💡 ICYMI from #ASCO26: The addition of Radium-223 fails to improve symptomatic skeletal event–free survival in #renalcellcarcinoma with bone metastases: https://t.co/0zxJGtLvrh
Why do VEGFR-TKI + IO combinations produce impressive responses in ccRCC but often fail to achieve the long-term durability seen with dual checkpoint blockade? Check out our lab's latest in @Cancer_Cell led by the incredible Lyn Vuong!
https://t.co/ASvkCpDzQW
Great presentation by Dr. Pavlos Msaouel. Panitumumab-based EGFR blockade in SMARCB1-deficient renal medullary carcinoma: ORR 53.9% (15.4% CR) and mOS 9.5 mo in heavily pretreated pts, far exceeding historical benchmarks. Wild-type EGFR dependency as a new therapeutic vulnerability in this rare, aggressive disease. #ASCO26 #RCC @OncoAlert@ASCO@OncBrothers
#ASCO26 GU Oncology Spotlight 🚨
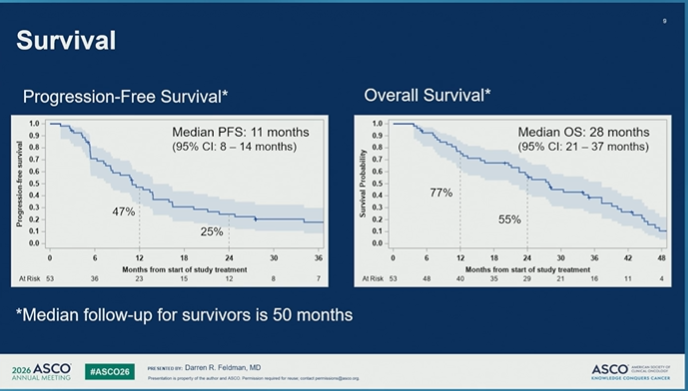
🔬 Abstract 4521 | CaboNivo in non–clear cell RCC
Final results of phase 2 cabozantinib + nivolumab in patients with non–clear cell renal cell carcinoma
Presented by Darren R. Feldman, MD
@ASCO@OncoAlert
Important final dataset in a difficult RCC space.
Non–clear cell RCC represents a biologically diverse group of kidney cancers, often with fewer prospective data and historically poorer outcomes than clear cell RCC.
🔵 Study design
Investigator-initiated phase 2 study:
➡️ cabozantinib 40 mg daily
➡️ nivolumab 240 mg q2w or 480 mg q4w
Cohort 1 included:
• papillary RCC
• FH-deficient RCC
• unclassified RCC
• translocation-associated RCC
Chromophobe RCC was evaluated separately and closed early for inefficacy.
🟢 Final efficacy signal
With longer follow-up of ~50 months, CaboNivo reaffirmed antitumor activity in non–clear cell RCC.
In cohort 1:
• N = 53
• PR/CR: 43%
• median PFS: 11 months
• median OS: 28 months
Responses were seen across several non–clear cell histologies, with a particularly notable signal in FH-deficient RCC:
➡️ 7/8 patients had an objective response.
🔵 Why it matters
Non–clear cell RCC is not one disease.
Histology matters.
Biology matters.
And prospective treatment data remain limited.
This final analysis supports cabozantinib + nivolumab as an active regimen for selected patients with non–clear cell RCC histologies, especially papillary, FH-deficient, unclassified, and translocation-associated disease.
🟠 Safety
Toxicity was consistent with known cabozantinib + nivolumab profiles.
Grade 3/4 treatment-emergent AEs occurred in a substantial proportion of patients, and discontinuations due to AEs occurred with cabozantinib, nivolumab, or both.
So this is active therapy — but not low-burden therapy.
🧠 My take
CaboNivo is one of the more clinically useful prospective datasets in non–clear cell RCC.
The key message is not “treat all non–clear cell RCC the same.”
It is:
➡️ use histology
➡️ recognize biologic subgroups
➡️ avoid assuming clear-cell algorithms fully apply
➡️ consider CaboNivo as a treatment option where prospective evidence supports activity
➡️ continue building trials specific to rare RCC subtypes
For non–clear cell RCC, better classification is the beginning of better treatment.
#ASCO26 #GUOnc #KidneyCancer #RCC #NonClearCellRCC #PapillaryRCC #FHdeficientRCC #Cabozantinib #Nivolumab #PrecisionOncology
@OncLive@TargetedOnc@CancerNetwrk@ASCOPost@ecancer@VJOncology@curetoday@JCO_ASCO
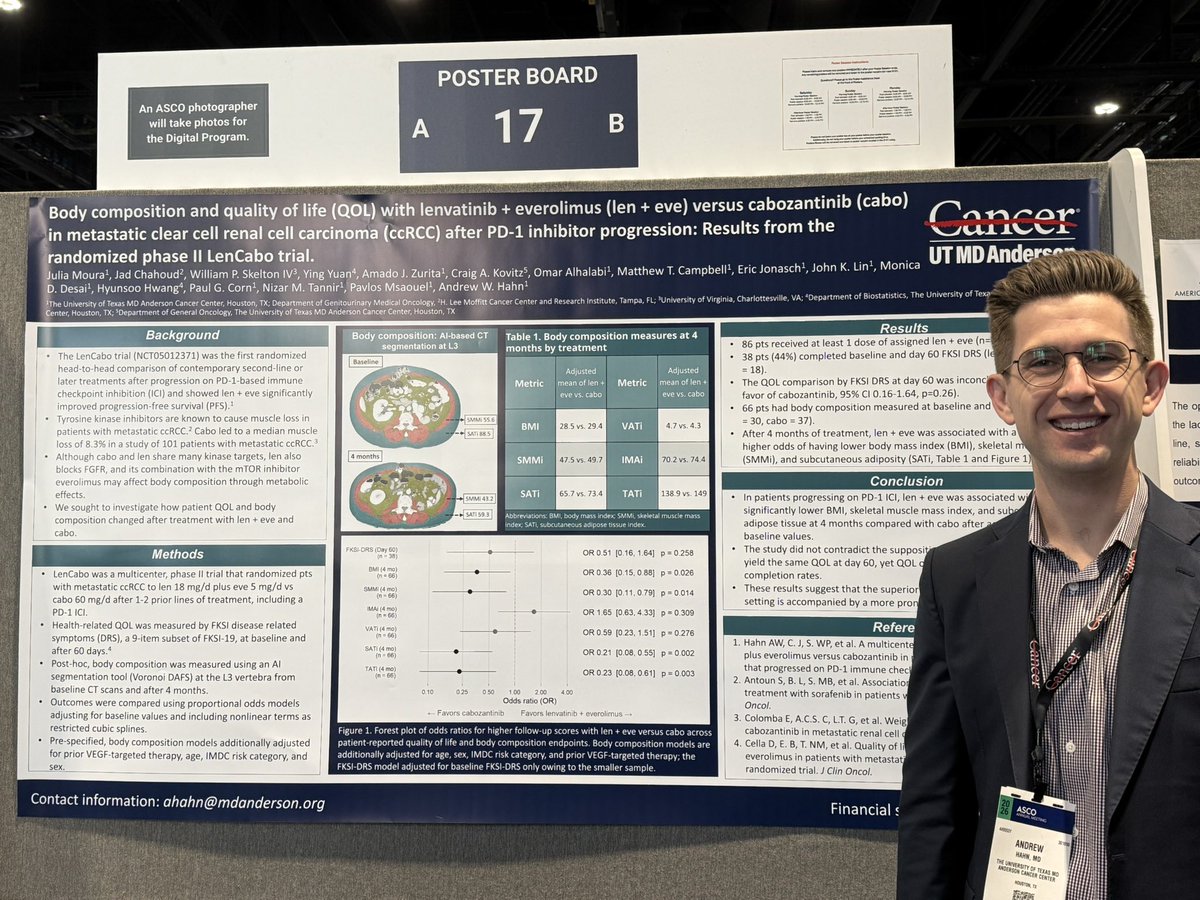
Does the PFS benefit of len + eve come with a body composition cost?
AI-based CT segmentation at L3 in post-IO ccRCC (phase II RCT, n=66):
After 4 months, len + eve associated with significantly greater losses in:
🔬 Skeletal muscle mass index: OR 0.30, p=0.014
🔬 Subcutaneous adiposity: OR 0.21, p=0.002
🔬 BMI: OR 0.36, p=0.026
QOL by FKSI-DRS was inconclusive between arms at day 60. Standard instruments may not capture what is happening at the tissue level.
AI-assisted CT phenotyping could be a new tool to understand treatment
Congrats @onchahn.
#RCC #KidneyCancer #GUonc #ASCO26
🟠#ASCO26 GU discussion
RCC with symptomatic bone metastases remains a difficult real-world scenario, especially where access to multidisciplinary bone care is variable.
📙Abstract 4500 | RADICAL
Cabozantinib ± radium-223 did not improve SSE-FS. @ASCO@DrRanaMcKay@urotoday
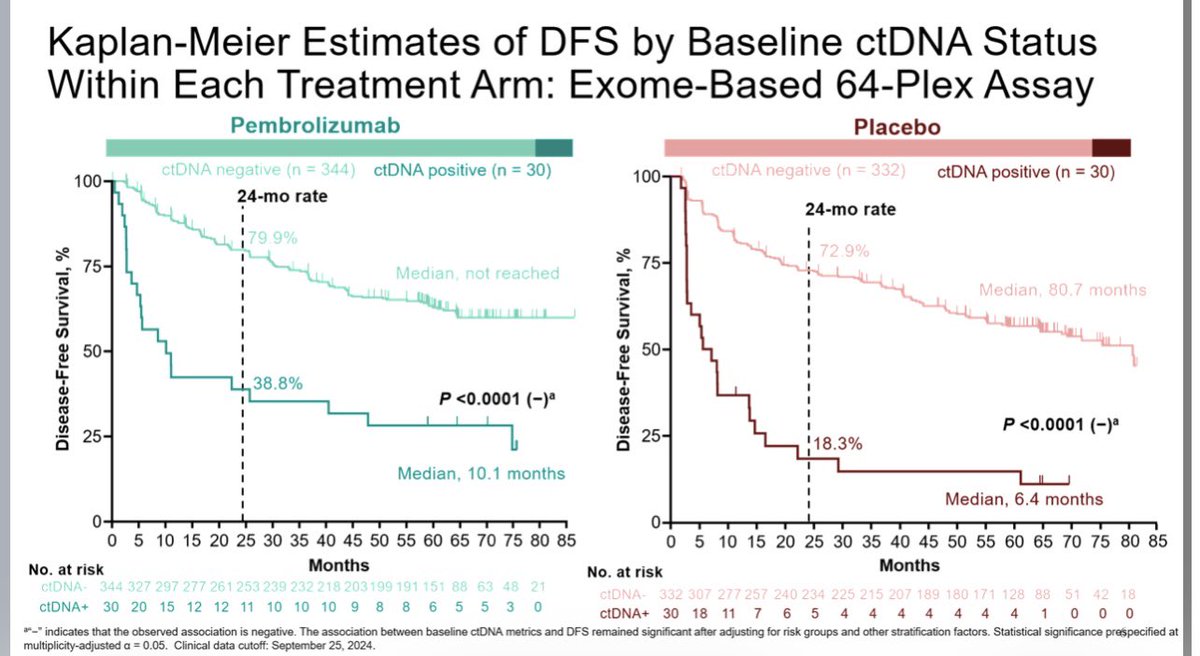
Clear cell RCC sheds low levels of ctDNA, but positivity and ctDNA dynamics are relevant in the adjuvant setting @DrChoueiri#ASCO26. This analysis is with an exome based personalised technique and shows a lack of sensitivity (5-8% ctDNA+ve rate vs 40% radiological relapse rate) but good specificity (almost all ctDNA +ves relapse). Whole genome ctDNA analysis should work work better. There is a future for ctDNA in renal cancer, we’re just not quite there yet IMO.
ctDNA in renal cell carcinoma: have we reached a turning point? Still many questions ahead — sensitivity, timing, clinical utility — but the field is clearly evolving fast. Great talk by @DrChoueiri#renalcellcarcinoma#ctDNA
We’re kicking off day one of #ASCO26 with @DrChoueiri highlighting ctDNA findings from the KEYNOTE-564 trial in kidney cancer, examining patients treated with adjuvant pembrolizumab or placebo after surgery.
First in class PD1/CTLA4 bispecific ph1 in nccRCC #ASCO26
➡️37 pts, ORR 51.6% esp in liver mets, mPFS 16.7 mo
⛔️ heterogeneity & high FH def population, no DLTs
✅promising 1L and manageable safety, not ready for clinic, but reinforces IO/TKI in nccRCC, driven by FH-def
PEAK-1: A randomized, double-blind, active-control, multicenter phase 3 trial of casdatifan and cabozantinib vs PBO and cabozantinib in patients with advanced clear cell #RCC. Upcoming poster presentation by @DrChoueiri@DanaFarber. #ASCO26 written coverage by @chavarriagaj@PSH_Urology > https://t.co/L6V29oTx8I @ASCO
⚡️ Phase 3 LITESPARK-022 in high-risk ccRCC after nephrectomy: adjuvant pembrolizumab + belzutifan vs pembrolizumab alone (n=1,841).
24-month DFS: 80.7% vs 73.7% (HR 0.72; P=0.0003).
First phase 3 adjuvant trial to demonstrate DFS benefit vs pembrolizumab monotherapy — a potential new standard of care.
#KidneyCancer
https://t.co/Y0gVbiAUDG
Renal cancer highlights #ASCO26 1) RAMPART - adjuvant durva/tremi vs durva vs surveillance. How much does CTLA4 help? 2) Is ctDNA useful post surgery in RCC (KN565 data)? 3) Does radium-223 help in bone mets patients? (a RII study) 4) Data on 2 VEGF+PD1 combination single arm studies in papillary RCC.
Looking forward to this #ASCO26 presentation by
@BethN01 addressing an important topic we see more and more in clinic: how patients perceive long-term toxicity and decision regret after adjuvant immunotherapy in RCC.
Finally published!!! 😃 The assessment of the Meet-URO score in a first-line mRCC international cohort. Thanks to @gbanna74@amg120395
https://t.co/abJQJ7S4h1
Do patients with bone metastases derive sustained benefit from first-line immunotherapy-based combinations in advanced RCC? #ASCO26@ASCO@apolo_andrea
Updated subgroup analyses from CheckMate-9ER and long-term outcomes with cabozantinib + nivolumab
https://t.co/p9S16JvnCy