Below are the links to important recent papers on arterial switch operation published in the Journal of Thoracic and Cardiovascular Surgery.
https://t.co/MiEMNy4Ur5
https://t.co/3dQQN4mhhw
https://t.co/lTNw3kNDve
https://t.co/GMjPqNPIKD
🫀 #CardioNugget: Flail Gap vs Flail Width in MR
📍 Flail Gap
➡️ Distance between the flail leaflet tip and the coaptation line
➡️ Think: “How far is the leaflet flying into the LA?”
🔴 Larger gap = more severe MR
✅ MitraClip-friendly: <10 mm
📍 Flail Width
➡️ Medial–lateral extent of the flail segment
➡️ Think: “How wide is the damaged portion?”
🔴 Wider segment = more complex repair
✅ MitraClip-friendly: <15 mm
🎯 Why it matters?
Both help determine severity + feasibility of transcatheter repair (e.g., MitraClip)
#CardioNuggets #MedEd #TEE #MitraClip
Recently published in #JTCVS Techniques: A case report describing the surgical management that achieves reduction and stabilization of the mitral annulus in a 5-month-old boy. Learn more: https://t.co/ASyDfZgP8H
@konstantinov_ie
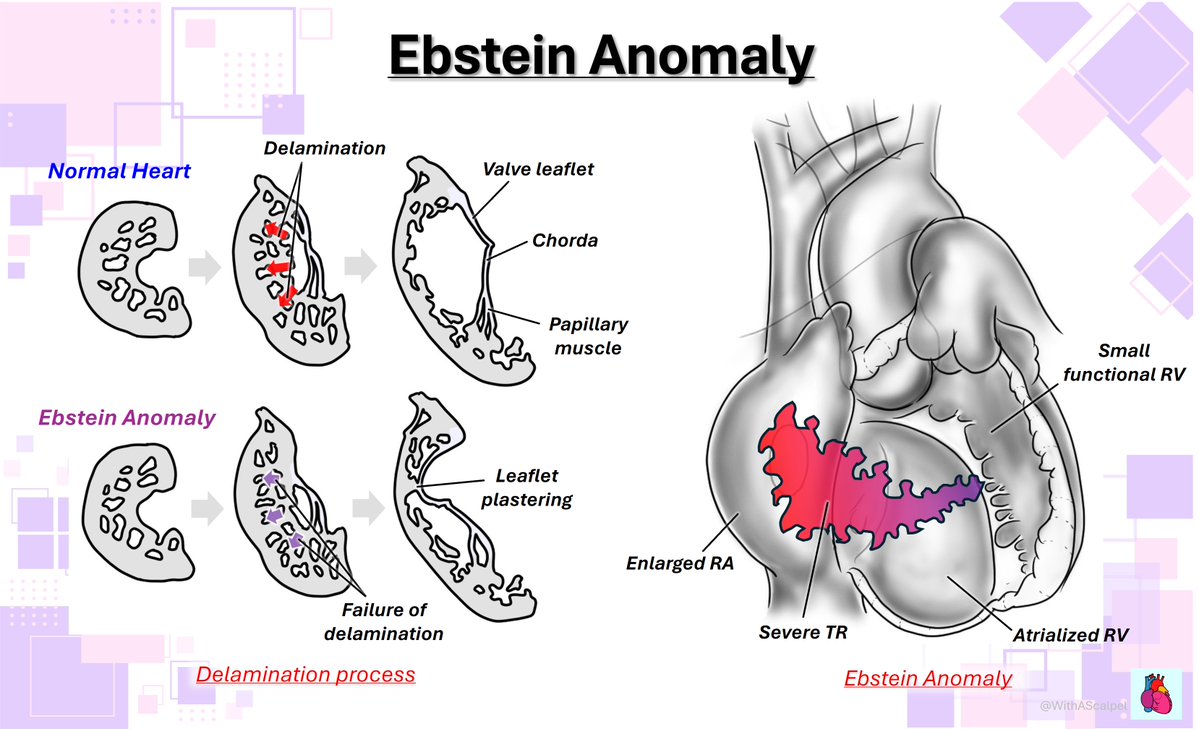
Ebstein Anomaly: Atrialized RV and Tricuspid Malformation
👉Failed delamination of the tricuspid valve results in apical displacement of the septal and posterior leaflets, creating an atrialized proximal RV.
#CardioNugget 🫀
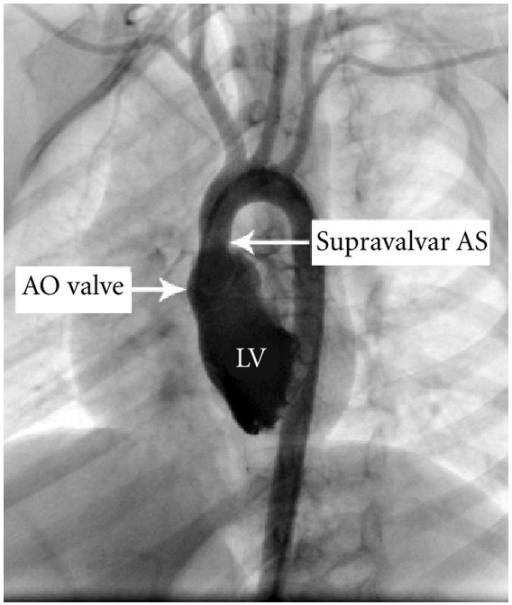
Supravalvular AS = jet direction matters
👉 Narrowing above aortic valve (classically in Williams syndrome)
👉 High-velocity jet hugs aortic wall → Coandă effect
👉 Jet preferentially enters brachiocephalic (right innominate) artery
⚡ Clinical clue:
RIGHT arm BP > LEFT arm BP (not coarctation!)
💡 Why?
More kinetic energy directed into right-sided arch vessels
#EchoBoards #Cardiology #Hemodynamics #CongenitalHeartDisease
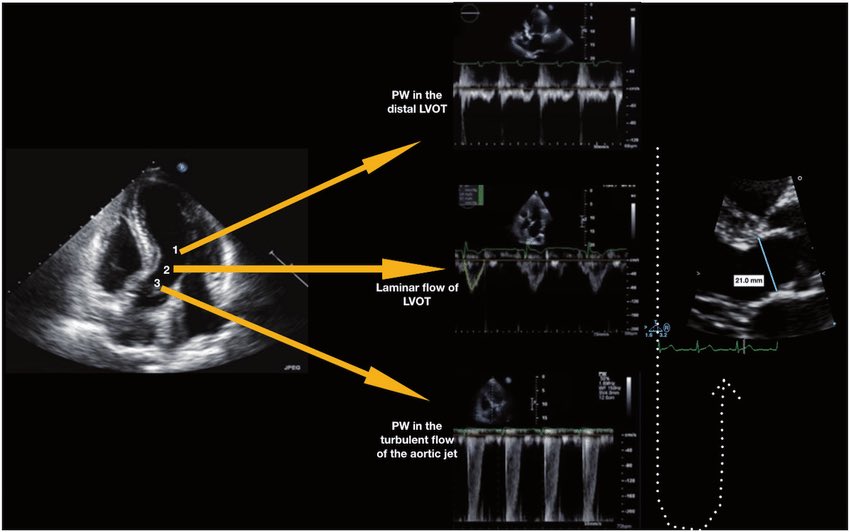
Understanding Intracardiac Blood Flow: Laminar vs. Disturbed Flow
Blood flow in the heart follows distinct patterns, influencing hemodynamics and disease progression.
⚫ Laminar Flow (Top Image) – Smooth, parallel streamlines with uniform velocity, seen in normal arteries and heart chambers. This pattern ensures efficient oxygen delivery and minimizes endothelial stress.
⚫ Disturbed Flow (Bottom Image) – Occurs beyond stenotic valves, regurgitant orifices, or intracardiac shunts. Chaotic vortices and eddies increase turbulence, shear stress, and risk of endothelial damage or thrombus formation.
⚫ Clinical Example: In Aortic Stenosis, blood is forced through a narrowed valve, creating a high-velocity jet. This jet remains laminar until it exits the stenotic orifice, where turbulence forms. Doppler echocardiography detects this as increased peak velocity and pressure gradients, helping assess stenosis severity.
⚫ Another Example: In Atrial Septal Defect (ASD), left-to-right shunting of blood through the septal defect leads to disturbed flow, visible as color Doppler turbulence in the right atrium. This abnormal flow pattern can cause right heart volume overload over time.
Recognizing these flow patterns is crucial in echocardiography and hemodynamic assessments.
In the spirit of our valve repair series, here another Single patch technique for mitral valve repair of MV Endocarditis, of the posterior leaflet and annulus, which of course I have learned Prof. El Khoury. More to follow. @GebrineK
A minimally invasive alternative to open heart surgery is gaining popularity—but some find their new valves don’t work as well or last as long as they hoped. 🔗 https://t.co/0lFyWeqbH3
Glenn Circulation #1: Principle of Stage 2 Palliation
👉The Glenn diverts SVC flow directly to the pulmonary arteries, removing “stolen” pulmonary blood flow from the systemic ventricle.
👉Pulmonary blood flow becomes passive and non-pulsatile, with Glenn flow largely determined by SVC return.
👉Oxygen saturation depends on both flow and resistance: ↓SVC return or ↑PVR can reduce PBF and cause desaturation.
Dr Eugene Braunwald's death has evoked much less reponse on #MedTwitter than I would have believed possible
This is the man Indian doctors between 40-50 years of age at present worship as the Harrison of cardiology
#MedTwitter#NeuroTwitter#CardioTwitter
Sinus Venosus ASD: Surgical Anatomy and Repair
👉Sinus venosus ASD is located near the caval–atrial junction and is commonly associated with PAPVR.
👉Surgical repair requires redirection of anomalous pulmonary venous return to the LA while maintaining a non-obstructed SVC pathway.
👉Depending on the anatomy, the Warden procedure or a two-patch repair is typically used.
Intraoperative Management for Valve-Sparing Aortic Root Replacement
VSARR offers 83.5% 15-year survival — surpassing the Bentall procedure. 🫀 Comprehensive intraoperative TEE is the anesthesiologist's essential tool for pre- and post-bypass assessment
https://t.co/26WshRmYtP
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → https://t.co/oCXGNgWsPF
👉 Pasipoularides et al. Am J Physiol 1984 → https://t.co/cfvNMpEgzG
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → https://t.co/lRVjLuYMEs
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → https://t.co/rf7l2FQUs4
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → https://t.co/avke1qOy4x
👉 Zoghbi et al. Circulation 1986 → https://t.co/KFiChfBNuc
👉 Oh et al. JACC 1988 → https://t.co/1C8sHRSMPq
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → https://t.co/U3hXFns4jx
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → https://t.co/iu07xBTwQS
👉 Hahn & Pibarot. JASE 2017 → https://t.co/uqgcv8kzO7
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni@JaeKOh2@ottoecho@WilliamZoghbi@ASE360@EACVIPresident@NephroP@iamritu@PPibarot@hahn_rt@MAecocardio@SISIACOficial@SONECOM_AC@VazyurVasquez@Cardiotweets83@HEARTof_echo@echobasics