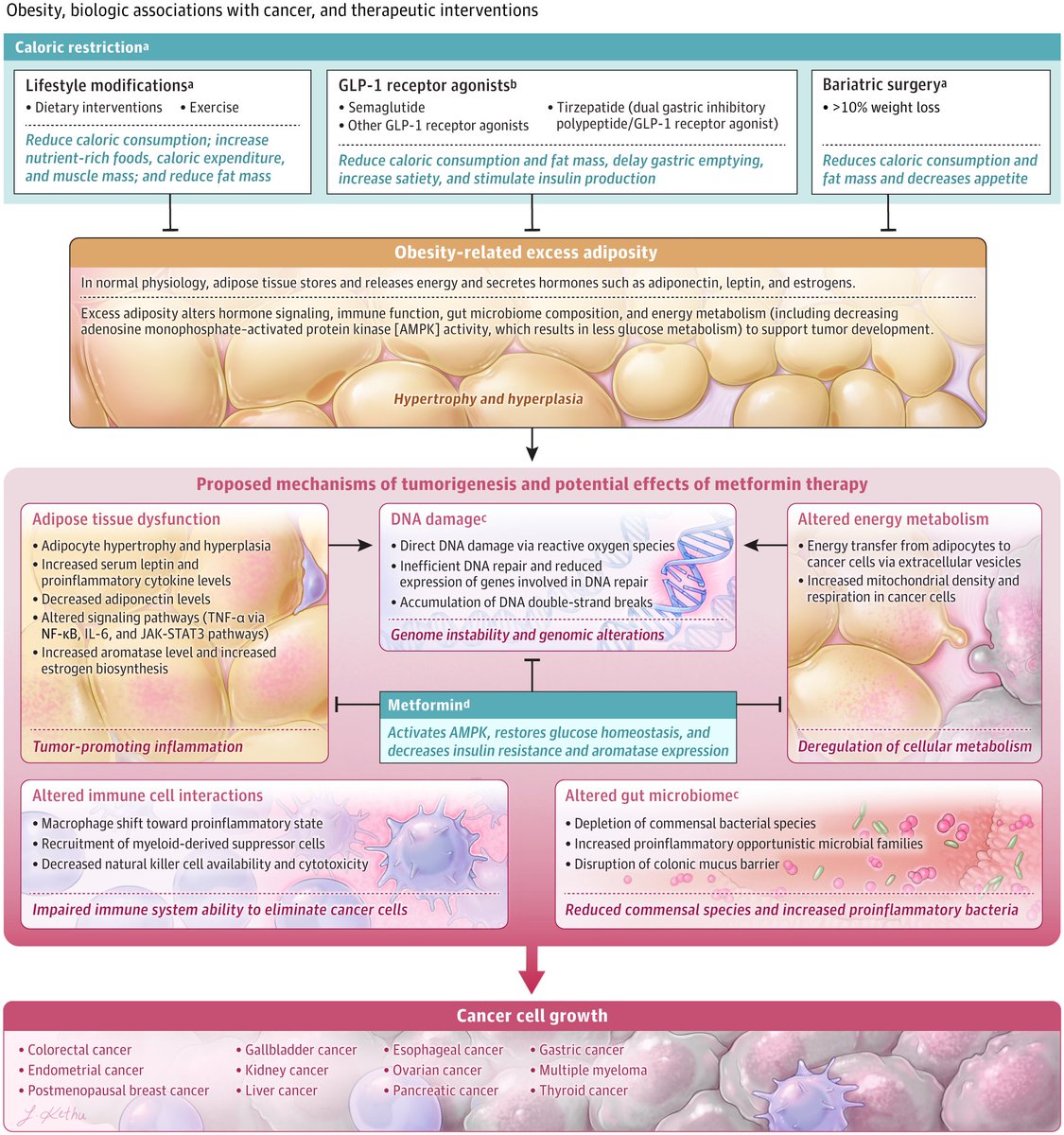
Obesity is linked to at least 12 cancers.
Here’s part of the biology in @JAMA_current
Dysfunctional adipose tissue becomes a pro-tumor endocrine organ, driving insulin signaling, estrogen excess, chronic inflammation, and immune suppression.
In other words: obesity can help create the ecosystem cancer needs to grow.
https://t.co/o9OHokqMuJ @OncoAlert
Risks of thrombosis and hemorrhage in concurrent use of anticoagulants and potential interacting prostate cancer agents
https://t.co/Inu5taP3Zl
In a population-based retrospective study from Ontario and Alberta, Canada🇨🇦 (2012–2023), investigators evaluated whether androgen receptor pathway inhibitors interact with direct oral anticoagulants (DOACs) in patients with #ProstateCancer . Among 2,997 patients, concurrent use of enzalutamide or apalutamide with DOACs did not increase thrombosis risk, and abiraterone with DOACs did not increase bleeding risk🩸
Overall, combining these therapies showed no clinically meaningful impact on thrombotic or bleeding outcomes.
@TzufeiWang@Dominick_Bosse@pietro_ravani@Msood99M@MarcCarrier1@OncoAlert@silkegillessen@AOmlin@weoncologists@JournalCancer
Alcohol increases breast cancer risk — and it’s dose-dependent 🍷
+13% (light) → +52% (heavy)
Stronger in HR+ disease.
After diagnosis? No clear rise in recurrence.
Less alcohol = lower risk.
#MVOnco#BreastCancer#Oncology#CancerPrevention