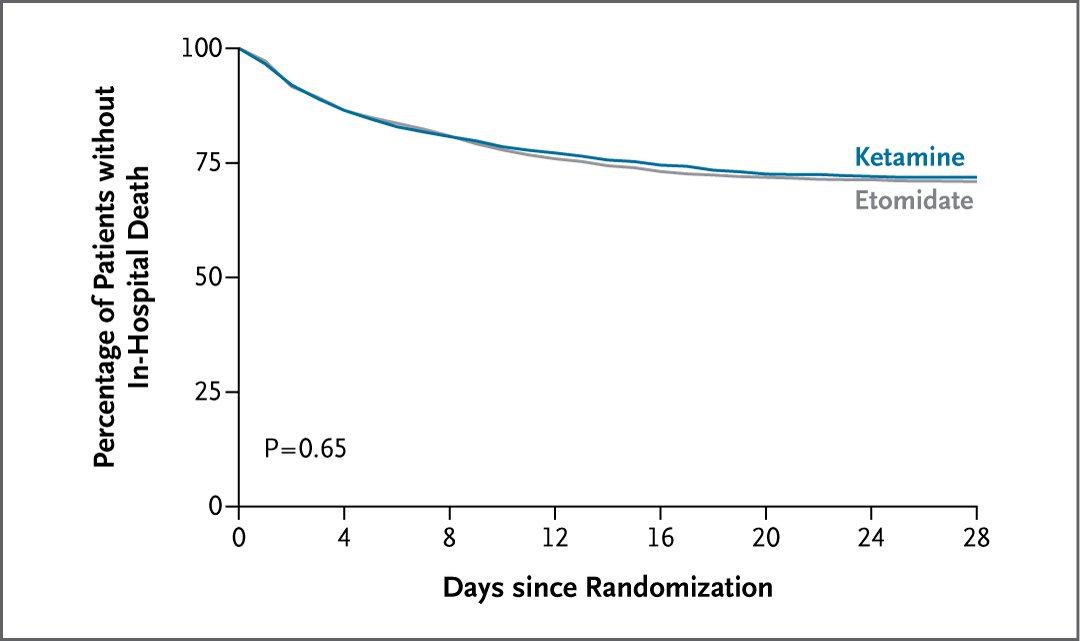
When someone is critically ill and needs a breathing machine, doctors commonly choose between ketamine and etomidate to put them to sleep. Which is better? We are excited to finally share the results of the RSI trial! @UABNews@PCCRG@UABPulmonary
@ADAlthousePhD@dnunan79 I also think we should carry the KM curves out to the end of the cohort’s life expectancy to remind us that we all one day shall die. To paraphrase the Teacher “I searched for a large absolute risk reduction but the outcome still later occurred. This too is vanity”
🔬@UABPulmonary Drs. @SGandotraMD, @DerekRussellMD
David Page, and Micah Whitson report in @NEJM that preoxygenation with noninvasive ventilation, as opposed to O2 mask, results in lower incidence of hypoxemia in adults undergoing tracheal intubation.
📕https://t.co/NDZS9S9cQG
EMCrit 377 - Breaking News - The PREOXI Trial changes everything for Preoxygenation in Intubations in the Critically Ill! I interview the lead authors and give my RECs.
[#FOAMed]
I've been advocating for this for years and now we have a beautiful trial...
https://t.co/xvLuUXCiPm
Since @CritCareReviews and #CCR24 have had a couple of win ratio analyses, here’s a little plug for a video I made with @CMichaelGibson a few years back that is meant to be an accessible explainer of how it works.
Please excuse my hair. It was a different time.
RT is VERY busy during RSI of critically ill adults... is it worthwhile to routinely ask them to also get a mask for NIPPV during preoxygenation? Prior smaller studies suggested NIV preox might safely reduce hypoxemia, but data mixed/inconclusive. Excited for PREOXI trial!
Our friends from @PCCRG are back too!
Our 5th major trial result presentation at #CCR24 is PREOXI:
Non-invasive ventilation vs facemask oxygen for preoxygenation in the critically ill
@JonathanCaseyMD & @KevinGibbsMD presenting the results
Register at https://t.co/1w9GNbBdCG
What is the PREOXI study?
Our methods 🔬 are hot 🔥 off the press 📃.
In the DoD-funded PRagmatic trial Examining OXygenation prior to Intibation (PREOXI), patients undergoing emergency intubation will be randomized to a standardized NRB mask versus a pressure mask (CPAP, BPAP) for preoxygenation.
Keep your eyes peeled this spring as we will answer this best-practices question.
https://t.co/KBsLCi5AP5
#emergency #emergencymedicine #icu #criticalcare #airway #ems #ambulance #sick #trauma #medic #combat #combatmedic #military #army #navy #airforce #foamed #foamcc #science #research #data #armyemdoc #medtwitter #medx
@ADAlthousePhD The answer might be Natalie Merchant’s Wonder since I think Carnival was the bigger hit. Nope, changed my mind: Rest of my Life by Unwritten Law. So much better than Seeing Red. But got me thinking: would you say that POTUSA’s Lump or Peaches was their “one hit”?
Miss the @PCCRG DEVICE trial, presented by Matthew Semler & Matthew Prekker at the Critical Care Reviews Meeting #CCR23 last week?
It was simultaneously published in @NEJM
https://t.co/3MobsWJfmh
Here, the trialists briefly explain the results
@ADAlthousePhD @WamsleyLab Agree... still, stopping huge trial early is much harder than just designing smaller trial. TBH, I get angry too. Lots of disingenuous/unrealistic power calculations that look suspiciously post-hoc or contrived out there. But suboptimal power can still be valid I think.
@ADAlthousePhD @WamsleyLab I get what you're both saying... I mean, ur not wrong, in ideal world. I even agree sometimes. But: 1. when lit suggests larger effect, can this b misplaced precision? 2. does this mean all studies testing something w tiny MCID need ~infinite pts? Can't incremental data b useful?
@anandiyermd @toddrice_ICU As non-statistician, I worry my language for such things could be not precise enough (esp using 2 lay language) so I recommend @ADAlthousePhD and @VR_Cornelius for better stuff... & if they have any tweetorials on Forest Plots of 95%CIs to link to, would rec taking a look.
@anandiyermd @toddrice_ICU Last tweet on this: However, our data does suggest benefit from VL even in these subgroups, just not within 95% confidence. In fact, the effect estimate for operators with >100 airways is still greater than the 5% MCID effect we were shooting for in this trial.

















![emcrit's tweet photo. EMCrit 377 - Breaking News - The PREOXI Trial changes everything for Preoxygenation in Intubations in the Critically Ill! I interview the lead authors and give my RECs.
[#FOAMed]
I've been advocating for this for years and now we have a beautiful trial...
https://t.co/xvLuUXCiPm https://t.co/ScZZPkabN2](https://pbs.twimg.com/media/GP9NhyYXQAAr6wb.jpg)