Why do VEGFR-TKI + IO combinations produce impressive responses in ccRCC but often fail to achieve the long-term durability seen with dual checkpoint blockade? Check out our lab's latest in @Cancer_Cell led by the incredible Lyn Vuong!
https://t.co/ASvkCpDzQW
Panitumumab improves survival for patients with RMC, a rare and aggressive variant renal cancer. @PavlosMsaouel is advancing tx for RMC, inspiring! #ASCO26
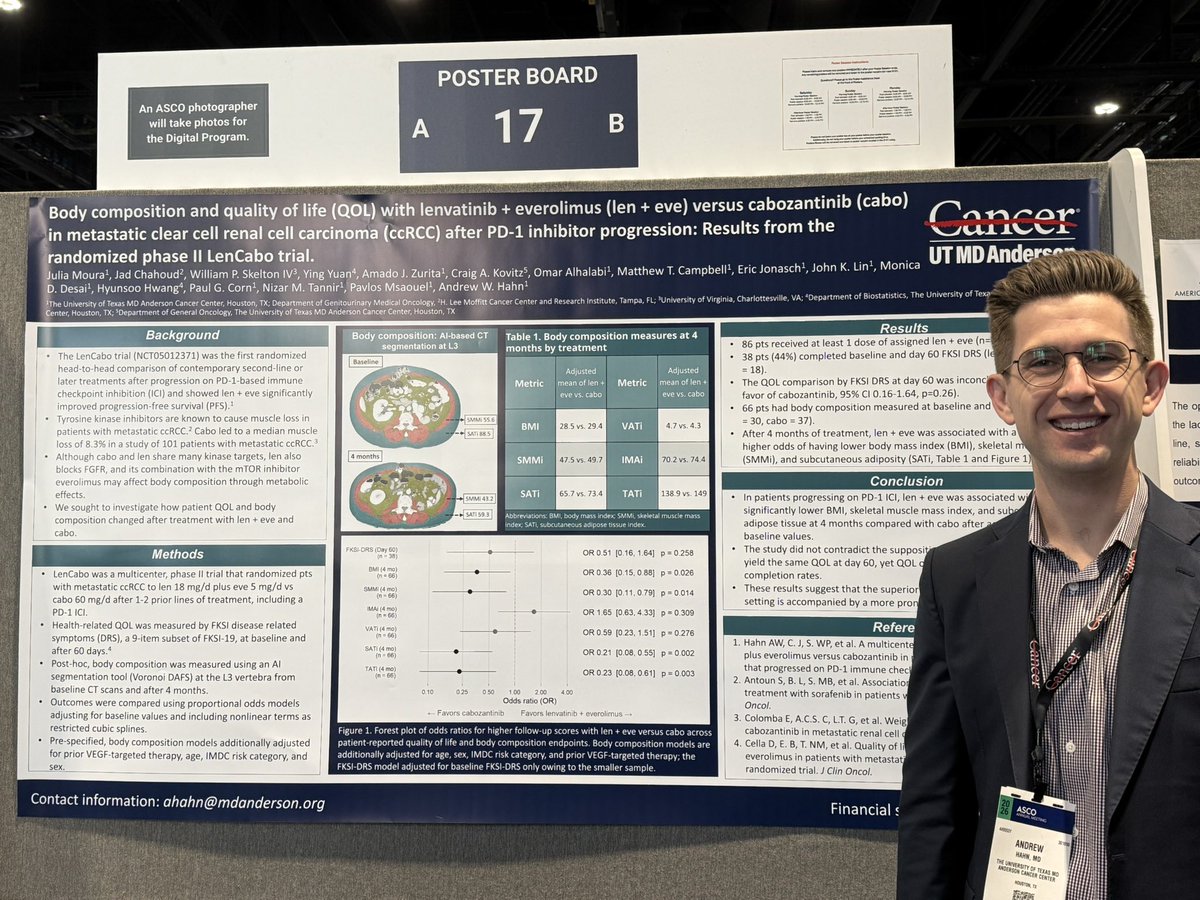
Thanks for highlighting our analysis of how muscle and fat changed between Len + Eve and Cabo in the phase 2 LenCabo trial @Uromigos Work led by @MourattJulia
Unsung hero poster award for RCC. @OncHahn discusses muscle and fat changes in patient receiving either Len/Ev or Cabo with some interesting findings that complement standard toxicity data.
Presented by Dr. Andrew Hahn at #ASCO26, an analysis from the phase II LenCabo trial found that lenvatinib plus everolimus was associated with greater reductions in body mass index, skeletal muscle mass and subcutaneous fat compared with cabozantinib in patients with metastatic clear cell renal cell carcinoma after PD-1 inhibitor progression. @OncHahn #EndCancer 6/7
Does the PFS benefit of len + eve come with a body composition cost?
AI-based CT segmentation at L3 in post-IO ccRCC (phase II RCT, n=66):
After 4 months, len + eve associated with significantly greater losses in:
🔬 Skeletal muscle mass index: OR 0.30, p=0.014
🔬 Subcutaneous adiposity: OR 0.21, p=0.002
🔬 BMI: OR 0.36, p=0.026
QOL by FKSI-DRS was inconclusive between arms at day 60. Standard instruments may not capture what is happening at the tissue level.
AI-assisted CT phenotyping could be a new tool to understand treatment
Congrats @onchahn.
#RCC #KidneyCancer #GUonc #ASCO26
Our outstanding post-doc @DrZachariahT presenting data on mediastinal GCT with somatic malignancy. A rare but difficult to treat entity, significantly enriched for sarcoma and p53 mut.
IM program directors be on the look out, he is a ⭐️!
A-DREAM asked a question patients actually care about: can favorable responders to ADT + ARPI safely take a break?
Single-arm phase 2 (Alliance A032101) in mHSPC. Eligible men had PSA <0.2 and suppressed testosterone after roughly 18 to 24 months on ADT + ARPI, then interrupted treatment.
Primary endpoint met:
🎯 41% (32/78) treatment-free with testosterone recovery at 18 mo (80% CI 33.5 to 48.9%, one-sided p=0.0249)
📊 67% (52/78) recovered eugonadal testosterone
📊 58% (45/78) remained treatment-free at 18 mo
📊 Median 24.5 mo off treatment, and 38.5% still off at 26.9 mo median follow-up
🔍 Low-volume disease and prior radiation to metastases predicted lower likelihood of needing to restart. Selection matters: these were patients and clinicians motivated to interrupt.
Defining the optimal intermittent strategy is the next question. Biomarker and PRO analyses pending.
Nicely done.
@AtishChoudhury #ProstateCA #mHSPC #GUonc #ASCO26
JUST In: TALAPRO-3 published in @NEJM
Adding #talazoparib to enzalutamide/ADT
=>3-year rPFS: 77% vs 56% in HRR-deficient metastatic prostate cancer !
Looking forward to full presentation by @neerajaiims who keeps changing SOC, one trial at a time.
@ASCO#ASCO26@OncoAlert
Great combo of presys by Dr. Mateo and @neerajaiims show ADT + enza + tala improves rPFS for APMS prostate cancer and how ADT + enza induces transcriptome changes but not HRD
Abstr. 5001. ENZAMET: Can Decipher GC (DGC) help move triplet selection in mCSPC beyond disease volume alone? @ChrisSweens1
634 pts
ADT + Enza: DGC >0.85 DGC had worse OS
ADT+ Enza + Docetaxel: adverse high-DGC signal attenuated with addition of docetaxel
No clear docetaxel benefit with DGC ≤0.85.
Implication: In a front-line mCSPC landscape where triplet therapy is still largely selected by high-volume disease on conventional imaging, this supports a shift toward prospective study of biology-informed approaches. In parallel, TRIPLE-SWITCH (SWOG-CCTG PR26) is testing a response-adapted intensification approach by adding docetaxel to pts with suboptimal PSA response to ADT + ARPI alone. @SWOG@sokolova_md@OncHahn@YuWeiChenMD@PCF_Science@JoshLangMD@DrRanaMcKay@urotoday@neerajaiims@MikeSerzanMD@scocmem@nataliagandur@OncoAlert
Cardiovascular prevention in #prostatecancer needs tools that actually fit oncology workflows.
We built + externally validated PC-specific risk scores for ASCVD, heart failure, and CVD using variables already available in cancer clinics. Introducing the GUHA-STABELLINI score
Congrats @AtishChoudhury 👉Can we safely de-intensify Rx in exceptional responders with mHSPC/ mAPMS #prostatecancer ? #ASCO2026 A-DREAM data👉Rx holiday after ADT + ARPI may be feasible, with 41% remaining treatment-free with testosterone recovery at 18 mos @OncoAlert@urotoday
Abstr. 4500. RADICAL/A031801: Does adding Radium-223 to cabo in pts with RCC + symptomatic bone mets improve SSE-free survival (SSE-FS)?
Median SSE-FS 17.9 vs 17.6 mo. ORR ~22% in both arms. PFS 11.0 vs 11.2 mo. Trial stopped early for futility. Radium-223 + cabo did not improve SSE-FS vs cabo alone.
Implications: In RCC bone mets, bone-seeking radioligands may be insufficient. CAIX-targeted radioligand therapies in combination +/- TKI-IO therapy may be more promising ➡️ongoing STARLITE-1, STARLITE-2, & LUTEON trials examining ¹⁷⁷Lu-girentuximab (TLX250), a CAIX-targeted radioligand, in various advanced ccRCC settings.
Congratulations to @DrRanaMcKay, the study team, & @ALLIANCE on their perseverance in conducting this trial. @OncoAlert@KidneyCancer@kidneycan@scocmem@nataliagandur #kcsm #ASCO26
Further evidence that more sensitive WGS-based assays capable of low ppm detection (used, eg, here: https://t.co/sPGnH5yJ7s and https://t.co/JwKq4gq1Rr) are needed to resolve the low TMB by exome and low ctDNA shedding challenges in clear cell #kidneycancer.
Sat. 3-3:30 p.m.
Kidney cancer treatment continues to evolve through innovation and research. At #ASCO26, Drs. Eric Jonasch, Pavlos Msaouel and Andrew Hahn will discuss advances shaping care today.
Stop by booth 13109 to join the discussion. @PavlosMsaouel and @OncHahn #EndCancer 9/11