Informazioni aggiornate sullo stato dell'arte del tumore del pancreas viste attraverso gli occhi dei pazienti
Italian Pancreatic Cancer Advocacy Organization
We have advocated for the same idea on the irinotecan vs Nal-iri for over three years. We are astonished to read somebody talking of a practice-changing protocol.
Read the news that NALIRIFOX got approved today by the FDA. Don’t be misled to believe that this represents any innovation. This is a pseudo innovation for which you get to pay more without any added benefits. We discuss this and other pancreatic cancer treatments in our recent @TheLancetOncol essay:
https://t.co/L9dx7qz2RZ
Our work is out on @JAMANetworkOpen ❗️
Is NALIRIFOX better than FOLFIRINOX as 1st line for metastatic #pancsm ❓
❎similar OS and PFS,
⚠️different clinical and 💰 toxicity
“I suppose we all thought that one way or another” https://t.co/ZeP0ionJV4
GIORNATA MONDIALE TUMORE DEL PANCREAS
Il nostro contributo con un video su un percorso di cura a cui tutti i pazienti dovrebbero avere accesso:
https://t.co/1qGcBKY3xO
Video realizzato con soli strumenti di AI
@headlighty@AISP_Pancreas
@ScaltritiLab Quello che medici e ricercatori classici non percepiscono è il valore dell'integrazione di biologia, medicina e tecnologie digitali. Nessuno sta pensando a riformare i piani di studio della facoltà di medicina ad esempio
In @JCOCCI_ASCO
Real-Time Identification of #PancreaticCancer Cases Using Artificial Intelligence Developed on Danish Nationwide Registry Data
https://t.co/qADuW9VXHw
The machine learning algorithm used here was able to identify high risk groups with a 10.1% risk of being diagnosed with pancreatic cancer within 1 year, anticipating diagnosis by ~5 months. The benefit to an algorithm like this is that it could be applicable in a primary care setting where patients often spend months in being worked up before a scan is ordered that identifies a pancreatic mass. A few months anticipation in diagnosis might be the difference between surgically resectable and unresectable cancers. Would love to see how real world implementation of algorithms like this result in meaningful stage shifts.
I wonder what postmortem @Penn is doing, given their past mistake: "UPenn told me that they’d had a meeting and concluded that I was not of faculty quality. When I told them I was leaving, they laughed at me and said, ‘BioNTech doesn’t even have a website.’"
@danielebanfi83 I pazienti con tumore del pancreas aspettano l'apertura del trial di Fase II sull'utilizzo di un vaccino mRNA specifico per i pazienti operabili e si augurano che presto ci sia una versione per i pazienti metastatici. Punti di vista diversi
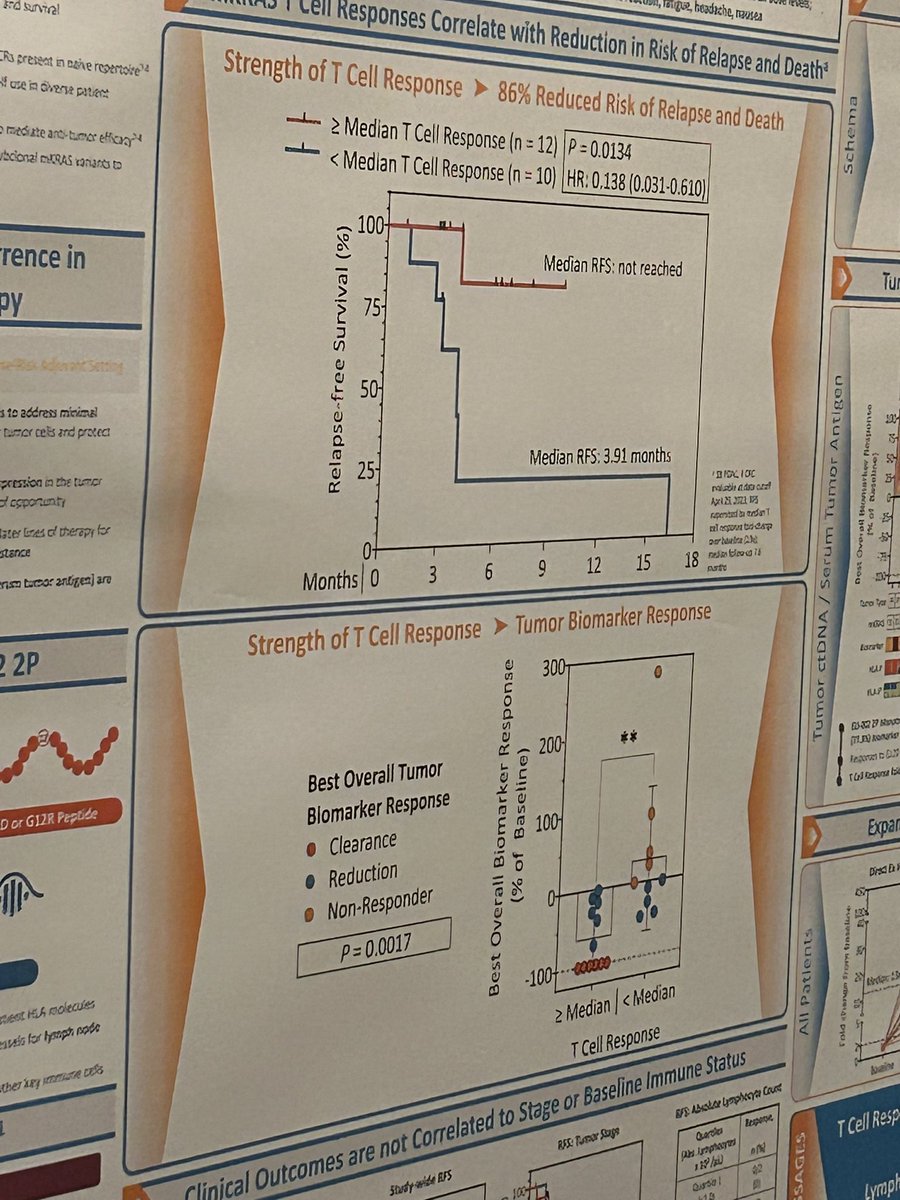
Crowds gather to hear @EileenMOReilly@MSKCancerCenter talk on the immunological correlatives of @ElicioTx amphiphilic lymph node targeted vaccine directed against mutant KRAS in surgically resected #PancreaticCancer (and #ColorectalCancer) with ctDNA or CA19-9 positive minimal residual disease (AMPLIFY-201).
The key data (albeit small numbers, limited follow up) is very similar to what was observed with mRNA vaccine in adjuvant setting - there is a subset of patients (around 50%) who generate potent T cell responses to the vaccine and these individuals do very well on the recurrence free survival scale. Then there is a subset (remaining 50%) that do not develop robust T cell responses and unfortunately those patients progress fairly rapidly. Now we need to figure - pre facto, not post - what differentiates the individuals who develop productive T cell responses from the ones who do not. #AACRPan23
@DrShubhamPant@MDAndersonNews
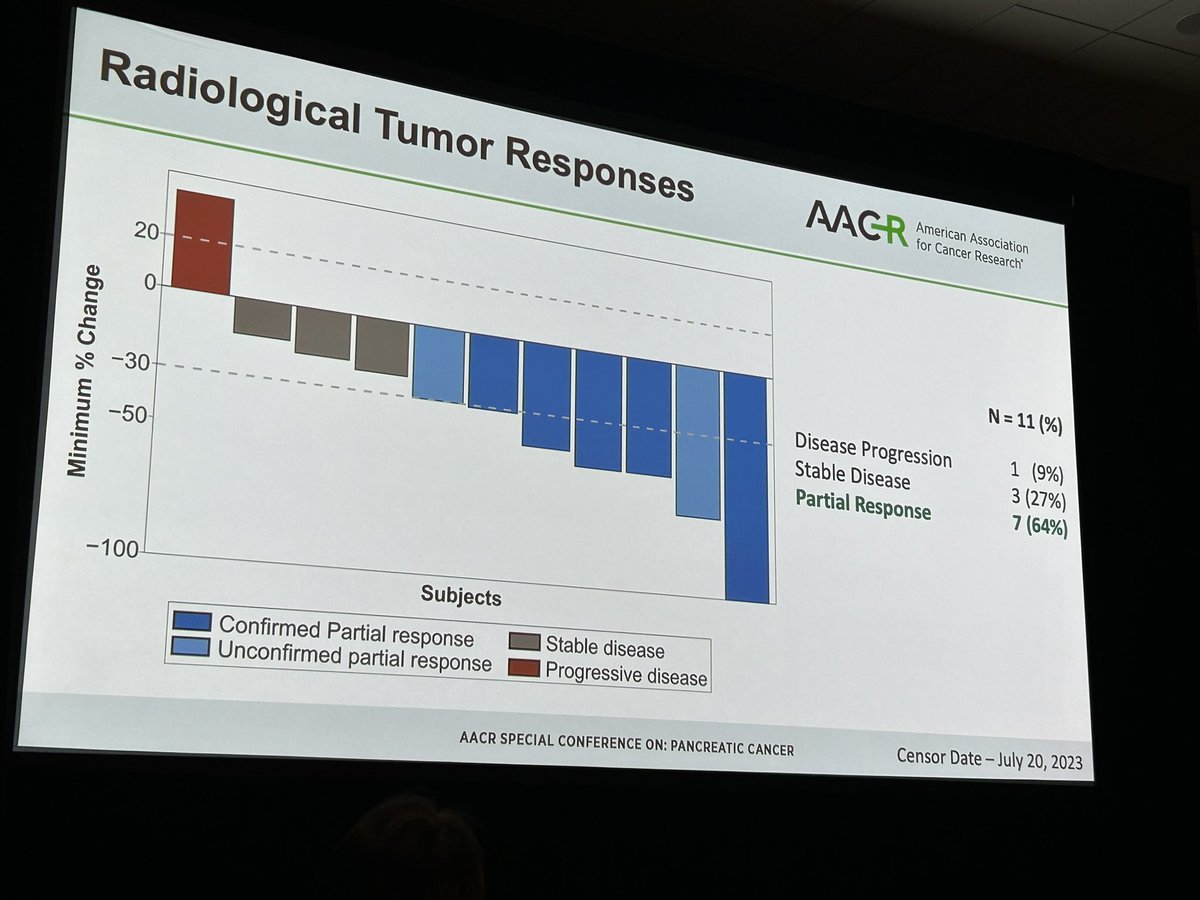
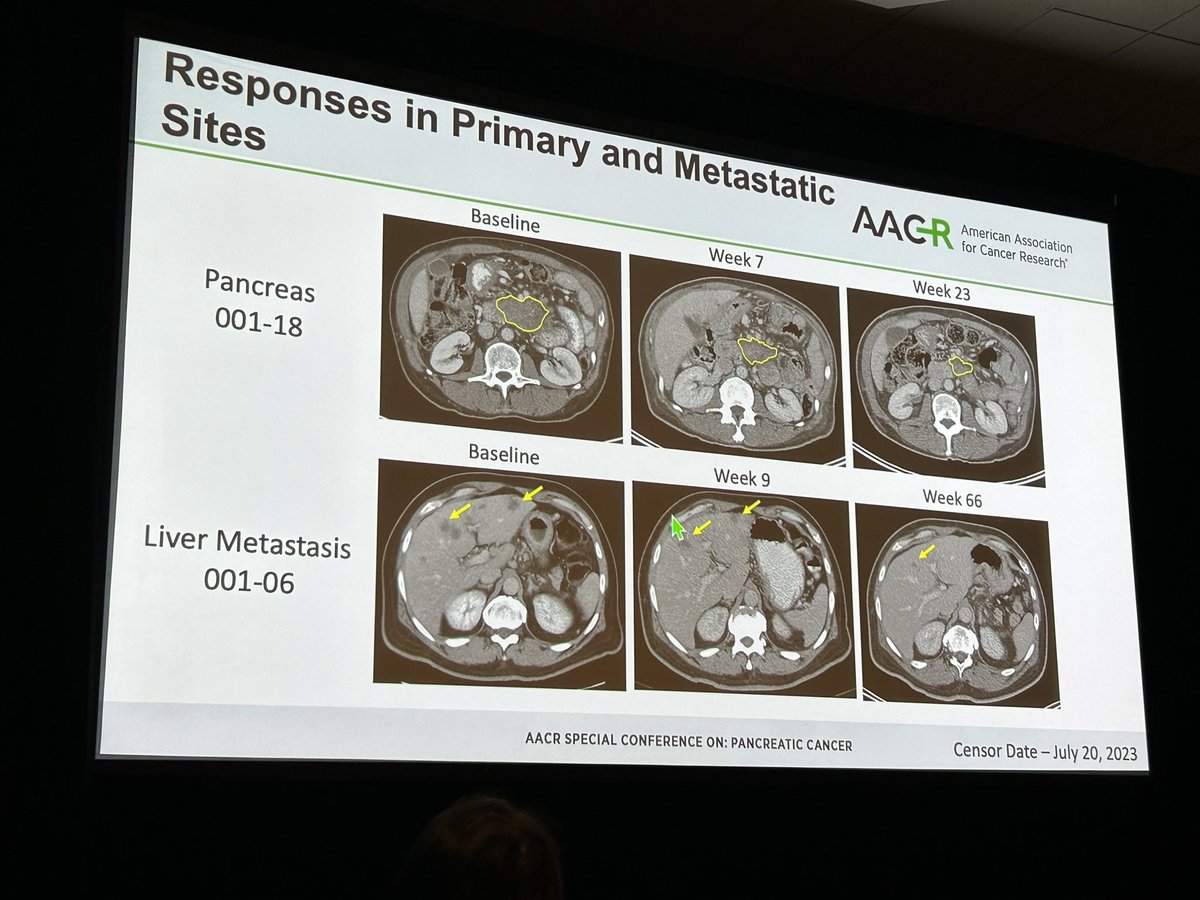
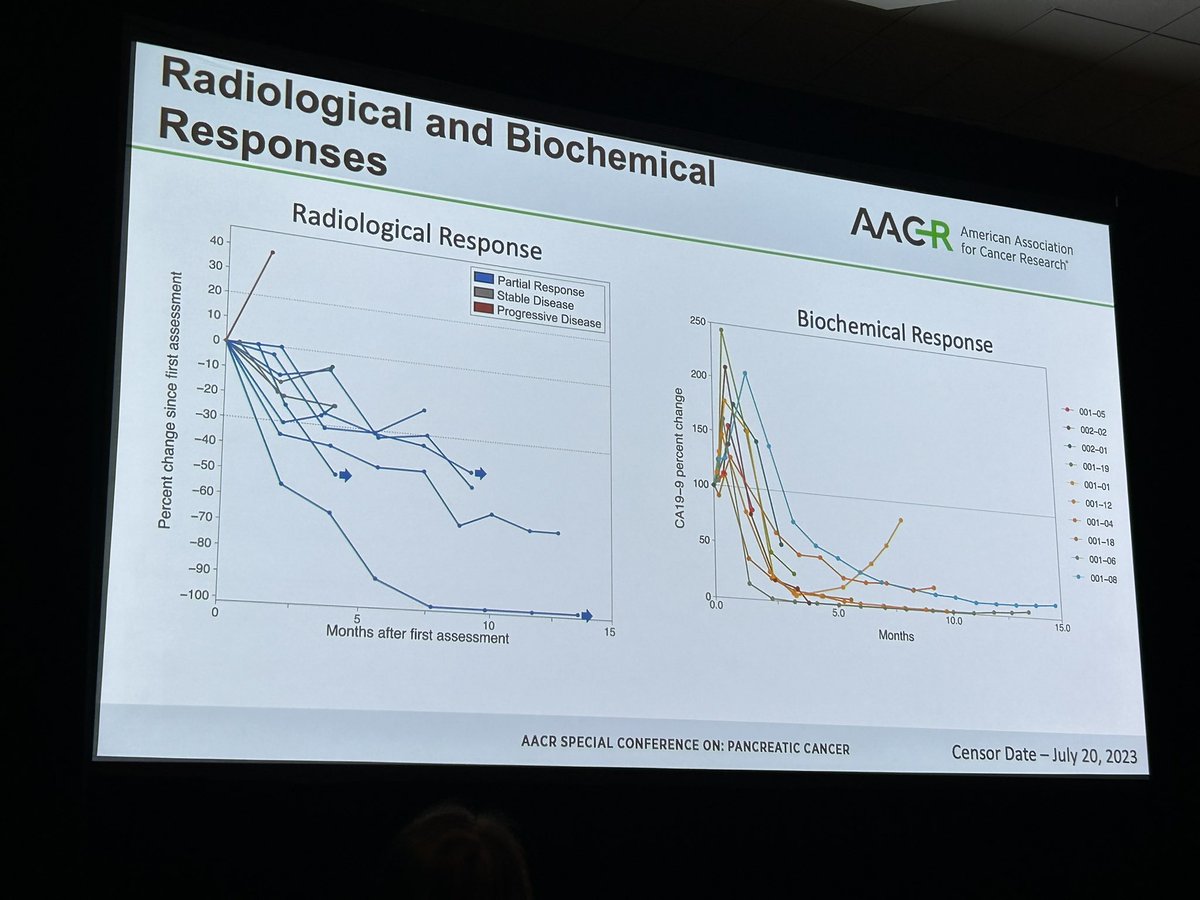
#AACRPan23 talk by Dr. Gulam Manji @columbiacancer on CheMoMETPANC 👉🏽 gemcitabine plus nab-paclitaxel + motixafortide (CXCR4 antagonist) + cemiplimib in advanced #PancreaticCancer. Responses observed in both primary & metastatic sites, with 64% partial responses & 27% stable disease. All patients in the trial received paired biopsies for deep correlative studies. Now moving to randomized phase 2.
#TumorBoardTuesday
Thursday wrap up!
@CentralParkWMD@ferguskeane2 led the discussion. More and more, molecular 🎯 different options in #PDAC.
✅HRD- PARPi; always want to go for curative surg if possible, but in met or 2L setting
✅KRAS- G12C small # of cases, G12D inhibs in trials
**Claudin18.2 emerging**
🆓#CME credit-2 quick❓
ALL CME 🔗: https://t.co/f2XlNam3Ty
CME eval🔗: https://t.co/0YtEgn3KRX
Word of caution on artery rsxn for PDAC: 1)These series reflect significant selection over decades where denominators not known. 2) Survival not clearly improved vs just chemo 3) high recurrence 4)high mortality and morbidity.@bjs @DrJashDatta https://t.co/Fi8vlt1fDy