⚠️ Low BP in HFrEF — should it stop us from using GDMT? Data says: probably not.
From COPERNICUS, PARADIGM-HF, RALES/EMPHASIS-HF & DAPA-HF:
✅ Carvedilol beneficial even at SBP 85–95 mmHg
✅ Sacubitril/Valsartan consistent across all BP strata
✅ MRA & SGLT2i similarly effective in low BP groups
Low SBP is a reason to be careful — not a reason to stop. 💡
#HeartFailure26 #HF2026 #HFrEF #GDMT #Cardiology
💧 REDOX-AHF — Should we rethink oxygen in acute heart failure? #HF2026
The question nobody has properly answered yet:
Oxygen is given to virtually every AHF patient on arrival — but is more O₂ actually better? Or could it be harmful?
The problem with current practice:
Despite oxygen being one of the first interventions in the emergency setting, optimal oxygen saturation targets in AHF remain unclear. Many patients receive O₂ to maintain SpO₂ >95%, while guidelines only recommend initiating therapy if SpO₂ <90% — a major discrepancy between practice and evidence.
The design:
Investigator-initiated, prospective, randomized, blinded, multicenter RCT — 122 patients with acute HF and pulmonary congestion, enrolled in the emergency department.
Randomized 1:1:
➡️ Liberal oxygenation → SpO₂ target 96%
➡️ Restrictive oxygenation → SpO₂ target 90%
Oxygen delivery automated via the O2MATIC robot to ensure blinded, precise titration.
Why restrictive O₂ might actually be better:
Hyperoxygenation may mask changes in SpO₂ that signal clinical deterioration — potentially delaying timely detection and intervention in AHF patients.
A systematic review in progress hypothesizes that restrictive oxygen strategies may be associated with reduced mortality and fewer serious adverse events.
Why it matters:
Oxygen is the most universally administered treatment in acute HF — and it has never been properly trialed. REDOX-AHF could rewrite the first line of our management algorithm.
Results today at 13:15 CET 👀
#REDOXAHF #HF2026 #HFA #ESC #HeartFailure #AcuteHeartFailure #Oxygen #Cardiology #MedTwitter
https://t.co/6WeImiXFRi
@cardiojaydoc02@wittykidney@BooyahBossman In fact..there is even data that suggest that restriction might be harmful since it upregulates ADH (=vasopressin)…
@cardiojaydoc02 : really admire how you keep asking attention to this important subject!! 🫡💪🏻
“Far too often, companies are suppressing unfavorable clinical trial results and keeping them secret from patients and the scientific community."
- Marty Makary
This reminds me of the “Dead Letter Office” that @coconnormd started several years ago in @JACCJournals Heart Failure.
But where will these negative studies be published? We know that citations are lower for negative studies and journals and researchers are focused on the impact factor and H index.
https://t.co/RpwspApo1W
https://t.co/3kL9FK03Pz
Rare clinical presentations remind us how important careful diagnostic evaluation and multimodality imaging are in cardiology.
This case report highlights the complexity of recognizing uncommon cardiac conditions and the value of a multidisciplinary approach.
Published in European Heart Journal – Case Reports:
https://t.co/iazFLOe9MT
#CardioTwitter #Cardiology #CardiacImaging #CaseReport #EHJCR #MedTwitter
#EHJCaseReports @Phiso_de@TJ_Yeo@aayshacader@BoldiKovacsMD@SukritiBanthiya@ANazmiCalik@O_Azizy_MD@saramoscatelli7@EHJCREiC #CardioX
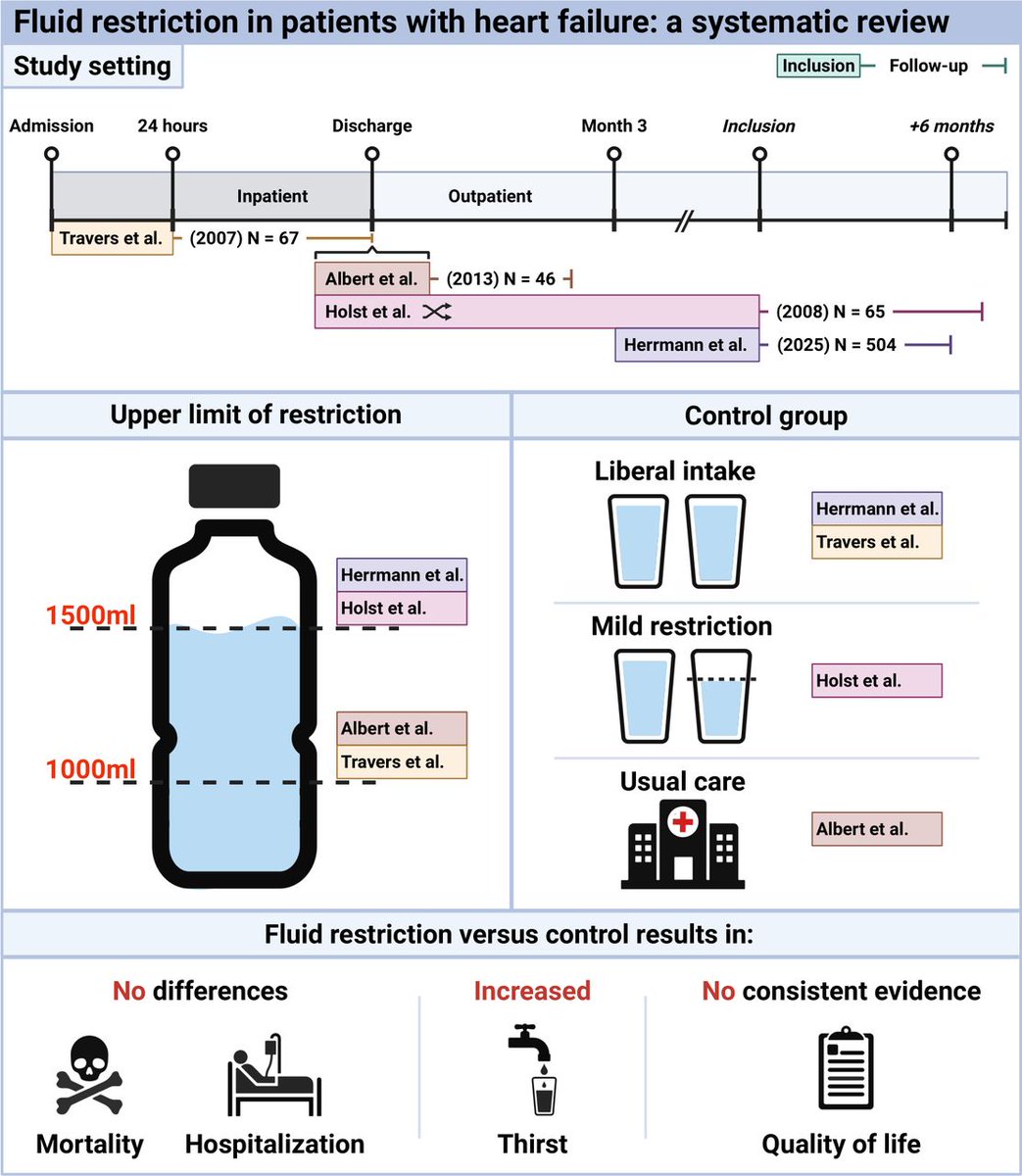
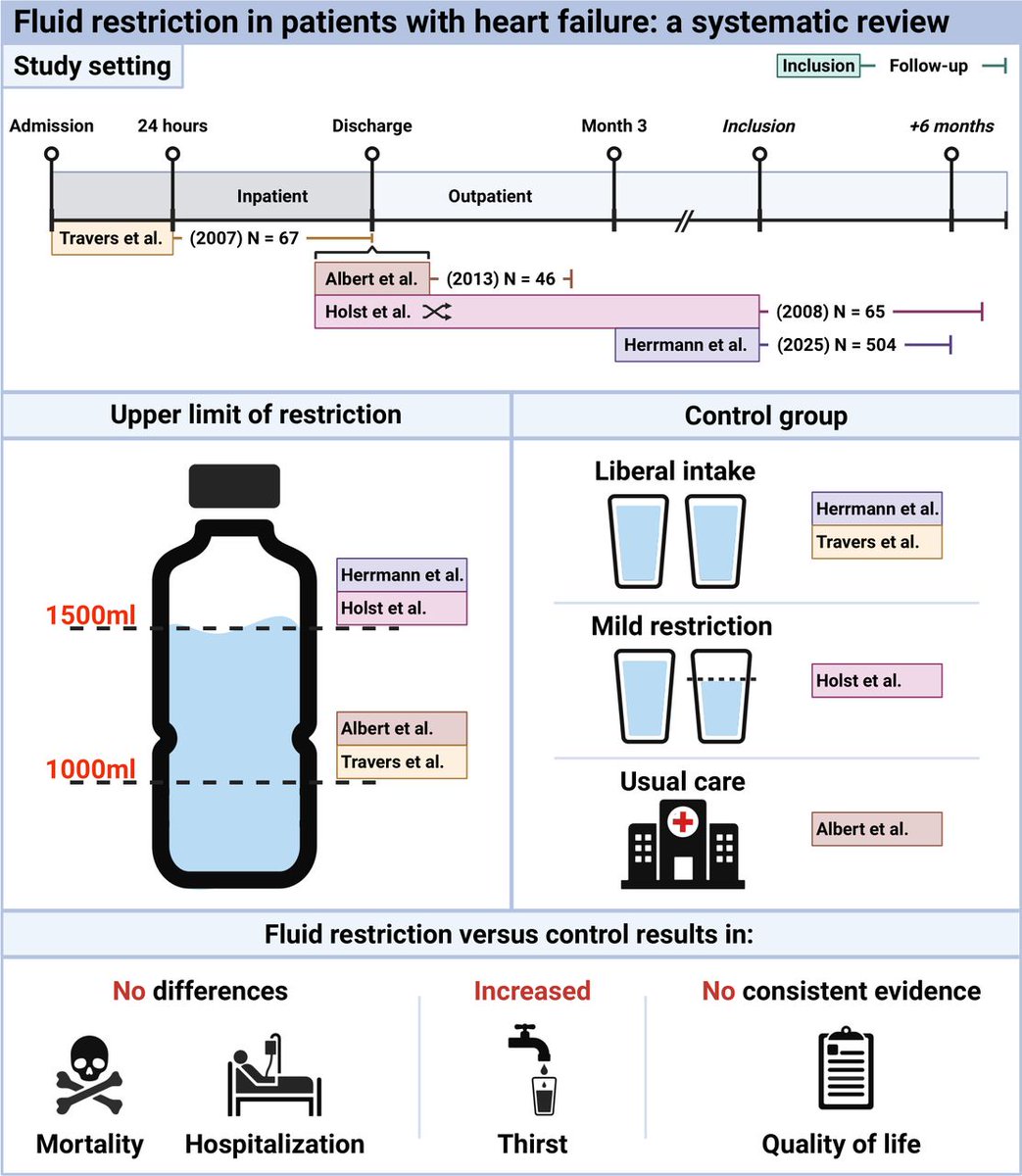
Fluid restriction in patients with heart failure: a systematic review
Studies on fluid restriction in patients with HF are scarce, and most of the available studies are at high risk of bias. Although power is lacking, there is no evidence indicating that fluid restriction affects mortality or HF hospitalisations, but there is a signal of harm in terms of thirst distress
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@mvaduganathan@HFA_President@hfcollaboratory@DrMarthaGulati@hvanspall@dranulala@dranulala@SJGreene_md@gcfmd
https://t.co/rqXQCbHe38
A Bayesian analysis of finerenone in heart failure with mildly reduced and preserved ejection fraction: a pre-specified analysis of FINEARTS-HF
The non-steroidal MRA finerenone reduced the rate of cardiovascular death and total heart failure events under both frequentist and Bayesian inference methods. The probability of benefit exceeded 80% for both cardiovascular and all-cause mortality with finerenone
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@mvaduganathan@hfcollaboratory@gcfmd@ESC_Journals@escardio@ShelleyZieroth@AndrewJSauer@safchat
https://t.co/wXb2XgPbXI
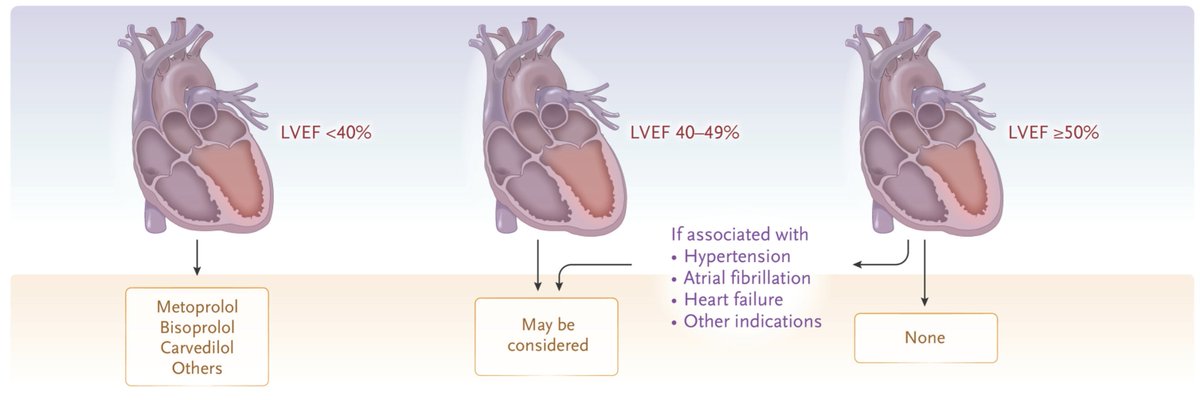
After the two recent meta-analyses published in The Lancet and NEJM, one could argue that the case is settled: following myocardial infarction, beta-blockers should be prescribed to patients with an LVEF <40%, may be considered in those with an LVEF of 40–49%, and in patients with an LVEF ≥50% only if there are other indications, such as hypertension, atrial fibrillation, or heart failure. The guidelines are partially misaligned with the emerging evidence and will most likely be updated in the near future.
ENCORE: One of JACC Heart Failure @JACCJournals most-read papers of 2025 — and the timing couldn’t be better.
If you care about heart failure outcomes and the aldosterone–mineralocorticoid receptor axis, this state-of-the-art review is worth a spot on your reading list.
Why now?
We’re at an inflection point in the MRA space. Traditional steroidal MRAs (spironolactone/eplerenone) remain foundational in HFrEF with Class I, Level A evidence, yet real-world use is still strikingly low, often driven by concerns about hyperkalemia, kidney function, and endocrine side effects.
Meanwhile, the evidence base for nonsteroidal MRAs (nsMRAs) has matured fast, especially for patients who live at the intersection of HFpEF/HFmrEF, CKD, and diabetes.
What this review does:
Clarifies the “why” behind class differences: nsMRAs lack a steroid nucleus and have different receptor selectivity, PK/PD, and heart–kidney tissue distribution, which may translate into a distinct efficacy/safety signature.
Synthesizes the clinical trial landscape: from the established HFrEF benefit of sMRAs to the more mixed HFpEF story (including the well-known TOPCAT regional issues), and then the expanding outcomes data for nsMRAs.
Frames what’s next (and what we still don’t know): head-to-head outcomes comparisons remain limited, and the pipeline (MR modulators, aldosterone synthase inhibitors) is evolving quickly.
Why it matters clinically:
For many of our patients with HF (especially those with CKD/diabetes), we’re constantly balancing:
---“Will they tolerate an MRA?”
---“Can we keep them on it safely?”
---“Which phenotype gets the most net benefit?”
This review is a pragmatic map of that terrain and a useful way to align clinicians, pharmacists, and trialists around the next set of questions that actually matter at the bedside.
If you’re following the MRA evolution across the EF spectrum, or designing trials/implementation strategies in this space, this is a worthwhile download for your files.
https://t.co/a4PoLtdYo1
🫀⚡ Extreme CAC doesn’t automatically mean severe disease: photon-counting CCTA tells a more nuanced story
REPOST b/c this is a change practice information.
This 2026 JACC: Advances brief report addresses a long-standing dilemma in preventive cardiology: what do we really find when asymptomatic patients with extreme coronary artery calcium (CAC >1,000 AU) undergo coronary imaging? With photon-counting CT (PCCT), the answer is far less alarming than many assume .
📊 Who was studied
The authors evaluated 19 asymptomatic patients (mean age 64.5 years, 32% women) with a mean CAC of 1,510 AUand no prior CAD, MI, or revascularization. All underwent ultra–high-resolution PCCT coronary CTA (0.2 mm slices), interpreted using CAD-RADS 2.0. FFR-CT and invasive angiography were used selectively.
🔍 Key findings
✅ 100% of PCCT scans were diagnostic, despite extreme calcification
74% had no severe coronary stenosis
CAD-RADS 2–3: 74%
CAD-RADS 4: 21%
CAD-RADS 5: 5% (1 patient)
FFR-CT (n=7) was negative in all tested patients (FFR 0.80–0.93)
Invasive angiography (n=4) confirmed:
1 true high-risk case → CABG
No PCI performed in any patient
🧠 Why this matters
Extreme CAC is a powerful risk marker, but it does not necessarily equate to:
flow-limiting stenosis
high-risk coronary anatomy
need for invasive testing
PCCT’s superior spatial resolution and reduced calcium blooming allow reliable lumen assessment where conventional CCTA often fails.
⚠️ Important caveats
Small, retrospective series; no outcome data; highly selected population. This is not an endorsement of routine CCTA in asymptomatic patients—but it challenges the assumption that CAC >1,000 makes anatomic imaging futile.
🔮 Bottom line
📌 CAC defines risk. PCCT clarifies reality.
In selected asymptomatic patients with extreme CAC, PCCT CCTA can safely exclude high-risk anatomy and reduce unnecessary downstream testing—turning fear-driven escalation into evidence-based reassurance.
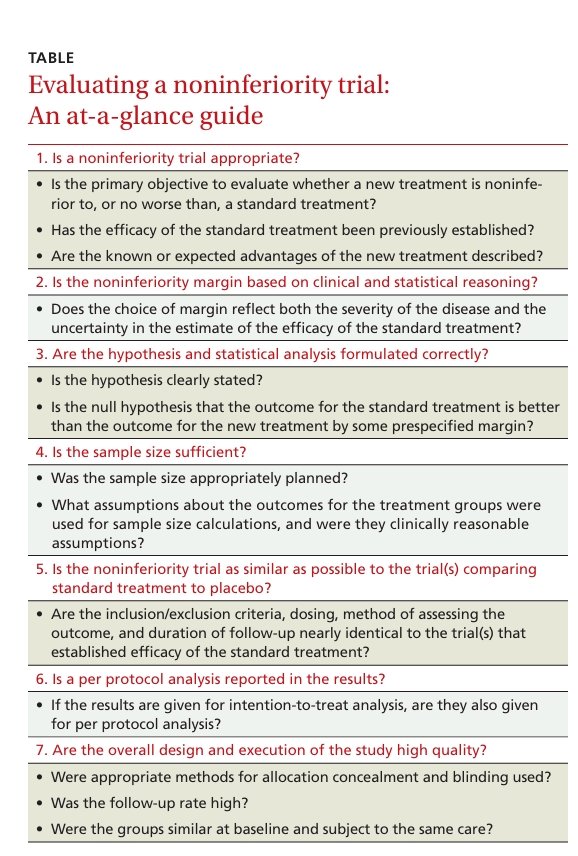
7 questions to ask when evaluating a noninferiority trial: While most physicians are accustomed to evaluating randomized placebo-controlled studies, many are less familiar with the purpose and takeaway of noninferiority trials
https://t.co/tDG5lcNlSF