@ryanAjoyce@GregLehman Interesting that zones 4-5 have almost no effect. So for those that don’t have enough time to train like elites and resort to higher intensities as a replacement and thinking they are improving aerobically , that may not work well.
We glorify Zones 4 and 5.
But your heart might not care.
Low-intensity, longer duration work in Zones 1 and 2 drives the most cardiac adaptation... not the hard stuff.
@guido_claessen@PaulBLaursen
-
📄 Dausin et al., European Heart Journal (2026)
-
🎙️ https://t.co/rm9CqHz5G7
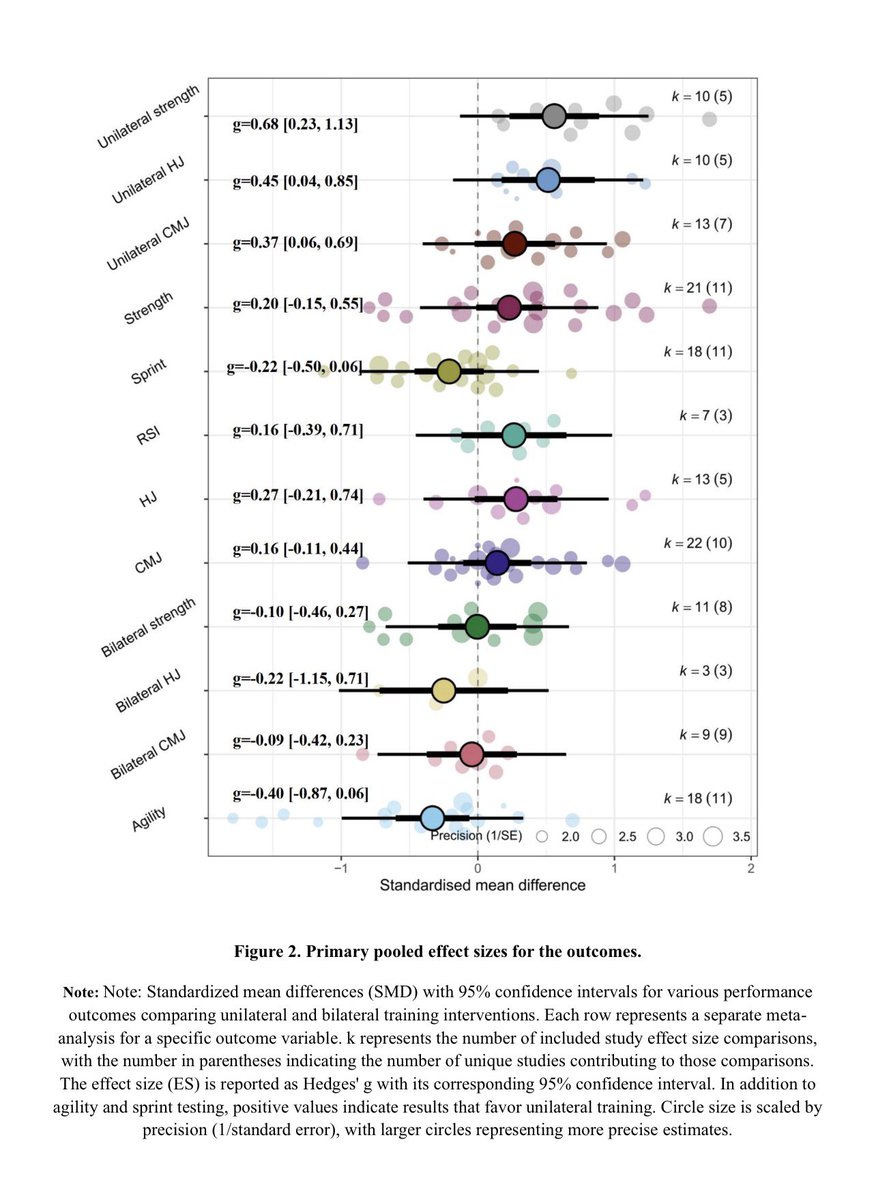
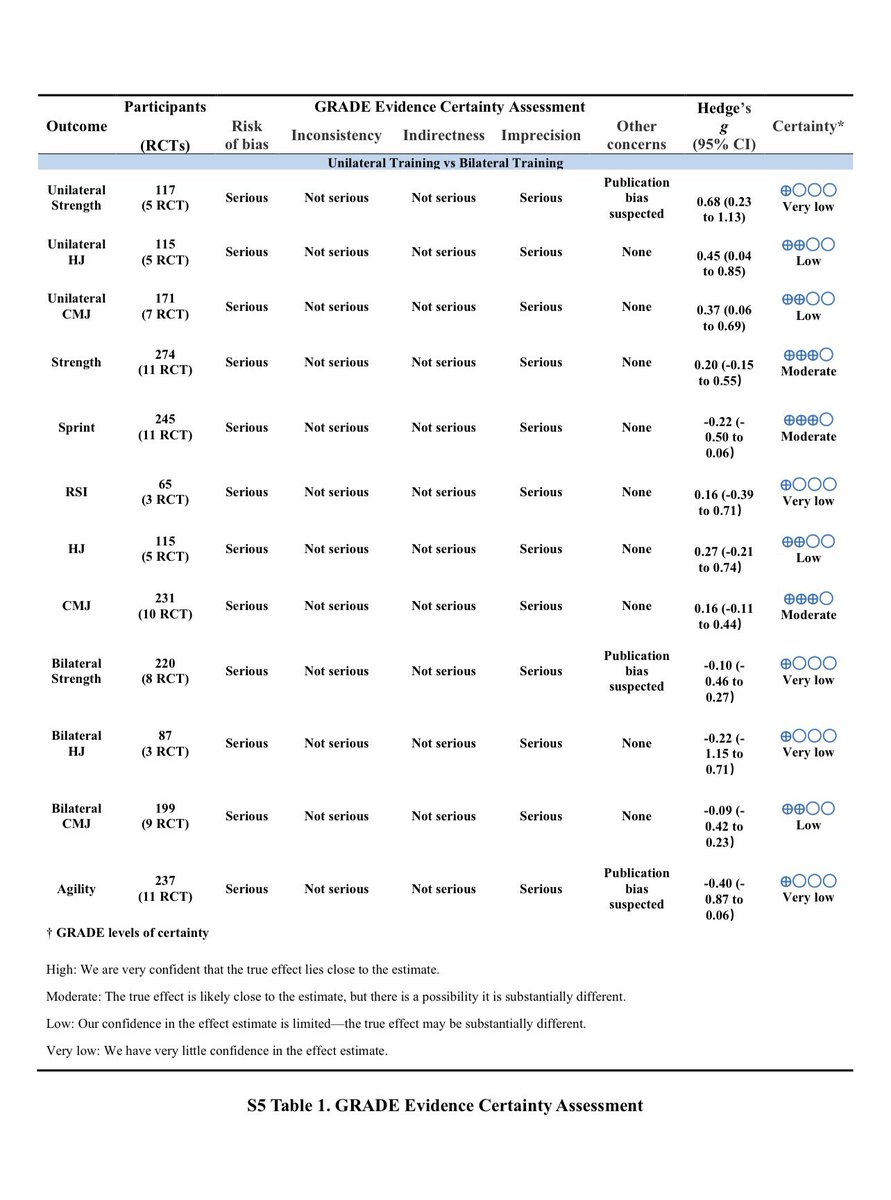
📄 Effects of Unilateral vs. Bilateral Training on Performance Measures in Team Sport Athletes — just accepted in Biology of Sport.
🔗 Link to accepted version on RG: https://t.co/eFtLWdrRkH.
@popeyecubs68@KBurola Neither intensity nor duration influenced risk of ventricular arrhythmia uniquely. In other words a high- or low-intensity session elevated risk similarly in the ensuing 24h.
@andrew_flatt@hjluks@MikeDPhysio Sorry, I should have been more clear.
With HIIT heart raises and lowers during the intervals, and resistance training has a similar effect.
Why Early Loading Heals Tendons Faster Than Rest
For many years, tendon injuries were initially managed with rest... or ice for a few days, followed by time in a brace or a boot. Pain was taken as a signal to avoid load, and recovery was expected to occur with time.
Mechanical stress was viewed as something to delay until symptoms settled.
Research from Denmark has shown that this approach is wrong.
Much of this work comes from the Copenhagen muscle and tendon research community, particularly from groups led by Michael Kjaer at the University of Copenhagen and collaborators at Bispebjerg Hospital, as well as from clinical research by Håkan Alfredson. Their combined laboratory and clinical studies have clarified how tendons respond to injury and recover function.
In several controlled studies, including work on Achilles and patellar tendon injuries, researchers compared outcomes between early, structured loading and delayed loading following a period of rest.
When controlled loading was introduced within the first few days after injury—often around day two—return to function occurred far sooner than when loading was delayed until day seven to nine, or later. Some papers reported that athletes in the early mobilization group were back 25% sooner than those in the delayed group.
Tendons are mechanosensitive tissues. Mechanical strain activates tendon fibroblasts through integrin-based signaling, leading to intracellular pathways such as MAP kinase activation that stimulate collagen synthesis and alignment. This process is necessary for restoring tendon alignment, stiffness, and load tolerance. When tendons are unloaded for prolonged periods, collagen remodeling is reduced, and structural organization worsens.
Rest can reduce pain, but it does not restore tendon capacity. In fact, prolonged unloading leads to decreased tensile strength and increased sensitivity to load reintroduction.
The worst thing we can do is to brace or boot these injuries for a period of time.
The tendon may feel better temporarily, but it is often less prepared to tolerate stress. The benefit of early loading depends on how the load is applied. The Danish studies emphasized controlled, progressive loading rather than a return to unrestricted sport. Early loading typically involved isometric or slow resistance exercises rather than elastic or high-velocity strain. The goal was to provide a mechanical stimulus sufficient to promote remodeling without provoking excessive irritability.
This distinction is important. Early loading does not mean ignoring pain or continuing normal training. It means modifying the load rather than eliminating it. In real life, that often means starting isometric exercises of a short duration… and progressing as comfort improves.
Clinically, this helps explain why many tendon injuries take longer to recover. Symptoms may improve with rest, but when activity is resumed, pain returns, and the cycle repeats. Tendon capacity was never rebuilt.
The work from the Copenhagen tendon research groups supports a different approach: tendons recover best when they are exposed early to appropriate mechanical loads adjusted to tissue tolerance (pain).
Tendons do not recover in a brace over time. They recover through progressive mechanical loading applied early enough to influence remodeling.
@JimGalanes@nick_krontiris Not sure if you had a chance to read this paper but was curious on your take of this study. I am struggling with intensity not being able to remodel ?