Among statin-intolerant adults at high cardiovascular risk, #BempedoicAcid was associated with reduced risk of #VenousThromboembolism, including deep vein thrombosis and pulmonary embolism.
https://t.co/AOeVP2X8Xt
@ShahzebKhanMD@JavedButler1@f2harrell Congratulations @ShahzebKhanMD
We conceived of this approach for ASCVD therapy in 1994, evaluated in UCLA CHAMP: ⬆️ use, adherence, outcomes (GWTG)
Proposed for quadruple GDMT in HFrEF in 2020 with @SJGreene_md + @JavedButler1 with subsequent RCTs
Look forward to your results
@echo_batman@maybeadoc1983@drjohnm The comparator solely guided by the evidence
For HFrEF, evidence/guidelines supported ACEI over ARB. If an ARB was selected would have been criticized since ARB had failed in RCTs to be non-inferior to ACEI
In HFpEF, ARB > ACEI. PARAGON-HF S/V vs valsartan 160 mg bid tested
@PLooserMD@naderjo@drjohnm Unblinded, ⬆️ SAE rates, small # of centers over 10 years, p=0.04, and yet the DSMB recommended to permanently stop 2nd RCT
Now what if the trial had been 10x larger, double blinded, SAEs less than control, RRR for CV☠️ similar magnitude ⬇️, and p=0.00008
Still require 2nd RCT?
An adequately powered RCT to evaluate similar outcomes as PARADIGM-HF would cost ~$300 to $450 million
You would need patients willing to volunteer/consent, investigators willing to randomize, and IRBs willing to approve
When most across the world already see ARNI as Class 1 https://t.co/iwjv0Y4wBe
Among patients with #Type2Diabetes and #ChronicKidneyDisease, finerenone reduced risks of cardiovascular and kidney events and promoted regression of #CKM syndrome regardless of baseline stage. https://t.co/jHZraJspjN
@crowanmd@drjohnm Concur
Primary endpoint met non-inferiority but not superiority (HR 0.94, 95% CI 0.86-1.03)
Secondary endpoint: ☠️ or CV 🏨 HR 0.91 [95% CI, 0.84 to
0.99]), P=0.024
The authors’ conclusions:
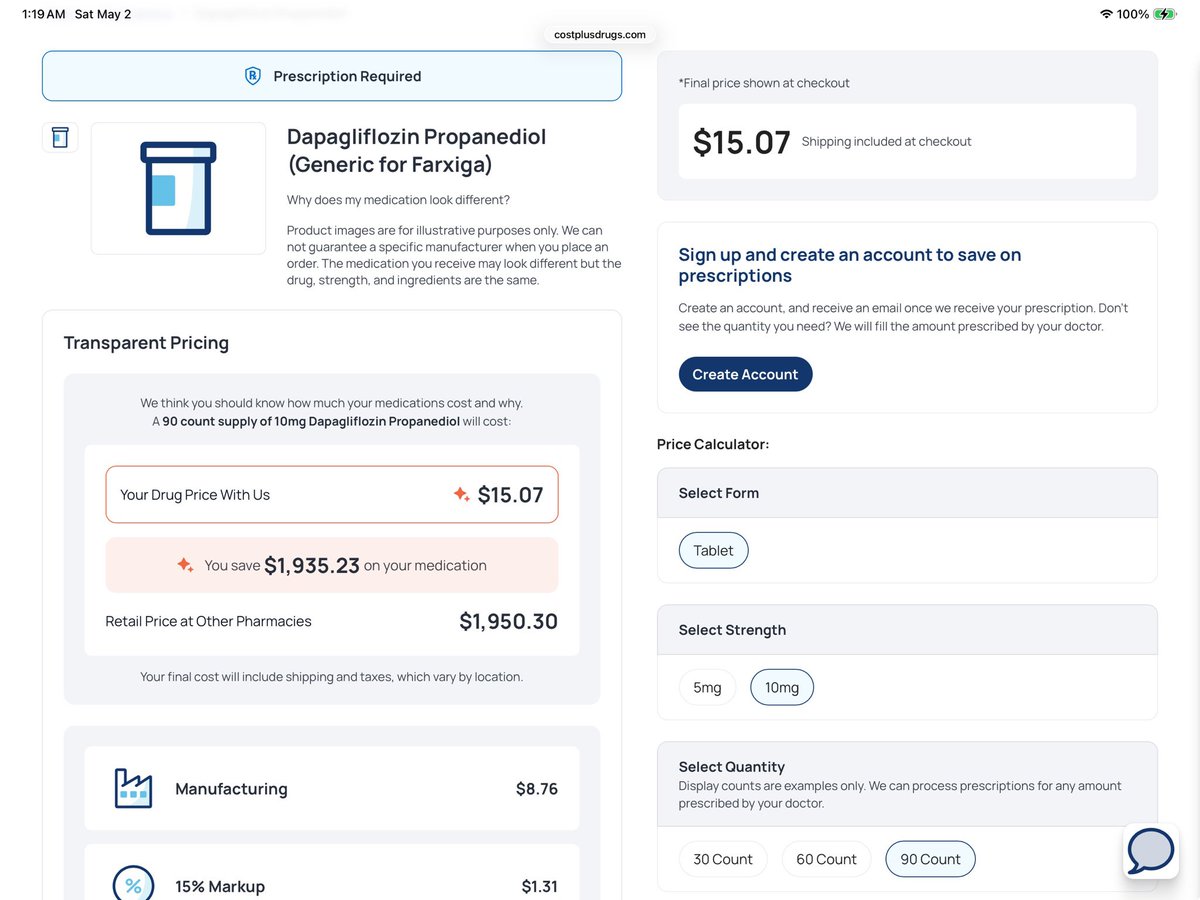
@CircOutcomes@jasonwasfy@kardiologykazi@laurapco Timing and drug pricing is everything
In 2026, with low cost generic pricing SGLT2i and ARNI are cost saving (cost dominant) to ICER <$5,000 per QALYs saved in HF
🌍 Heart failure affects > 64 million people worldwide + remains a major global health challenge.
👉This review summarizes the latest data on HF epidemiology, trends, and future challenges.
https://t.co/xJipGll9Or
@EJHFEiC@AmrAbdin10@GiuseppeGalati_@HanCardiomd
@naderjo@drjohnm No RCT MI+cardiogenic shock
➡️
DanGer Shock: 14 centers, 355 patients, 185 events, p=0.04
➡️
RECOVER IV terminated following DanGer +results
DSMB: equipoise no longer exists
Recommended permanent discontinuation

Judged unethical to keep randomizing to a no-Impella arm
@Sensible__Med@AnilMakam 🤣
Contrived with no valid basis to assert enalapril 10 mg bid is sub therapeutic or that any dose of valsartan is a more valid comparator. Playing games as if HFpEF and HFrEF are the same.
Hopefully can do something better with “appraisal” than this
@crowanmd@drjohnm The OVERTURE trial was not powered for CV☠️ but showed the potential for neprilysin inhibition in HFrEF
A better agent (S/V) w/ less angioedema risk was developed
Tested in PARADIGM-HF
Proven to
⬇️ CV☠️/HF🏨
⬇️ CV☠️
⬇️ AC☠️
As well or better tolerated vs enalapril
@crowanmd@drjohnm Here is the meta-analysis which includes IMPRESS, OVERTURE, and PARADIGM-HF in HFrEF
⬇️ CV☠️/HF🏨
⬇️ AC ☠️
Combined neprilysin/RASi, 2 agents, 3 trials ➡️ benefit in HFrEF
OCTAVE was 24 week hypertension trial for BP control and Angioedema rate. Not CV events.
@AnilMakam It was a double blind RCT, not open label
Tested vs a gold standard agent/dose
The run in was shown to have no impact on efficacy, even if excluded pts imputed back in
And then need to write off PIONEER-HF with no run in, conducted by the TIMI group as also somehow biased
@drjohnm PS:
In PREVAIL there were n=33 primary endpoints at 26 month mean f/u
Compared to PARADIGM-HF of n=1251 CV ☠️ endpoints
20% RR ⬇️ vs ACEI control, p=0.00008
Not all “just one” trial are the same in terms of strength and meeting FDA criteria for “substantial evidence”








![gcfmd's tweet photo. @crowanmd @drjohnm Concur
Primary endpoint met non-inferiority but not superiority (HR 0.94, 95% CI 0.86-1.03)
Secondary endpoint: ☠️ or CV 🏨 HR 0.91 [95% CI, 0.84 to
0.99]), P=0.024
The authors’ conclusions: https://t.co/CtzjjuS18o](https://pbs.twimg.com/media/HJ-YDbebAAAVfUX.jpg)