Zaniburtinib is dosed at 320 mg once daily or 160mg twice daily. This clinic prefers twice daily because that’s what the clinical trial (ASPEN) trial did but will change to once daily if patients have neutropenia because once daily causes less neutropenia
Patients with WM will often have two M-spikes on SPEP because IgM exists as monomer and pentamer so both with show up. However about 5% of patients will have a biclonal disease and have a second monoclonal antibody that isn’t the same IgM so confirmation is needed
Just out!! In @NEJM - Our randomized trial in myeloma (ENDURANCE trial) shows limited duration of lenalidomide maintenance is just as good as indefinite therapy, with less side effects!!! @eaonc@theNCI
Implications are HUGE. This is a drug we spends billions on each year:
-Less side effects
-Less second cancers
-Similar overall survival
-Less cost
@myelomaMD@Myeloma_Doc@SagarLonialMD
National NCI funded trial led by @eaonc and joined by @ALLIANCE_org & @SWOG
https://t.co/k8nGWeSA03
Ten reasons why I would favor the gedatolisib doublet (fulvestrant/geda) over the triplet with palbo:
1) VIKTORIA-1 was not designed to compare the two geda arms — yet, the PFS improvement over fulvestrant was similar with or without palbo (HR 0.24, HR 0.33, with overlapping 95%CI)
2) ORR was also similar, 31% vs 28%, consistent with the idea that palbo does not add much activity
3) there is no OS advantage from adding palbo, and the current favorable OS trend is similar in both geda arms (HR 0.69 and 0.74)
4) the PIK3CAmut sub-study of VIKTORIA-1 also confirmed this pattern, with no apparent benefit from the addition of palbo to the doublet
5) using palbo after prior CDK4/6i has failed to improve outcomes in two randomized trials (PACE, PALMIRA).
6) the triplet clearly adds toxicity. >50% grade 3 neutropenia (0% without palbo) and higher rates of severe stomatitis and nausea
7) treatment-related deaths only occurred with the triplet, with two grade 5 toxicities (vs none with the doublet)
8) the triplet adds logistic burden. A nearly weekly IV infusion and a monthly shot are already burdensome. Adding a third anticancer drug with distinct route of administration and frequent requirement for dose holds further adds complexity.
9) the triplet further adds costs
10) we treat this disease to achieve disease control with preservation/improvement of QoL. Adding a third drug which adds toxicity and may worsen QoL, without clear long-term benefit, does not sound like a good deal
Today I learned that MDS/MPN is associated with pyoderma gangrenosum (PG). Up to 8% of PG patients have an underlying blood cancer. The mechanism is speculated to be that the cancerous myeloid progenitor cells causes dysfunctional/overactive neutrophils and monocytes, causing PG
Nice work @LuisRaezMD Agree about increasing testing, fast if you use plasma ct DNA. new 4th gen EGFR TKIs have activity against C797 series mutations. Assuming 1 or more achieve approval, this will broaden the potential of personalizing therapy: On target vs Bypass (Off target)
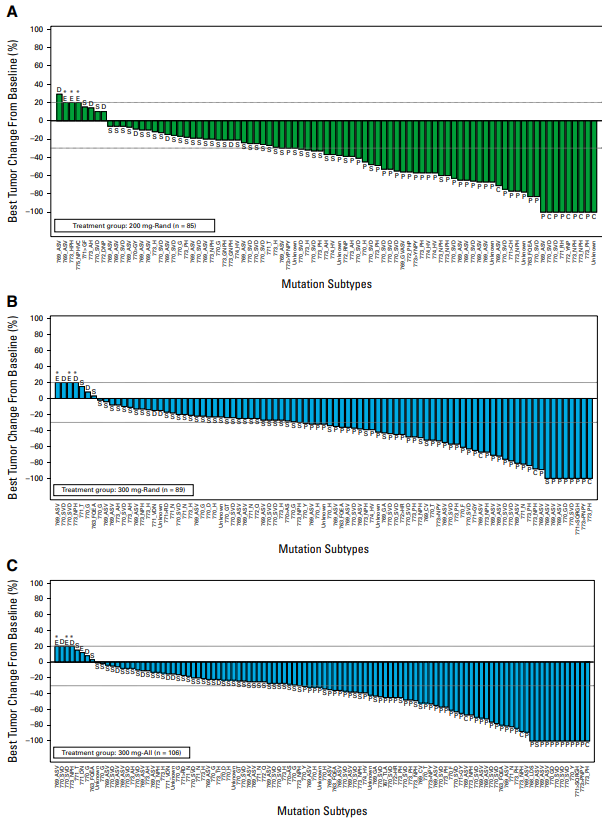
WU-KONG1B for EGFR exon 20 @JCO_ASCO from James Yang, Pasi Jänne et al.
Take: Exon 20 is the hardest EGFR to treat. Sunvozertinib orally joins ami and dato. ORR ~45%, DOR ~13m. Waterfall plots easy to read from far away. More options for @EGFRResisters@EgfrUk#LCSM #thoraciconcology
Agree @TejasPatilMD regarding consolidation RT in E-SCLC. Worth remembering that original trial published (Slotman 2015) had mainly patients with residual disease only in the chest. Hence benefit of RT. This latest trial likely the proverbial "Nail in the Coffin"! ⚰️
Negative results from phase 3 ZEAL-1L trial @JTOonline. Pts with NSCLC completed induction chemo-immunotherapy, randomized to pembro maintenance with PARP inhibitor niraparib or placebo. No difference in PFS with niraparib (mPFS 4.4min both arms).
https://t.co/8VcILiv4RQ
Characterization of EGFR mutant NSCLC transformed to SCLC (n=45) @JTOonline. 70% received EP alone, 23% had EP combo (IO/TKI). Combo PFS 7.5m vs 2.8m (many confounders). DLL3+ in 88%, B7-H3+ in 67% but prior reports show poor RR to tarlatamab. ADCs here?
https://t.co/SEXfsdU0DC
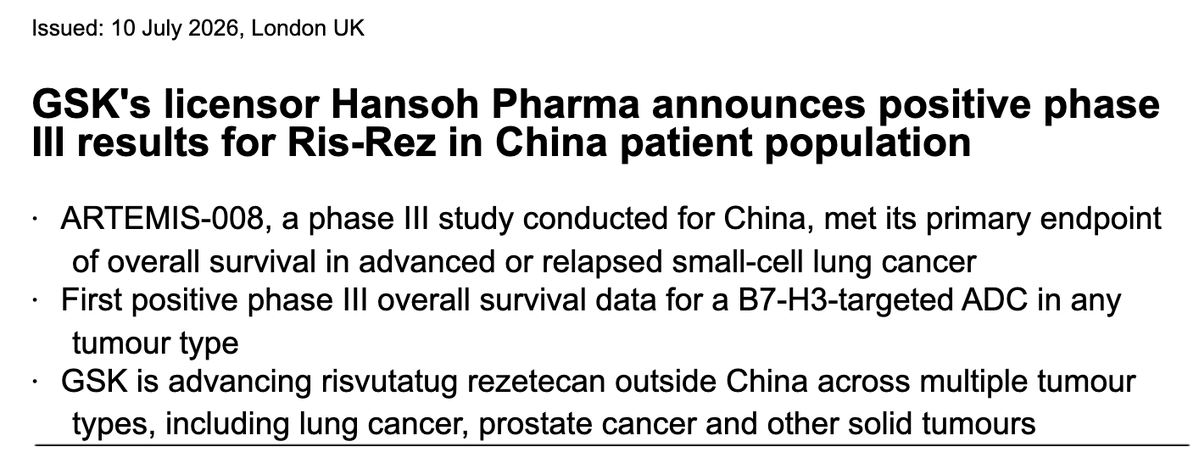
GSK announces positive results from phase III ARTEMIS-008 trial. Risvutatug rezetecan (Ris-Rez), a B7-H3 ADC, shows superior survival over topotecan in pts with relapsed SCLC. Await full dataset but would still favor tarlatamab here. @OncoAlert
https://t.co/clzI5Ft8Dr
🔥off the press🔥
Pan-Asian adapted ESMO Clinical Practice Guidelines for the diagnosis, treatment, and follow-up of patients with hepatocellular carcinoma
@ESMO_Open
https://t.co/LiWMffR3ZT
👏great consensus between east & west
@myESMO
Study of first line ifebemtinib (FAK inhibitor) plus garsorasib (KRAS G12C inhibitor) in KRAS G12C NSCLC @LancetRespirMed. RR 82%, mPFS 22.3m, mOS 27.8m. 24% had G3+ TRAEs (proteinuria, diarrhea, anemia, HTN, pneumonia). Small numbers, but encouraging.
https://t.co/JWhBSmHe3t
A clearly problematic study has now lost its status as valid scientific evidence. After the Nature Medicine retraction, the related ASCO abstract was also retracted from JCO.
Retractions are no longer rare, but seeing a meeting abstract formally retracted is still not a common occurrence. Hopefully, this case will serve as a lesson.
Among patients with resected ALK-positive non–small-cell lung cancer, 2-year disease-free survival was higher with the ALK inhibitor ensartinib than with placebo. Grade 3 adverse events were more frequent with ensartinib. Full ELEVATE trial results: https://t.co/JbfYGnXSyC
Post hoc analysis of PACIFIC (durvalumab after CRT for stage III NSCLC) @TheLancetOncol shows 40% used PPIs at baseline; with durvalumab, PFS 9.4m vs 17.2m with no PPI (HR 1.57) and OS 33m vs 57.9m (HR 1.66). No difference with placebo. Similar PFS findings with antibiotics.
Join us at #STOPCancer2026 for two days of cutting-edge discussions on precision medicine and novel cancer therapeutics. Looking forward to learning from colleagues and contributing to the lung cancer sessions. See you in NYC!
A historic day for solid tumor oncology.
China has approved satri-cel (CLDN18.2 CAR-T) for advanced gastric/GEJ cancer, making it the first CAR-T therapy ever approved for a solid tumor. For years, CAR-T has transformed hematologic malignancies while solid tumors remained left in the dust.
📊 CT041-ST-01 (3L+ CLDN18.2+ gastric/GEJ cancer) in the Lancet
• Median PFS: 3.25 vs 1.77 months (HR 0.37)
• Median OS: 7.9 vs 5.5 months (HR 0.69)
• 18-month OS: 20% vs 10%
• Demonstrated superiority over physician’s choice therapy in a heavily pretreated population.
The absolute numbers are not dramatic, but that isn’t the point.
This is the first regulatory approval of a CAR-T for a solid tumor.
Also notable: this happened in China, not the United States.
As China continues to accelerate development of cell therapies, ADCs, and other oncology platforms, it is increasingly becoming the site of first-in-class innovation.
Satri-cel may ultimately be remembered less for the 2.4-month OS gain and more for what it represents:
The beginning of the solid tumor CAR-T era.
@Onco_Nexus@OncoAlert@TheGutOncLab
https://t.co/gon4I3udIR