Surgical oncologist | Gastrointestinal tumors
Liver, pancreas & biliary tract cancer
Head of GI Tumors Dept, National Cancer Institute of Mexico (@incanMX)
Quality in Surgery: Concepts, Measurement, Advances and Strategies for Improvement.
@mtzsaid@charlesbalchmd@DorianGarciaMD la calidad no depende únicamente de la habilidad técnica del cirujano, sino del funcionamiento integral del sistema de salud. https://t.co/LhMuHGDUW5
15 millones de cirugías oncológicas al año en el mundo
20% complicaciones postoperatorias en de los cirugías mayores, un % importante se debe a fallas del sistema más que a errores técnicos
Este articulo propone evolucionar de una visión tradicional en mortalidad y complicaciones hacia un “Learning Health System” quirúrgico, donde los datos se utilicen para rediseñar procesos, mejorar resultados, reducir inequidades y generar valor para los pacientes
@GABOUALFA presents #EMERALD-3 phase 3 study of #TACE#STRIDE +/- #lenvatinib in patients with embolization eligible #HCC. Waiting for more data/longer follow up, a potential new option for our patients @asco
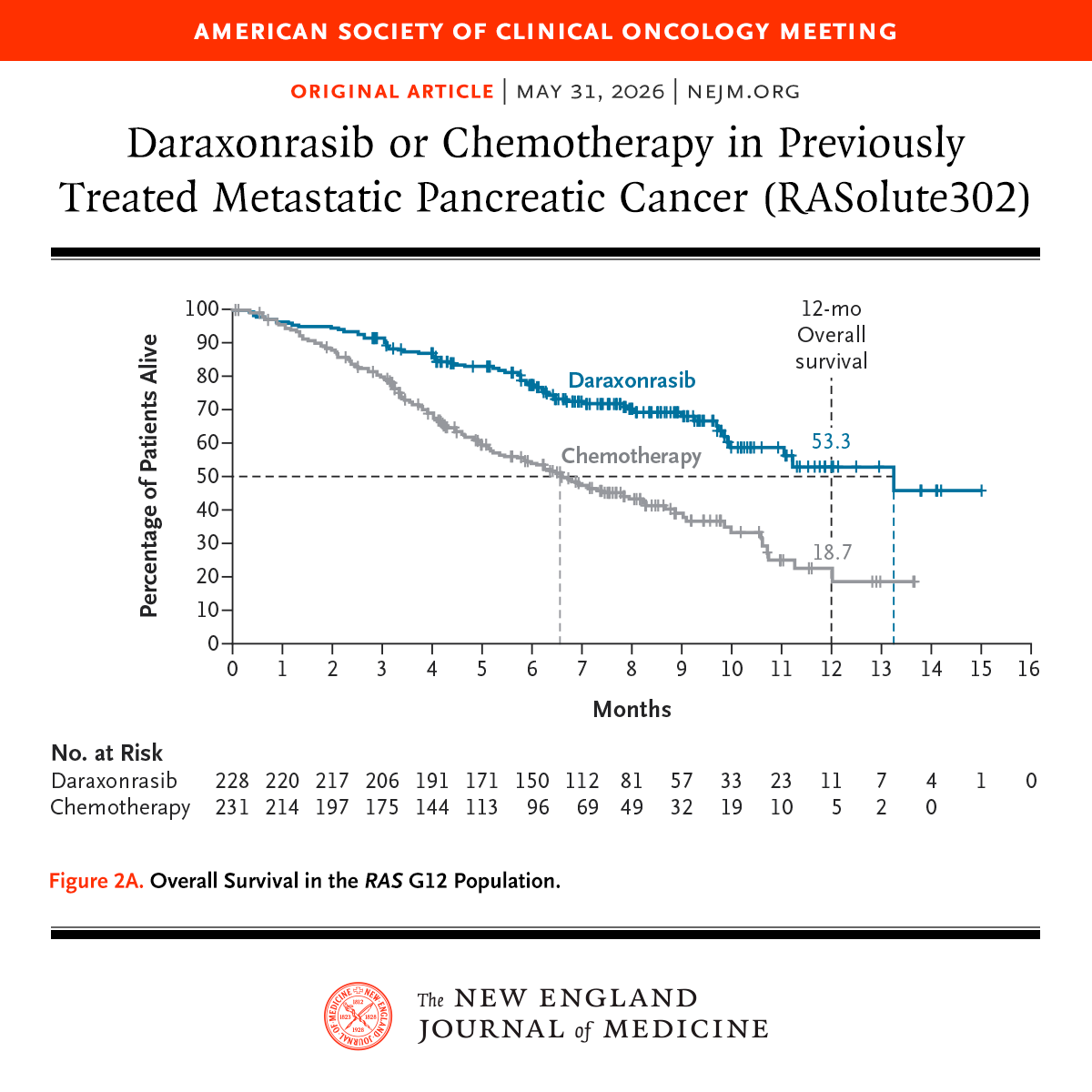
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
#ASCO2026| RASolute 302 marca un posible antes y después en cáncer de páncreas metastásico. Daraxonrasib demostró superioridad frente a quimioterapia en 2ª línea, con mejor supervivencia global, mejor supervivencia libre de progresión y menor toxicidad. #vaporti#cancerdepancreas
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
1/n
Daraxonrasib (RMC-6236), the first-in-human oral 💊RAS(ON) multi-selective tri-complex inhibitor, in previously treated RAS-mutated pancreatic cancer phase I/II study is now published in the New England Journal of Medicine @NEJM
A novel💡 way to shut down ⚔️RAS, one of the most important oncogenic drivers in cancer that had long been considered “undruggable.”
🔗https://t.co/ptfNVcxrb4
Shout out to Brian Wolpin, @CentralParkWMD@GarridoLagunaMD@AlexSpiraMDPhD@salmanpunekar@MeredithPelster@bherzbergmd Nilo Azad Aparna Hegde @DavidHongMD and the whole team who dedicated to this study. @EileenMOReilly
#HBP #HumansBeyondPatients
Pancreatic cancer has one of the most suppressive tumor microenvironments in oncology.
But two pancreatic cancer results dropped today. Both matter.
1. BioNTech mRNA neoantigen vaccine: nearly all responders still alive at 6 years. 98% of induced T cells were de novo — the immune system learned to see a cancer it had always been blind to.
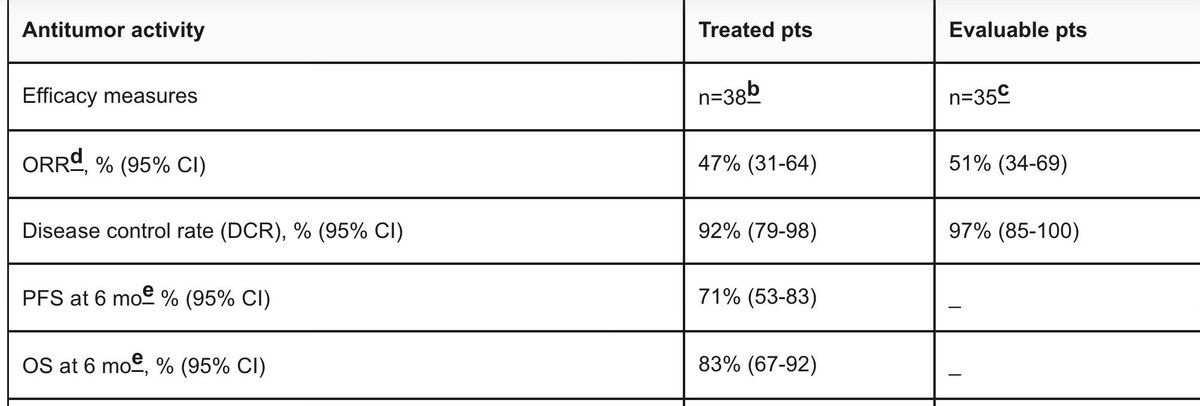
2. Daraxonrasib: 47% ORR, 92% disease control as first-line monotherapy. KRAS G12D, undruggable for 40 years, finally has a drug.
Different mechanisms. Same disease. Both working.
<13% of patients survive 5 years. That number is about to change.
great day for science! 🔥
A Mayo Clinic-developed artificial intelligence (AI) model can help specialists detect pancreatic cancer on routine abdominal CT scans up to three years before clinical diagnosis. It identifies subtle signs of disease before tumors are visible, when curative treatment may still be possible. The findings, published in Gut, mark a milestone in Mayo Clinic's multiyear research effort to enable earlier detection of one of the deadliest cancers.
Learn more: https://t.co/EJySSkaW3P
Nuestro especialista, el Dr. Javier Melchor Ruan, participó en La Hora Nacional hablando sobre cáncer colorrectal.
Te invitamos a escuchar su intervención y conocer información clave sobre prevención, detección oportuna y tratamiento.
¡Infórmate y comparte!
¿Sabías qué?🤔
El cáncer de colon es altamente curable si se detecta a tiempo mediante pruebas de cribado como la colonoscopia.
🎥Este próximo domingo en nuestro programa nos acompañará el Dr. Javier Melchor Ruán, cirujano oncólogo y jefe del Departamento de Gastroenterología del Instituto Nacional de Cancerología, quien nos explicará cómo prevenir esta enfermedad, cuidados y tratamientos.👨🏻⚕️
✅️Infórmate mañana a las 10 de la noche. 📺
Adjuvant chemotherapy works in colorectal cancer… right? 🤔
When it comes to resectable colorectal liver metastases, the answer may be more complicated than we like to admit.
JCOG0603 was the first randomized trial to test adjuvant doublet chemotherapy after hepatectomy in CRLM. The headline result was familiar: adjuvant mFOLFOX6 improved disease free survival. But with long term follow up, overall survival has told a different story. There was no OS benefit compared with surgery alone, despite years of additional follow up. This mirrors what we have already seen with EORTC 40983 and New EPOC.
Why the disconnect?
• The trial was powered for DFS, not OS
• Oxaliplatin alters liver parenchyma, making CT based DFS a potentially unreliable surrogate
• Patients in the surgery only arm had more effective salvage surgery and greater reuse of oxaliplatin at recurrence
• Toxicity mattered, with high rates of severe neutropenia, poor chemotherapy completion, and even rare treatment related death
The bigger lesson is uncomfortable but important. In resectable colorectal liver metastases, delaying radiographic recurrence does not necessarily translate into living longer or living better. Post recurrence management, surgical salvage, and tumor biology may matter far more than perioperative chemotherapy intensity.
For me, this argues against routine adjuvant mFOLFOX after hepatectomy and toward more selective, biology driven decision making 🧬
At the same time, this is not an easy “don’t treat” scenario. We lack clearly superior alternatives, and choosing not to give systemic therapy in a high risk disease is hard for clinicians and patients alike.
If anything, JCOG0603 highlights the real unmet need in CRLM: better studies, better biomarkers, and better drugs. This disease keeps surprising us, and this is one of the most important reminders why.
@OncoAlert@TheGutOncLab
https://t.co/dbCFtf1Zft
🆕 Article in @JCO_ASCO
🚨 Adjuvant mFOLFOX6 after hepatectomy for colorectal liver metastases – JCOG0603 long-term OS results 🚨
📚 Randomized Phase II/III trial
👥 300 patients with colorectal adenocarcinoma and liver-only metastases (unlimited number)
💊 Adjuvant mFOLFOX6 after hepatectomy
⚖️ Hepatectomy alone
⏳ Median follow-up: 7.7 years for disease-free survivors
📊 Results:
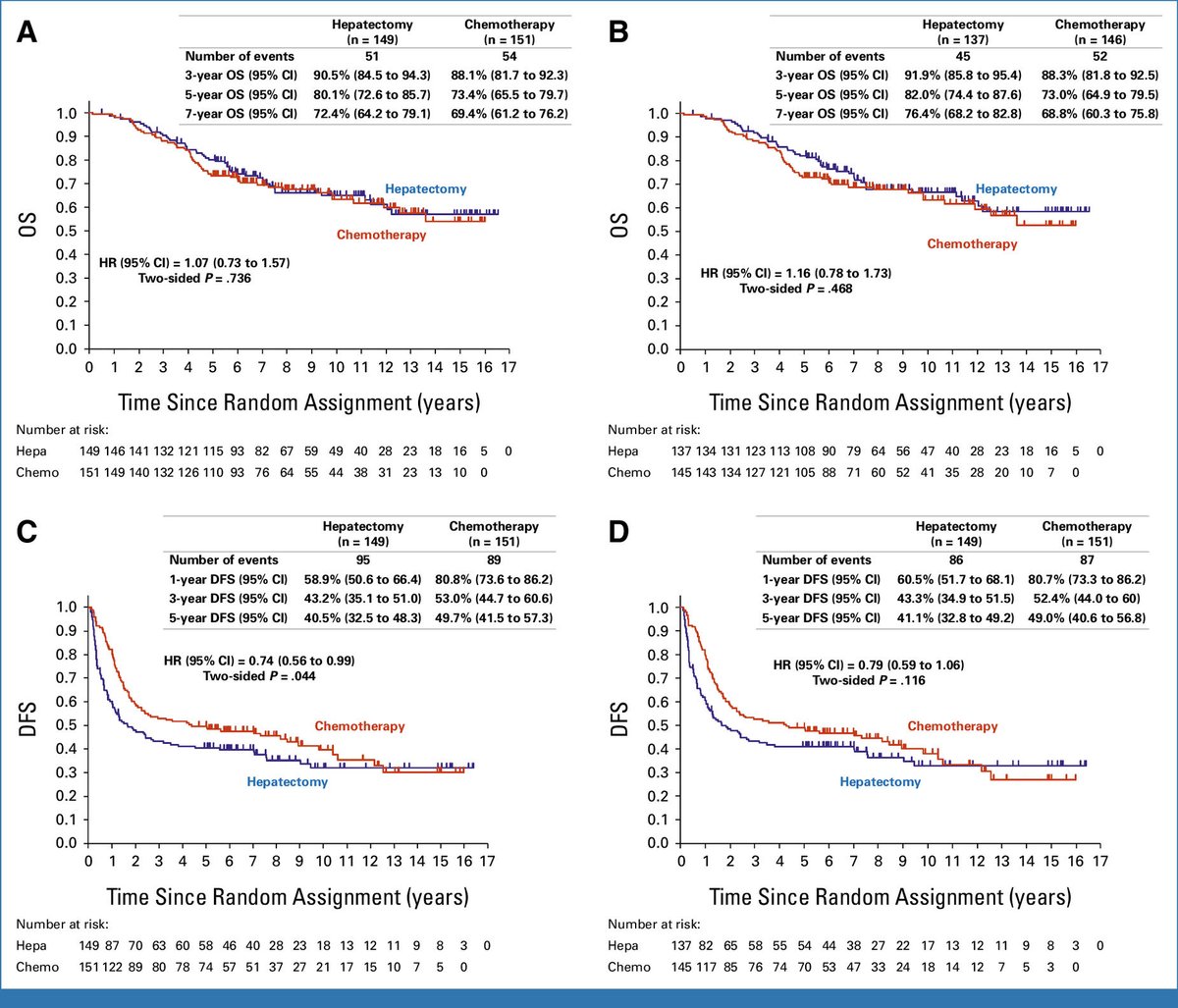
📈 5-year DFS: 49.7% (adjuvant chemo) vs 40.5% (surgery alone)
📉 DFS HR = 0.72 (95% CI, 0.54 to 0.97) ✅
📈 5-year OS: 73.4% (adjuvant chemo) vs 80.1% (surgery alone)
📉 OS HR = 1.07 (95% CI, 0.73 to 1.57) ❌
⚠️ Toxicity: One possible treatment-related death in adjuvant arm; one post-protocol complication death in surgery arm.
💡 Adjuvant mFOLFOX6 improved DFS but did not translate into a long-term overall survival benefit.
#ColorectalCancer #LiverMetastases #Hepatectomy #AdjuvantChemotherapy #mFOLFOX6 #MedTwitter #PubXelProject
PMID:41564372
https://t.co/RZjJCXXppE
This commentary observes that the disappearance of colorectal liver metastases on imaging does not reliably signify nonviability, emphasizing the need for cautious patient management and advanced diagnostic tools. https://t.co/snTF7iahf7